
Abstract
Background:
Magnetic resonance imaging (MRI) has been used as a diagnostic and prognostic instrument to evaluate the results of conservative treatment for plantar fasciitis. However, there are scarce data available relative to changes in the plantar fascia after operative treatment. The primary objective of this study is to evaluate the imaging changes in patients with recalcitrant plantar fasciitis treated operatively by means of proximal medial gastrocnemius release.
Methods:
Thirteen patients with recalcitrant plantar fasciitis were studied with MRI preoperatively and 1 year after operative treatment. Quantitative (plantar fascia thickness) and qualitative variables (hyperintensity in the plantar fascia, insertional calcaneus bone edema, a plantar fascia tear, and the presence of perifascial collections) were assessed by 2 musculoskeletal radiologists. Clinical results were also measured with American Orthopaedic Ankle & Society (AOFAS), visual analog scale (VAS) pain, and 36-Item Short Form Health Survey (SF-36) scales.
Results:
The mean plantar fascia thickness was 6.59 mm preoperatively and 6.37 mm postoperatively (P = .972). No statistically significant differences were found in any of the qualitative variables on comparing the pre- and postoperative periods. Patients reported clinical improvements in pain VAS, AOFAS measurement, and the physical subdomains of the SF-36 scale.
Conclusion:
Quantitative and qualitative variables assessed for the plantar fascia on MRI did not show any significant change after medial gastrocnemius release despite clear clinical improvement.
Level of Evidence:
Level II, perspective cohort study.
Introduction
Plantar fasciitis represents the most frequent cause of talalgia in adults. It affects approximately 2 million people annually in the United States. 25 Furthermore, it is estimated that 10% of patients will present with it at some time in their life. It is a self-limiting condition that improves with conservative treatment in 90% of the cases. 5 The diagnosis is clinical but it can be associated with imaging studies such as magnetic resonance imaging (MRI) and ultrasonography to rule out other pathologies. 23 The thickness of the plantar fascia can be measured with those ancillary tests, with 4 mm being considered pathologic. 14
Some 10% of patients will not improve with conservative treatment and will enter the chronic stage of the disease, which is denominated recalcitrant plantar fasciitis (RPF). 6 It is only then, when nonoperative measures are exhausted, that operative treatment should be considered. 1
Currently, one of the most accepted operative treatments for RPF is the release of the proximal medial gastrocnemius owing to its low rate of complications and good functional results. 11,23
MRI findings like plantar fascia thickness or other qualitative variables (bone marrow edema, a high-signal intensity area in the fascia or tear of the fascia) have been used to assess the effectiveness of plantar fasciitis treatment. MRI findings have been assessed before and after conservative treatment and have been proposed as an indicator of a good response in terms of pain and function. 9,17,18,21
Little has been published on surgical treatment and MRI findings of RPF. 31,32 To our knowledge, there is no previous study that evaluates and compares pre- and postoperative MRI findings after proximal medial gastrocnemius release in patients with this condition.
The objective of this study is to evaluate, preoperatively and 1 year postoperatively, MRI quantitative and qualitative variables in patients operated on for RPF using proximal medial gastrocnemius release. Our initial hypothesis was that there would be a decrease in the thickness of the plantar fascia and modifications in the qualitative variables after surgical treatment, especially in the hyperintensity variable in plantar fascia.
As a secondary objective, an interobserver correlation study was carried out to assess the effectiveness of an MRI variable findings assessment.
Materials and Methods
Patients and Treatment
This study is a part of a randomized controlled trial of surgical treatment in RPF. 11 Fifteen patients were included in the proximal medial gastrocnemius release group. Two patients did not show up for the scheduled postoperative MRI, leaving 13 patients between 30 and 68 years old enrolled in the study. They underwent surgery for RPF by means of proximal medial gastrocnemius release in a single institution between 2012 and 2016.
