
Abstract
Background:
Although metatarsophalangeal joint (MTPJ) arthrodesis is considered the “gold standard” for treatment of advanced MTPJ arthritis, a modified oblique Keller capsular interposition arthroplasty (MOKCIA) is an alternative treatment for hallux rigidus that retains MTPJ motion. We aim to retrospectively compare long-term patient-reported outcomes, radiographic alignment, MTPJ walking kinematics, and plantar pressure between the MOKCIA and MTPJ arthrodesis for advanced hallux rigidus.
Methods:
Thirty-five patients were recruited from a retrospective chart review (MOKCIA [n = 15, average 15 years from surgery] or an arthrodesis [n = 20, average 13 years from surgery]). We measured visual analog scale (VAS) pain and satisfaction, Foot and Ankle Ability Measure (FAAM), Patient-Reported Outcomes Measurement Information System (PROMIS) physical function scores, radiographs, walking MTPJ sagittal plane kinematics, forefoot, and first toe peak plantar pressure during walking, MTPJ goniometer range of motion, and need for additional surgery. Two-sample t tests or χ2 were used to compare groups. A Spearman correlation was used to examine the relationships between measured variables.
Results:
Groups did not differ on demographic characteristics, FAAM activities of daily living scale (MOKCIA = 94 ± 8, arthrodesis = 94 ± 7, P = .93), PROMIS physical function T-score (MOKCIA = 50 ± 6, arthrodesis = 48 ± 6, P = .41), forefoot, and first-toe walking peak plantar pressure. The MOKCIA had small but significantly lower VAS pain (MOKCIA = 0.1 ± 0.3, arthrodesis = 1.0 ± 1.6, P = .02) and higher satisfaction scores (MOKCIA = 9.5 ± 0.9, arthrodesis = 8.4 ± 1.8, P = .03). MTPJ passive arc of excursion in the MOKCIA group was 44 ± 15 degrees, and greater goniometric measured flexion of the first MTPJ correlated with greater patient satisfaction in the MOKCIA group (ρ = 0.70, P < .01). No MOKCIA patient in our study group required additional surgery.
Conclusion:
Patients in both the MOKCIA and arthrodesis groups reported high function with little limitation due to their toe surgery. Patients in the MOKCIA group had similar pain and satisfaction compared with the arthrodesis group. These results suggest MOKCIA is a joint range of motion–preserving alternative to MTPJ arthrodesis for long-term treatment of hallux rigidus.
Level of Evidence:
Level III, retrospective, cohort study.
