
Abstract
Background:
Gastrocnemius tightness has been implicated in the pathogenesis of calcified insertional Achilles tendinopathy (IAT), Haglund deformity, and Achilles intratendinous calcifications (IC). The aims of this study were to determine long-term clinical and radiographic results of combined proximal medial gastrocnemius release (PMGR) and Achilles tendon debridement and reattachment (ATDR) for patients presenting with symptomatic calcified IAT.
Methods:
A retrospective cohort study was performed in order to determine clinical and radiographic outcomes of PMGR and ATDR for patients presenting with symptomatic calcified IAT, at a minimum follow-up of 30 months. Patient satisfaction was assessed at last available follow-up as very satisfied, satisfied, and unsatisfied. Clinical assessment was performed evaluating preoperative and last available follow-up visual analog scale for pain (VAS-P) and the Foot and Ankle Outcome Score (FAOS). Radiographic evaluation included Fowler-Phillip angle, calcification length, calcification width, and presence of Achilles IC, measured on standard weightbearing lateral calibrated radiograph of the foot preoperatively and last available follow-up evaluation for each patient.
Results:
The mean follow-up was 46 (range, 30-72) months. We registered 45 “very satisfied” patients (84.91%), 6 “satisfied” patients (11.32%), and 2 “unsatisfied” patients (3.77%), as well as statistically significant improvement on both clinical scores tested. We found statistically significant differences between the initial evaluation and last available follow-up on all radiographic measurements. There was no significant radiographic recurrence of calcified IAT, whereas minor Achilles intratendinous calcifications were found in 10 patients (18.87%).
Conclusion:
Combined PMGR and ATDR provides significant clinical and radiographic improvement for patients presenting with symptomatic calcified IAT and, although not preventing radiographic recurrence of minor Achilles IC, may reduce the rate of radiographic recurrence of calcified IAT, though the lack of a control group limits causal inference.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
Chronic insertional Achilles tendinopathy (IAT) is a debilitating condition, leading to progressive pain, swelling and tenderness around the Achilles tendon insertion to the posterior calcaneus, and can frequently be associated with Haglund deformity and Achilles intratendinous calcifications (IC).6,14 –16 Gastrocnemius tightness, which can be clinically assessed by the Silfverskiöld test, has been implicated in IAT pathogenesis, together with extrinsic or intrinsic factors as excessive loading of the Achilles tendon, progressive aging and systemic conditions as obesity, dyslipidemia, or hypertension.4,7,18 –20,22
Proximal medial gastrocnemius release (PMGR) is probably the least invasive option when considering triceps surae lengthening procedures and has been proven as a useful procedure in recalcitrant Achilles tendinopathy.1,2,10,13 Instead, when dealing with symptomatic calcified IAT, Haglund deformity, and Achilles IC, there is a relative consensus on complete tendon debridement, calcaneal exostectomy, removal of the calcification and tendon reinsertion through a central splitting approach of the Achilles tendon, which can be abridged to Achilles tendon debridement and reinsertion (ATDR).5,8,9,12,17,21,23 ATDR was found to be clinically effective, although radiographic recurrence rates of calcified IAT range between 21% and 50% on previous reports.8,17
The aims of this study were to determine long-term clinical and radiographic results of combined PMGR and ATDR for patients presenting with symptomatic calcified IAT, as well as its possible effect on recurrence of calcified IAT. We hypothesized that this technique would demonstrate and maintain improvement in clinical and radiographic parameters in the long term, particularly by acting on gastrocnemius tightness and this way preventing the recurrence of calcified IAT.
Materials and Methods
Study Design
A retrospective cohort study analyzing clinical and radiographic results of a consecutive series of patients presenting with symptomatic calcified IAT who underwent combined PMGR and ATDR between January 2017 and May 2022 was carried out at the first author’s institution. The protocol was in accordance with the ethical standards of the first author’s institutional Ethics Committee, as well as with the Declaration of Helsinki and the Guidelines for Good Clinical Practice. Written informed consent was obtained from all patients enrolled. Demographic data was collected, including gender, laterality and age (Table 1). The minimum follow-up was 30 months.