The inclusion criteria were patients older than 18 years with a clinical diagnosis of RPF treated for at least 9 months with conservative treatment who had not responded. The diagnosis was clinical and consisted of mechanical heel pain, especially in the first steps of the day or after a prolonged period of rest and acute pain on palpation on the medial side of the proximal insertion of the plantar fascia. Conservative treatment included anti-inflammatory drugs, physical therapy consisting of calf muscle and fascia elongation exercises (checked for good compliance), the use of inserts (mainly padded inserts in the heel), and infiltrative therapy (1 mL of local anesthetic with triamcinolone). 7
After conservative treatment failed, patients were evaluated with preoperative MRI and ultrasonography to rule out other masked conditions and to describe pathologic changes within and around the fascia. Subsequently, they were programmed surgical treatment with proximal release of the medial gastrocnemius. The surgery was performed by a single orthopedic surgeon. Surgical technique and clinical outcomes have been thoroughly described in a previous published work. 11 The results in terms of pain, satisfaction, function, and self-reported health perception have been recorded using the visual analog scale for pain, Likert satisfaction, and American Orthopaedic Foot & Ankle Society hindfoot scales and the 36-Item Short Form Health Survey (SF-36) questionnaire, respectively. All patients were evaluated with a new MRI at 1 year postoperatively to compare the imaging changes to the preoperative MRI.
The exclusion criteria were any previous foot and ankle pathology (fracture, infections, deformity, and surgery), patients with rheumatoid arthritis, the presence of neuropathic heel pain, or the need for chronic analgesics due to another condition.
The research was approved by the local ethics committee. The nature of the study was explained to the patients and they gave their consent to participate in it.
Evaluation With MR Images
The MRI (both preoperative and postoperative) findings were evaluated by 2 musculoskeletal radiologists from the same institution preoperatively at 1 year after surgery. The quantitative variable considered was fascia thickness. Four qualitative variables were evaluated. They were a signal change in plantar fascia (hyperintensity), bone marrow edema, a plantar fascia tear, and perifascial soft tissues collections. The MRI examinations were performed on a 3-tesla (T) imaging system (Achieva; Philips Medical Systems, Oakwood, GA) using a phased-array knee coil. The ankle was examined in the supine position without support for the ankle. The 3-T MRI protocol comprised a sagittal T1 (response time [TR] / echo time [TE] = 500 ms / 20 ms) and short-TI inversion recovery (STIR; TR/TE = 3543 ms / 60 ms; inversion time [TI] 230 ms) or T2 with fat-suppression (FS) sequence (2578 ms / 80 ms) and a coronal T1 (TR/TE = 500 ms / 20 ms) or proton density (PD) fat-suppressed sequence (TR/TE = 5729 ms / 30 ms).
The thickness of the plantar fascia was assessed in sagittal T1-weighted images. The radiologists used a ruler within the software to measure the thickness of the fascia and measurements were performed 1 cm from the insertion site of the fascia into the calcaneus on an axis perpendicular to it. This is the area where the greatest thickness of the plantar fascia has been found. 10 An example is shown in Figure 1.

(A) Pre- and (B) postoperative sagittal T1-weighted MRI: no changes are observed in the thickness of the plantar fascia.
The qualitative variables were assessed in STIR sagittal and T2-weighted FS sagittal sequences as shown in Figure 2. The assessment criteria were (1) hyperintensity: increasing signal change within the plantar fascia (comparing it to the hypointensity of the normal plantar fascia); (2) bone edema: rising signal in calcaneus bone marrow in the area of plantar fascia attachment; (3) plantar fascia tear marked hyperintensity (fluid signal) with partial or complete disruption of the fascia; (4) presence of perifascial collections (fluid signal in soft tissues surrounding plantar fascia).

(A) Preoperative sagittal STIR MRI image shows hyperintensity in the plantar fascia (single arrow) as well as perifascial collections. (B) No changes (double arrow) are observed after surgery. MRI, magnetic resonance imaging; STIR, short-TI (inversion time) inversion recovery.
Both radiologists carried out a blinded reading of the MRI variables. They did not know whether the images were pre- or postoperative. Moreover, all the MRI images for each participant were scored randomly, mixing pre- and postoperative images.
For the interobserver correlation study, 2 different assessments were done. The first was done without a consensus for any specific image of the sequence seen. Each radiologist assessed all the images in the same sequence to score the variable.
In the second one, a consensus between both radiologists was reached to determine which image of the sequence was the most accurate and representative to evaluate each variable in each patient. This second measurement (consensus) was used to make the statistical pre- and postoperative comparison of all the variables studied.
Statistical Analysis
A descriptive statistical analysis of data was performed. The interobserver correlation study was done using a correlation coefficient index for quantitative variables, and a Kappa index was used to assess the qualitative variables.
A Wilcoxon signed-rank test was used to compare pre- and postoperative fascia thickness. The McNemar test was used for repeated comparisons of qualitative variables. Data were analyzed using IBM-SPSS 26.0 (IBM Corp, Armonk, NY). A P value <.05 was considered to indicate statistical significance.