This is a visual representation of the abstract.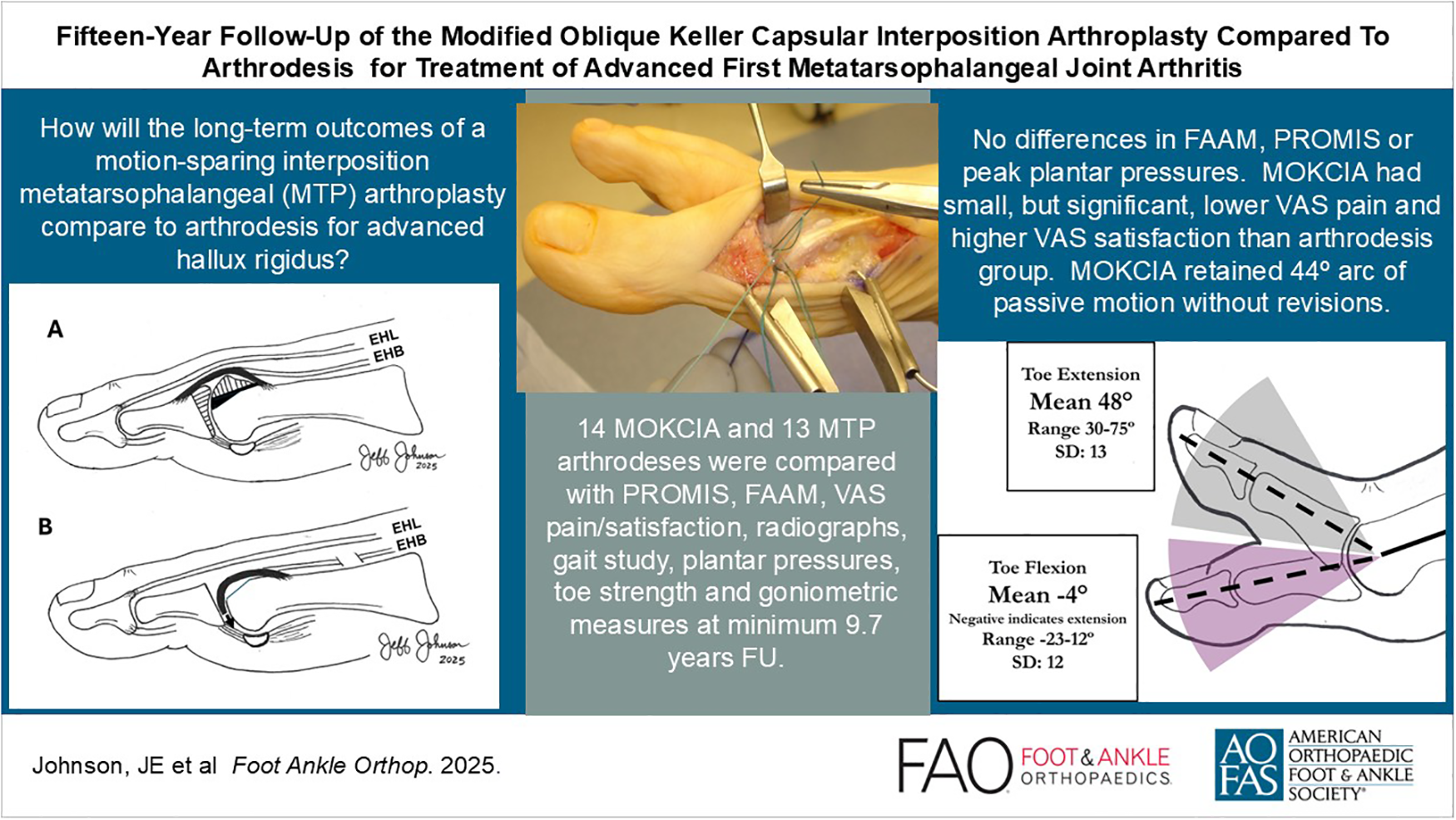
Keywords
Introduction
Hallux rigidus is a common musculoskeletal condition characterized by osteoarthritic changes of the first metatarsophalangeal joint (MTPJ) with dorsal osteophyte formation, joint space narrowing, and painful MTPJ motion that can limit weightbearing activities. 7 Although arthrodesis of the first MTPJ for late-stage disease (Coughlin-Shurnas grade 3 and 4) provides satisfactory pain relief and typically restores satisfactory levels of function, 6 patients and surgeons continue to show interest in procedures for advanced hallux rigidus that allow for pain control as well as maintenance of first MTPJ range of motion. Joint range of motion–preserving procedures using numerous different materials including metal, polyvinyl alcohol hydrogel, silicone polymers, and autogenous and allograft biologic materials have been advocated by numerous authors.3,4,10,11,13,15,19 -21,22,24 -26,29,30,32 However, most of these arthroplasty procedures have not replaced arthrodesis as the standard treatment for hallux rigidus because of implant material failures, lack of reproducible results by surgeons other than the surgeon developer, local tissue complications, poor clinical outcomes, or the lack of long-term data.1,2,5
The modified oblique Keller capsular interposition arthroplasty (MOKCIA) is a motion-preserving procedure that uses autogenous MTPJ capsule or allograft soft tissue as an interposition resurfacing arthroplasty for treatment of late-stage hallux rigidus.3,15,19,25,26,29 The MOKCIA procedure has provided favorable midterm results for late-stage hallux rigidus, as reported by some authors, and has not been plagued with some of the failures caused by shortening or toe deformity associated with procedures that use synthetic implant materials.1,3,5,11,29 Nevertheless, the procedure has not attained widespread use, in part, because long-term outcomes from a controlled study are lacking. The purpose of this study is to retrospectively compare the long-term outcomes of the MOKCIA procedure and MTPJ arthrodesis for late-stage hallux rigidus to provide foundational evidence that will inform treatment decisions for patients and surgeons. We hypothesized that patients undergoing the MOKCIA procedure would have similar patient-reported outcomes and functional testing when compared to patients who underwent arthrodesis at long-term follow-up.