Patient Demographics.
Inclusion criteria were as follows: (1) patients presenting with pain, swelling, and tenderness around the Achilles tendon insertion to the posterior heel, as well as a positive Silfverskiöld test, demonstrating gastrocnemius tightness4,20; (2) patients with radiographic criteria for calcified IAT6,16; and (3) patients who had previously received conservative treatment with eccentric exercises, physical therapy, and analgesic medication for at least 6 months without subjective pain relief.
Exclusion criteria included patients with previous surgery or requiring concomitant surgical procedures of the foot or ankle, neuromuscular disease, peripheral vascular disease, uncontrolled diabetes mellitus and acute infection. All patients without pre- and postoperative calibrated radiographs were also excluded.
Clinical Analysis
Patient satisfaction was assessed at last available follow-up as very satisfied, satisfied, and unsatisfied. Clinical assessment was performed evaluating preoperative and last available follow-up visual analog scale for pain (VAS-P) and the Foot and Ankle Outcome Score (FAOS).3,11 All clinical questionnaires were administered by 2 of the coauthors and 2 independent research associates.
Assessment of potential complications was performed, including wound healing problems, revision surgery, neurovascular damage, or thromboembolic event.
Radiographic Analysis
Standard weightbearing anteroposterior, lateral, and long axial view calibrated radiographs of the foot and ankle were taken preoperatively and last available follow-up evaluation available for each patient. Radiographic evaluation included Fowler-Phillip angle, calcification length, calcification width, and presence of Achilles IC, measured on standard weightbearing lateral calibrated radiograph of the foot preoperatively and last available follow-up evaluation for each patient (Figure 1).6,16 All radiographs were evaluated by 2 of the coauthors and 2 independent research associates.

Standard weightbearing lateral radiographs demonstrating a left foot calcified insertional Achilles tendinosis. (A) Calcification length of 19.57 mm. (B) Calcification width of 11.43 mm. (C and D) Progression of the Fowler-Phillip angle from preoperative 65 to 47 degrees at the last available follow-up evaluation.
Operative Technique
A combination of spinal anesthesia and popliteal sciatic nerve block was used. Patients were placed in prone position with a sandbag under the contralateral hip to allow internal rotation of the operated leg. The ankle joint was left free at the end of the table and the operated leg was placed over a pad in order to relax the gastrocnemius and to allow full dorsiflexion of the ankle joint. After exsanguination with an Esmarch bandage, a tight tourniquet was placed.
PMGR was performed first. A posteromedial incision of approximately 3 cm was performed around 1 cm distal to the posterior knee crease. After retraction of the subcutaneous fat, the crural fascia was sectioned in line with the incision and the proximal insertion of the medial gastrocnemius was identified. After cutting all the white fibers, the ankle was forced into full dorsiflexion, allowing for complete lengthening of the muscle fibers.
Subsequently, a longitudinal incision was made over the Achilles tendon, starting 2 cm proximal to its insertion and extending around 4 cm over the posterior calcaneus. After performing a full-thickness incision centered on the Achilles tendon, a small surgical retractor was placed (Figure 2A). The calcaneus was then exposed by gently stripping the medial and lateral lips of the Achilles tendon insertion. All the intratendinous calcifications were carefully excised and a complete debridement of the unhealthy tendon was performed, with care not to exceed 50% of the tendon width. Subsequently, a calcaneal exostectomy was performed using a combination of microsagittal saw, osteotomes, and rongeurs in a controlled manner (Figure 2B). Finally, we reinserted the Achilles tendon on the posterocentral calcaneus using a 3.5-mm titanium suture anchor (Figure 2C). After stepwise wound closure and placement of adequate surgical dressings, a walking boot was applied with the ankle in a neutral position.