Results
The interobserver correlation of the variables analyzed when there was no consensus on the specific image observed turned out to be nonsignificant, which are specified in Table 1. The interobserver correlation improved when there was a consensus, being higher and significant for the majority of the variables. They are summarized in Table 2. For the pre- to postoperative comparison analysis, the data obtained from the images evaluated in consensus by the 2 radiologists were used. The average thickness of the plantar fascia before surgery was 6.58 mm for observer 1 and 6.6 mm for observer 2. One year after surgery, the average was 6.41 mm for observer 1 and 6.34 mm for observer 2. No statistically significant differences were found in plantar fascia thickness (P = .97), as seen in Table 3. Regarding qualitative variables, no statistically significant differences for any of the variables were found after 1 year of the surgical treatment. Those data are summarized in Table 4.
Interobserver Correlation (No Consensus).

Abbreviations: CCI, correlation coefficient index; postop, postoperatively; preop, preoperatively.
a Qualitative findings are expressed in number of feet.
Interobserver Correlation (Consensus).
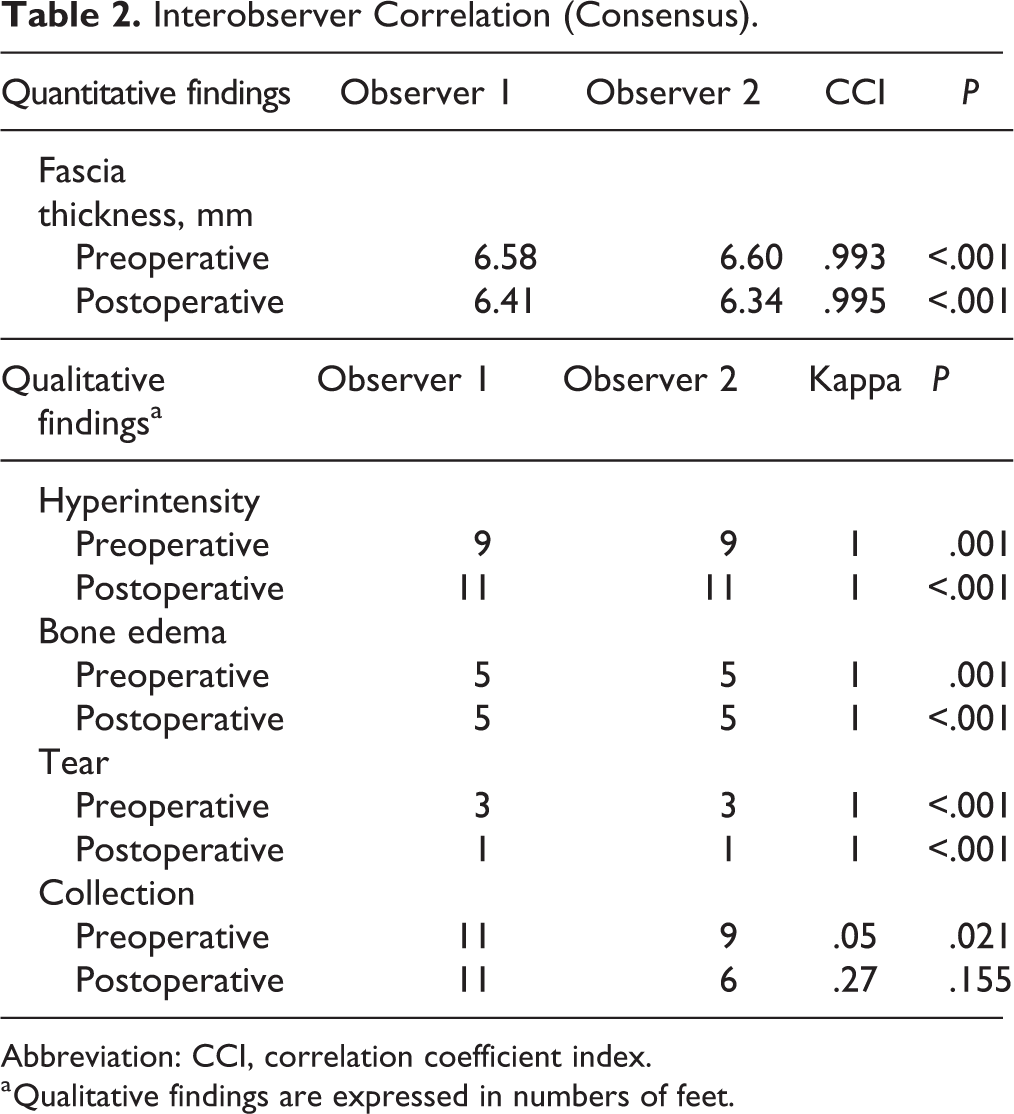
Abbreviation: CCI, correlation coefficient index.
a Qualitative findings are expressed in numbers of feet.