Methods
Following institutional review board authorization, the Department of Orthopaedic Surgery database at our institution was retrospectively queried for all patients aged 18-75 years who received either a first MTPJ arthrodesis or a MOKCIA procedure for the diagnosis of advanced hallux rigidus between January 1, 2005, and December 31, 2020. Hallux procedures for all other diagnoses were excluded. This yielded 58 MOKCIA patients (62 feet) and 112 metatarsophalangeal arthrodesis patients (112 feet). From this group, a long-term outcome cohort was defined with a minimum of 9.7 years of follow-up consisting of 29 MOKCIA subjects (34 feet) and 55 arthrodesis subjects (55 feet). The first foot operated on of bilateral feet was eligible for inclusion.
Study participants were recruited according to the flow diagram with up to 3 attempts to contact by phone, followed by 1 mailing for all subjects who had accurate contact information, which yielded 14 MOKCIA and 13 arthrodesis subjects for the full study (Figure 1). All data collection and subject testing occurred between September 2023 and March 2024. Participant demographics, body mass index (BMI), presence of diabetes and other medical comorbidities, history of prior procedures, and smoking status were recorded. The index operative report was retrospectively evaluated to ensure the procedures were performed for isolated hallux rigidus. Exclusion criteria included neuropathy at the time of surgery, neurologic disorders affecting gait at the time of surgery or currently (eg, Parkinson, stroke with motor deficits, cerebral palsy, myelopathy), patients with current dementia that would affect patient-reported outcome measures, and patients who underwent a MOKCIA or arthrodesis for any diagnosis other than hallux rigidus.

Study recruitment flow diagram showing the results of exclusion criteria on the final study groups.
The decision for which procedure was performed was made preoperatively based on a diagnosis of hallux rigidus rated as grade 3 or 4 7 and surgeon-patient preference based on a preoperative discussion of the risks, goals, and expectations for each procedure. The MOKCIA procedure was offered for patients with at least a 30-degree arc of metatarsophalangeal motion and no significant angular deformity or prior surgery. The MOKCIA procedures were performed by 2 fellowship-trained surgeons, and the arthrodeses were performed by those surgeons and 1 additional fellowship-trained surgeon.
MOKCIA Surgical Technique
The MOKCIA procedure was performed as initially described by Mroczek and Miller, modified from Hamilton’s technique, consisting of a dorsal cheilectomy, oblique resection of the phalanx base, and interposition of the dorsal capsule15,29 (Figure 2). Slight modifications were made using a dorsomedial incision just above the mid-axis of the first metatarsal head rather than a dorsal incision medial to the extensor hallucis longus (EHL) tendon.19,25 It is not to be confused with the original Keller resection arthroplasty described in 1904, primarily for treatment of hallux valgus deformity.20,21,24 A dorsomedial incision was made in the extensor retinaculum 1 cm medial to the EHL. The dorsal subcutaneous tissues and EHL tendon were retracted laterally. A medial capsular incision was used to expose the entire dorsal half of the MT head, leaving the inferior portions of the medial and lateral collateral ligaments of the MTPJ intact. The dorsal joint capsule, along with the dorsal periosteum of the proximal phalanx and the attachment of the extensor hallucis brevis (EHB), were elevated together with the dorsal capsule to create a proximally based flap of soft tissue of sufficient length to cover the metatarsal head and reach to the plantar capsule. A dorsal cheilectomy was performed to remove osteophytes and decompress the joint. Then a micro-sagittal saw was used to remove a wedge-shaped sliver of bone and cartilage from the base of the proximal phalanx to create an oblique surface to the phalanx to further decompress the joint, allow a gap for the interposition of the capsular tissue, and preserve the proximal phalanx plantar plate attachment. Small amounts of additional bone were removed from the cheilectomy and proximal phalanx osteotomies until the great toe achieved 70 degrees of dorsiflexion relative to the metatarsal head while the graft is temporarily held interposed in the joint. In general, the dorsal cheilectomy removed slightly less bone than for a standard cheilectomy, and the acute angle created at the distal edge and sides of the cheilectomy was beveled to a more rounded shape to reduce the edge loading on the interposition tissue.