The central tendon-splitting approach for left foot calcified insertional Achilles tendinosis. (A) Placement of small retractor, after full-thickness longitudinal incision of the Achilles tendon. (B) Performing calcaneal exostectomy with a microsagittal saw and removing intratendinous calcifications with rongeur. (C) Placing a 3.5-mm titanium suture anchor on the posterocentral calcaneus.
Postoperative Regimen and Follow-Up
All patients were discharged the day after surgery. Analgesic medication and anticoagulation were prescribed for 2 weeks. After a period of partial weightbearing with walking boot and crutches for 6 weeks, if significant clinical improvement was observed, together with radiographic evidence of correct placement of the suture anchor, patients were allowed to remove the walking boot, gradually increase weightbearing on the operated foot, and start physiotherapy. We proceeded with clinical and radiographic evaluation at 3 months, 6 months, 1 year, and then on scheduled annual appointments.
Statistical Analysis
Data analysis and statistical tests were performed using GraphPad Prism, version 10.0.0 for Windows (GraphPad Software, Boston, MA). Results were presented as mean ± SD. Wilcoxon matched pairs was used to compare preoperative and last available follow-up clinical scores (VAS and FAOS), Fowler-Philip angle, calcification length, and calcification width measurements. A P value under .05 was considered statistically significant.
Results
Patient Demographics
Demographic data are depicted on Table 1. The mean follow-up was 46 (range, 30-72) months. No patient was lost during follow-up.
Clinical Outcomes
We registered 45 very satisfied patients (84.91%), 6 satisfied patients (11.32%), and 2 unsatisfied patients (3.77%), as well as statistically significant improvement on both clinical scores tested (P < .05) (Table 2). We found statistically significant differences between the last follow-up and the initial evaluation on all clinical scores (P < .0001) (Table 2). VAS-P score progressed from 8.77 ± 1.10 (range, 7-10) preoperatively to 1.40 ± 1.39 (range, 0-6) at last follow-up (P = .011). FAOS score progressed from 42.98 ± 8.95 (range, 28-64) preoperatively to 85.66 ± 6.24 (range, 68-96) at last follow-up (P < .0001).
Comparison Between Preoperative and Last Available Follow-Up Clinical Scores.

Abbreviations: FAOS, Foot and Ankle Outcome Score; VAS-P, visual analog scale for pain.
Radiographic Outcomes
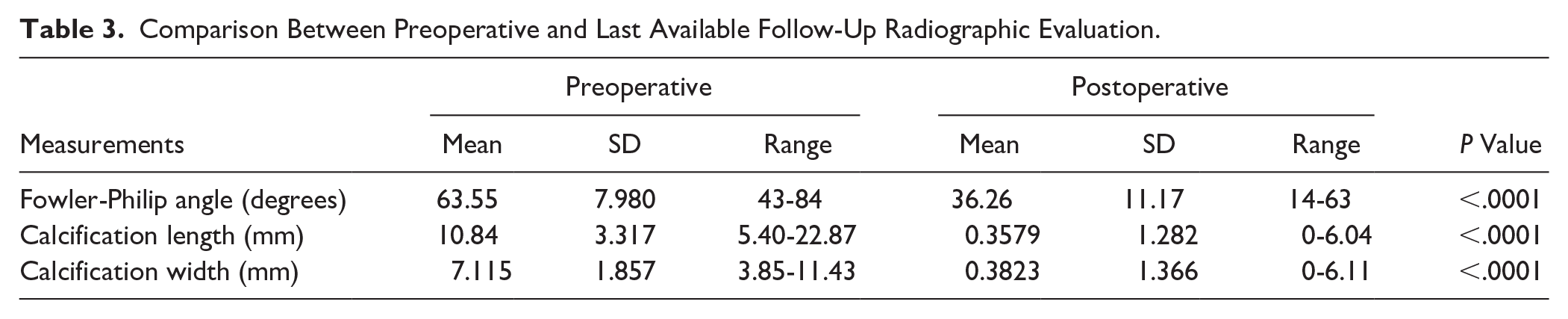
We found statistically significant differences between the initial evaluation and last available follow-up on all radiographic measurements (Table 3). There was no significant radiographic recurrence of calcified IAT. We found recurrence of minor Achilles IC on 10 patients (18.87%) (Figure 3). The differences between the measurements made by the different authors and independent research associates were not statistically significant.