Preoperative vs Postoperative Comparison of Plantar Fascia Thicknessa

a Data were obtained from radiologic consensus.
Preoperative vs Postoperative Comparison of Qualitative Variables.a

a Data were obtained from the radiologic consensus. Values are expressed in numbers of feet.
Clinical Outcomes
Although it is not the aim of this study, it is important to highlight that the majority of the patients that took part in a previously published study 11 showed improved clinical results at 1 year of surgery in terms of pain, quality of life, and function with a satisfaction rate above 85%. The results are summarized in Tables 5 and 6.
Clinical Results at 1-Year Follow-up.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; VAS, visual analog scale.
SF-36 at 1-Year Follow-up.

Abbreviation: SF-36, 36-Item Short Form Health Survey.
Discussion
The main finding of the study was that there was no imaging variation in all variables studied between the preoperative and postoperative periods.
With regard to plantar fascia thickness, a minimum nonsignificant difference was found after the release of the proximal medial gastrocnemius (Figure 1). This is in contrast to what is described in numerous studies in the literature about the relationship between treatment response and plantar fascia thickness changes in plantar fasciitis. It is well known that patients who have plantar fasciitis suffer an increase in plantar fascia thickness. 2,4,10,20 A decrease in plantar fascia thickness measured by means of MRI after conservative treatment has been reported in acute cases 3 as well as in cases with a chronic symptoms onset. 12,30 This decrease has been correlated with a good treatment response in those cases. This is probably due to the fact that all of these studies enrolled patients who did not have a longstanding evolution time from the onset of the symptoms. It is thought that inflammatory changes are present in plantar fascia at the moment of treatment, early in the clinical course while still modifiable. Therefore, they can be resolved with the effect of the conservative treatment applied, and this fact is reflected in a reduction of plantar fascia thickness. On the other hand, patients who have chronic symptoms of plantar fasciitis and do not respond to conservative treatment finally develop RPF. Herein, the reparative process produces neovascularization and fibrosis that brings on degeneration of the fascia (fasciosis) rather than chronic inflammation. 10,16,22 These kinds of changes can be considered irreversible. In these cases, the plantar fascia thickness measured by MRI is not supposed to be modified by the treatment. 19 These chronic histological degenerative changes are thought to be the main explanation for the MRI findings in plantar fascia thickness reported in this article. The mean time from the onset of the symptoms to surgery was 29 months. During the symptomatic period, they received conservative treatment. Therefore, the minimum follow-up period was at least 9 months for all patients, during which there was comprehensive monitoring and checking for compliance prior to including them in the investigation. It means that all of them were diagnosed with RPF. Moreover, this finding is consistent with the results observed by Gamba et al 10 where no correlations were found between plantar fascia thickness and the clinical status of patients with RPF in terms of pain, function, and perceived quality of life.
Relative to the qualitative variables, no significant differences in these measurements (hyperintensity of the plantar fascia, insertional bone edema, fascia tear, and perifascial collections) were seen at 1 year of surgery (Figure 2). Once more, these findings are also contrary to what is reported in previous studies of conservative treatment in acute cases or even chronic evolution from the onset of plantar fasciitis symptoms. 3,19 Those authors reported changes in the qualitative variables after conservative treatment. The majority of them used shock wave therapy. It is especially the case for hyperintensity of the fascia and bone edema. These MRI findings have been associated with acute inflammation, and the hyperintensity and edema tend to be reduced or minimized. In contrast, Ulusoy et al 30 found no important differences in those 2 variables on comparing them before conservative treatment and 1 month after it. 30 The main reason those results are consistent with ours may lie in the fact that they included patients with more than 6 months of symptoms. Moreover, they were already unresponsive at 6 weeks of the first-step conservative treatment. It is not enough time to visualize changes in the MRI because of the short follow-up. The sample in our study includes patients who had symptoms for some years and were unresponsive after more than 9 months of distinct conservative treatments.