The MOKCIA procedure is based on the technique described by Mroczek and Miller and consists of (A) a dorsal cheilectomy and an oblique resection of the articular surface of the base of the proximal phalanx with interposition of the dorsal capsule .19,25,26,29 Note the area shaded in black in panel A that represents additional metatarsal head bone that may need to be removed to allow adequate space for insertion of (B) the capsular interposition graft and to allow for optimal toe dorsiflexion range of motion.
Using a small, stout, half-circle tapered point needle and 2-0 nonabsorbable braided suture, 4 sutures were placed in a row, but not tied, between the distal edge of the capsular tissue and the plantar plate. A pin distractor was used to aid exposure to the plantar plate as needed (Figure 3). A fifth suture was placed to act as a pull suture and threaded onto a Keith needle, which was then placed from dorsal to plantar through the plantar plate and out the skin under the first MTPJ. The EHB tendon was tenotomized in the proximal aspect of the incision to allow more capsular excursion, and the pull suture was used to advance the capsular interposition material over the metatarsal head to the plantar plate. While holding tension on the capsule, the 4 sutures were tied to secure the capsule to the plantar plate. The medial portion of the capsule was closed over the metatarsal head (Figure 4). If there was any slack in the medial capsule or valgus deviation of the great toe, the medial capsule is plicated to correct alignment. The extensor retinaculum was repaired to the dorsomedial capsule to centralize the extensor hallucis longus tendon and the subcutaneous tissues, and the skin was closed (Figure 5). In this study, no dermal allograft interposition arthroplasty patients were included.
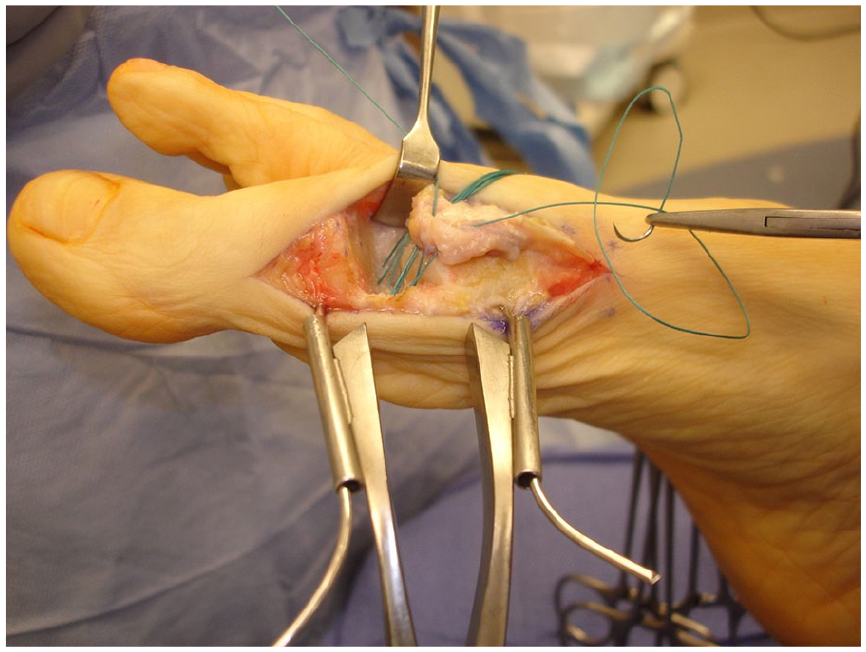

Using a pull stitch passed out the bottom of the joint, the capsular flap is pulled into the joint and the 4 sutures are tied. A tenotomy of the extensor digitorum brevis, made at the proximal end of the incision, aids in the delivery of the capsule to the plantar plate. (Source: From Figure 9 in Johnson and McCormick 19 )

The medial capsule is closed, and reefed as needed, to stabilize the great toe in neutral. (Source: From Figure 11 in Johnson and McCormick 19 )
A soft forefoot dressing was used to provide mild compression. At 2 weeks, sutures were removed, and an elastic toe wrap was applied. Weightbearing as tolerated was begun in a postoperative sandal and instructions given on passive and active toe flexion and extension range of motion exercises to be done at least 3 times per day for 10 minutes each session. The wrap was continued until the patient was able to transition to an athletic shoe at week 4, or when swelling and pain allowed.