Comparison Between Preoperative and Last Available Follow-Up Radiographic Evaluation.

Standard weightbearing lateral radiographs depicting right foot calcified insertional Achilles tendinosis. (A) White arrow pointing to preoperative minor Achilles intradeninous calcification. (B) Short-term follow-up evaluation demonstrating complete removal of Achilles intratendinous calcification and large insertional calcification. (C) White arrow pointing to more considerable Achilles intratendinous calcification at 42-month postoperative follow-up evaluation.
Complications
During follow-up, we registered 3 cases (5.67%) of superficial wound dehiscence, 2 concerning the PMGR (3.77%), and 1 the ATDR (1.89%), all healing with local wound care. One patient (1.89%) required revision surgery, due to local irritation caused by suture threads originating from the suture anchor. After removal of the suture anchor, the symptoms resolved. Another patient (1.89%) presented with radiographic signs of extrusion of the suture anchor 6 weeks postoperatively. Magnetic resonance evaluation revealed no tendon discontinuity, the Thompson test was normal and the patient asymptomatic, so no revision surgery was necessary. We also registered 1 case (1.89%) of deep vein thrombosis. There was no case of deep infection or neurovascular damage.
Discussion
The essential findings of this study were that the combination of PMGR and ATDR was associated with statistically significant clinical and radiographic improvement. Although we observed low recurrence rates of calcified IAT, the retrospective nature of the study without a comparison group limits our ability to attribute this outcome directly to the addition of PMGR.
Gastrocnemius recession, defined as the release of the proximal, middle, or distal aspect of the muscle tendon unit has proven to be effective on patients presenting with IAT.7,18,22 The rationale behind PMGR was initially described by Barouk and Barouk,1,2 as this surgical approach proved to be less invasive and safer when comparing to traditional gastrocnemius recession procedures. Gurdezi et al 10 compared the clinical results of PMGR on patients presenting with IAT and noninsertional Achilles tendinosis, at an average 2.5-year follow-up. Despite reporting clinical improvement in both groups, the 4 patients included in the IAT group did not reach statistical significance and, quite notably, all patients went on to have revision surgery in order to perform ATDR or calcaneal exostectomy. There was also 1 case of deep vein thrombosis and 1 hypertrophied scar. Looking at our series, we listed 2 patients with superficial wound dehiscence (3.77%) involving PMGR, both healing with local wound care without need of antibiotic therapy. A relevant finding from our study is the absence of neurologic complications, a complication frequently reported on more distal gastrocnemius lengthening procedures.19,22
We registered 45 very satisfied patients (84.91%), 6 satisfied patients (11.32%), and 2 unsatisfied patients (3.77%), as well as statistically significant improvement on both clinical scores tested (P < .05) (Table 2). One patient (1.89%) reported dissatisfaction due to persistent scar pain over the ADTR incision, which only bothered him while working with safety footwear. The second unsatisfied patient (1.89%) required revision surgery, because of local irritation caused by suture threads originating from the suture anchor. After removal of the suture anchor, the symptoms resolved. This rare hardware-related complication has also been reported with knotless suture anchors in prior studies.5,8,21 Ettinger et al 5 reviewed 40 patients who were surgically treated with ATDR for symptomatic IAT and reported an overall statistically significant improvement on AOFAS and FAOS scores, at a mean follow-up of 15.6 ± 3.7 (range, 12-27) months. Tay et al 23 reported on 75 cases of ATDR for IAT, with continued improvement 2 years postoperatively, as the mean preoperative VAS-P score improved from 6.73 to 0.55 at final follow-up. A recent study by Stumpner et al 21 found excellent functional results and high patient satisfaction regarding postoperative sports ability on 25 patients presenting with IAT who underwent ATDR, with a minimum follow-up of 28.3 months, with only 1 patient (4%) reporting scar pain.