Therefore, it seems that RPF shows unmodifiable MRI qualitative findings after treatment. The greater the evolution from the onset of symptoms, the more unmodifiable the MRI qualitative variables.
The most widely accepted surgical treatment for PF has long been the partial plantar fasciotomy. 26,29 However, foot and ankle surgeons moved to “gastrocnemius recession” techniques because of some characteristic biomechanical complications, 12,13 the unsatisfactory results with some patient series 14 and their better understanding of biomechanics. 6,8,13,15,23,28 In particular, the proximal medial gastrocnemius release procedure has gained favor in recent years and come to be one of the most common surgical option for most surgeons. This technique manages to decrease the excess tensile stress on the Achilles-calcaneal-plantar complex enough to prevent the potential biomechanical complications of the partial fasciotomy. Moreover, good clinical and functional results have been supported by new findings. 11,23,24
Regarding surgical treatment and MRI findings, studies by Yu et al 31,32 have described the pre- vs post-MRI changes in partial plantar fasciotomy. Those authors studied asymptomatic individuals who had had a partial fasciotomy after 24 months (range 11-46). They found a minimum reduction of the fascia at the site of enthesis (only a 14% reduction), but the fascial thickness at the fasciotomy site nearly doubled. On the other hand, an absence of edema in the fascia and perifascial tissues as well as an absence of bone marrow edema were the main key postoperative observations. It contrasted with our observation after surgical treatment relative to the qualitative variables. Some drawbacks in the methodology of this article may explain these results. First, only 5 patients had preoperative MRI images to facilitate comparing the pre- and postoperative periods. Second, the postsurgical changes made by means of this local surgery of the plantar fascia may be an impediment to an accurate assessment of the subjective qualitative variables. Otherwise, medial gastrocnemius release produces a biomechanical effect at a distance. It makes it possible for the observers to do a better local MRI assessment. This at-a-distance biomechanical effect probably explains why these qualitative variables had not changed at 1 year of surgical treatment. As far as we know, the present study is the first to evaluate MRI changes after proximal medial gastrocnemius release in patients with RPF.
It is important to highlight that these results are based on measurements obtained after a rigorous process of coming to a consensus among radiologists. A strict protocol drastically changed the reproducibility of the variable assessments. This has been previously demonstrated to happen with ultrasonographic evaluations of the plantar fascia. When a strictly agreed protocol is introduced to obtain the measurement of variables, reproducibility improves. 4,27 The results from this study bring to light the subjectiveness around these variables and the great importance of reaching a consensus among observers.
This study had some limitations. First, it is a small sample. This corresponds to a sample of patients from a line of investigation used to research other aspects of the PF. Additionally, the few previous studies of this topic had a similar sample size. Second, these variables have a measurement error for which a correlation study between 2 musculoskeletal specialized observers tried to minimize. These observations improved their correlations when a consensus had been established (in terms of the specific image of the sequence that should be examined). However, it is our opinion that these items (especially the qualitative variables) are subjective variables. As a result, they are quite difficult to assess. Presumably, an intraobserver correlation may increase the accuracy of this measurement. Finally, no correlations with clinical and functional results are mentioned. It was not considered worthwhile as no pre-post changes were observed in the MRI findings. Additionally, the vast majority of patients had a significant improvement in terms of pain, function, and quality of life. Notably, some 86% were satisfied with the result of the surgery. 11
Conclusion
As best we can tell from this limited series using the methodologies we had to assess outcomes, plantar fascia morphology did not significantly change after medial gastrocnemius release in patients with RPF, despite the clear symptomatic improvement. Further study is clearly warranted to better elucidate the cause of clinical improvement after surgical release of the medial head of the gastrocnemius to treat RPF.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211027323 - Clinical And Plantar Fascial Morphologic Changes After Proximal Medial Gastrocnemius Release Treatment of Recalcitrant Plantar Fasciitis
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211027323 for Clinical And Plantar Fascial Morphologic Changes After Proximal Medial Gastrocnemius Release Treatment of Recalcitrant Plantar Fasciitis by Alberto Ginés-Cespedosa, Ignacio Wormull Ugarte, Jesus Ares-Vidal, Alberto Solano-Lopez, Daniel Bianco Adames and Carlo Gamba in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
The research was approved by the local ethics committee. The nature of the study was explained to the patients and they gave their consent to participate in it.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.