First Metatarsophalangeal Joint Arthrodesis Surgical Technique
A standard dorsal, or dorsal-medial, approach was made over the MTPJ. The joint was prepped in a standard fashion with cannulated hemispherical reamers and drill perforations to expose cancellous bone and increase fusion surface area. The toe was aligned in a position of neutral rotation, slight dorsiflexion, and slight valgus with the aid of a flat metal plate to simulate the weightbearing surface and intraoperative radiographs. The toe position was held with a smooth wire. Rigid internal fixation was achieved with two 3.5-4.0-mm cancellous lag screws or 1 lag screw and a dorsal plate. A nonweightbearing cast was used for 6 weeks, followed by a weightbearing walker boot.
Study Protocol
Weightbearing radiographs
Standard (3-view) weightbearing anterior-posterior (AP), lateral, and oblique foot radiographs were completed. AP radiographic measurements included metatarsophalangeal-1 angle (MTP-1 angle) defined as the angle between the axis of the first metatarsal and the proximal phalanx; intermetatarsal 1-2 angle (IM1-2) defined as the angle between the shafts of the first and second metatarsal; hallux axis angle (Figure 6) defined as the angle between a line drawn from the middle of the proximal phalanx base to the tuft of great toe distal phalanx and first metatarsal shaft; and the second toe deviation angle defined as the angle between the axis of the second metatarsal and the second toe proximal phalanx. Lateral radiographic measurements including great toe proximal phalanx extension angle (PP extension) was defined by the angle between the mid-axis of the great toe proximal phalanx and the radiographic foot plate (Figure 7). All measurements were made with a digital radiographic measurement tool (IBM iConnect Access 8.2, https://mergecustomer.force.com/mergeusercommunity; Merge Healthcare Incorporated, Hartland, WI, USA) by a senior fellowship-trained orthopaedic surgeon. One surgeon measured twice, on separate occasions, and then measures were averaged.

Postoperative lateral radiograph of the MOKCIA procedure demonstrating the proximal phalanx extension angle measured between a line along the lateral axis of the proximal phalanx and the floor. Note the maintenance of joint space of this MOKCIA procedure subject at 20.6 years of follow-up who had her index surgery at 53 years of age.

Postoperative AP radiograph of the same MOKCIA procedure subject as shown in Figure 6. The hallux axis angle is measured between a line drawn from the middle of the proximal phalanx base to the tuft of the great toe distal phalanx and the first metatarsal axis.
Gait kinematics
Bilateral 3-dimensional (3D) gait kinematics during self-selected and fast gait speeds were collected using a 10-camera 3D motion capture system (Vicon, Los Angeles, CA, USA) and Bertec force plate (FP4060-10 model; Bertec Corporation, Columbus, OH, USA). Methods from recent publications were followed. Thirty 10-mm reflective markers were used to define the shank, foot, forefoot, and first toe proximal phalanx segments on each leg.16-18 All data were processed and analyzed using Vicon Nexus (Vicon), Visual3D (HAS-motion, Kingston, Ontario, Canada), and statistical package R. Six trials of gait speed, first MTPJ excursion, and ankle plantarflexion during gait were recorded and averaged.