In terms of radiographic evaluation, there was nearly complete disappearance of calcified IAT, with mean postoperative calcification length of 0.36 mm and calcification width of 0.38 mm (Table 3). We found recurrence of minor Achilles IC on 10 patients (18.87%), but quite notably without any clinical influence, as all these patients were part of the very satisfied group (Figure 3). Greiner et al, 8 who performed ATDR on 42 patients presenting with symptomatic calcified IAT, found recurrence of Achilles calcifications (either intratendinous or insertional) on lateral radiograph on 30 patients (71.4%), at a mean follow-up of 32.8 (range 18-52) months. Perhaps more interestingly, they found recurrence of distal insertional Achilles calcifications on 13 patients (20.9%), a finding virtually absent from our series. Nunley et al 17 described a 50% recurrence rate (11 of 22 patients) of Achilles calcifications on the longest follow-up available (mean 7 years) on radiographic results of ATDR for calcified IAT. Our findings raise the obvious question if adding the PMGR to ATDR contributed to the lower recurrence rate of calcifications observed in our cohort. However, a comparative study is needed to determine this. There was also statistically significant improvement regarding the Fowler-Philip angle, reflecting additional radiographic improvement on Haglund deformity, which is quite often found on patients presenting with calcified IAT (Table 3). Güler et al 9 reported a similar statistically significant Fowler-Philip angle improvement from 55 ± 6 preoperatively to 32 ± 3 on 27 patients presenting with Haglund deformity, at a mean follow-up of 30 (range, 21-39) months. Ma et al 12 compared Haglund resection vs nonresection for patients presenting with calcified IAT and undergoing surgical treatment with ATDR and, at a minimum follow-up of 24 months, reported greater improvement on Fowler-Philip angle on the Haglund resection group, decreasing from 55.55 ± 12.34 (range, 43-84) preoperatively to 44.52 ± 10.24 at the latest follow-up.
Limitations to our study include the retrospective study design and a limited mean follow-up of 46 months. Additionally, the lack of a control group precludes direct attribution of clinical or radiographic outcomes specifically to the addition of PMGR. The strengths include using patient-reported outcomes, as well as clinical and radiographic evaluation completed by 2 of the coauthors and 2 independent research associates.
Conclusion
Combined PMGR and ATDR provides significant clinical and radiographic improvement for patients presenting with symptomatic calcified IAT and, although not preventing radiographic recurrence of minor Achilles IC, was associated with low recurrence of calcified IAT, in our cohort, although causality cannot be established in this retrospective case series.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251348194 – Supplemental material for Outcomes of Combined Proximal Medial Gastrocnemius Release and Achilles Tendon Debridement and Reinsertion for Calcified Insertional Achilles Tendinopathy
Supplemental material, sj-pdf-1-fao-10.1177_24730114251348194 for Outcomes of Combined Proximal Medial Gastrocnemius Release and Achilles Tendon Debridement and Reinsertion for Calcified Insertional Achilles Tendinopathy by Daniel Saraiva, Markus Knupp, Daniel Freitas, André Sá Rodrigues, Tiago Pato, José Tulha, Tiago Mota Gomes and Xavier Martín Oliva in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
This study methodology is in accordance with the ethical standards of the first author’s institutional Ethics Committee, as well as with the Declaration of Helsinki and the Guidelines for Good Clinical Practice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written informed consent was obtained from all patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.