Ten-meter walk time was used to assess gait speed. A 10-m walkway was measured and the time it takes to walk the central 6 m were recorded and used to calculate gait speed (m/s). The first and last 2 m allow time for acceleration and deceleration so that peak walking velocity is captured. 34
Plantar pressure and great toe flexion strength
Plantar pressure was assessed bilaterally using the 3-step method while walking barefoot at their self-selected walking speed. The plantar pressure distribution was divided into toe, forefoot, and hindfoot masks, and the peak plantar pressure in each mask was calculated by averaging 5 steps for each foot, a method found reliable in previous studies.16,17
First MTPJ toe flexion strength was measured with the participant seated in a chair, feet on the pressure mat, knees over toes, and arms crossed at chest height. The participant flexed their toes maximally for 5 seconds, rested for 3 seconds, and repeated this 5 times. The peak force produced during the entire trial was used in the analysis. 27
Goniometric joint range of motion
Standardized goniometry methods were used to assess active ankle dorsiflexion/plantarflexion, passive calcaneal eversion/inversion, and passive MTPJ flexion and extension. 8 All measures were repeated twice and averaged for analysis.
Patient-reported outcomes
Participants completed Patient-Reported Outcomes Measurement Information System (PROMIS) anxiety, pain interference, depression, and physical function questionnaires, Foot and Ankle Ability Measure sports and activities of daily living questionnaires, and the visual analog scale (VAS) for pain (0 = no pain, 10 = worst possible pain) and satisfaction (0 = extremely unsatisfied, 10 = extremely satisfied).
Statistical Analysis
Intraclass correlation coefficients (ICCs) were calculated from a linear mixed effects model to assess radiographic measurement interrater reliability. Histograms and Shapiro-Wilk tests were examined for the variables involved with tests that assumed normality. No substantial violation was detected. Thus, 2-sample t tests, χ2 tests, or Fisher exact tests were used to compare the long-term outcomes of the MOKCIA and Arthrodesis groups. For variables with significant group differences, Spearman correlation (rho) was used to examine the interrelationships. Statistical significance level was set at P <.05. All the statistical tests are 2-sided, and analysis was performed with SAS 9.4 (SAS Institute Inc, Cary, NC). Power analyses were completed for the variables that were close to being significant (P <.10) to inform future sample sizes.
Results
The demographics for both groups were not significantly different (Table 1). The following results, including weightbearing radiographs, gait kinematics, plantar pressure, great toe flexion strength, and goniometric joint range of motion, compare 14 participants in the MOKCIA group and 13 participants in the Arthrodesis group. The patient-reported outcomes compare 15 participants in the MOKCIA group and 20 participants in the Arthrodesis group.
Demographics (N = 35).

Weightbearing Radiographs
There were no nonunions in the arthrodesis group. The first MTP-1 angle on the AP radiograph and the great toe proximal phalanx extension (PP extension) angle on the lateral radiograph were significantly different between the MOKCIA and arthrodesis groups. There was no difference between groups in the angular measurements on the AP and lateral radiographs for intermetatarsal 1-2 angle, second toe deviation angle, or great toe axis angle. Intrarater correlation coefficient (ICC) for all radiographic measures indicated good to excellent intrarater reliability (range: 0.78-0.95) (Table 2). 23
Radiographic Measurements (N = 27).

Abbreviations: IM1-2, intermetatarsal 1-2 angle; MOKCIA, modified oblique Keller capsular interposition arthroplasty; MTP-1, metatarsophalangeal-1 angle; PP, proximal phalanx.
Gait Kinematics
There were no significant group differences in self-selected, fast-walking speed, ankle plantarflexor power, or 10-m walk time during gait kinematic testing. First MTPJ extension was greater in the MOKCIA group during self-selected gait and fast gait (P < .001; Table 3).
Gait Kinematics, Plantar Pressure, Great Toe Flexion Strength, Goniometric Joint Range of Motion (N = 27).

Abbreviations: MOKCIA, modified oblique Keller capsular interposition arthroplasty; MTPJ, metatarsophalangeal joint.
Plantar Pressure and Great Toe Flexion Strength
There was no significant group difference in walking speed during plantar pressure assessment, peak forefoot pressure, peak great toe plantar pressure, pressure time integral, or great toe flexion force (Table 3).
Goniometric Joint Range of Motion
There was no significant difference between groups for active ankle dorsiflexion or plantarflexion, or passive calcaneal inversion or eversion. The MOKCIA group had significantly greater first MTPJ passive extension and flexion (P < .001) (Table 3). The MOKCIA group had first MTPJ passive extension and flexion arc of motion of 44 degrees (Figure 8). The arthrodesis did not have an arc of range of motion (0 degrees).
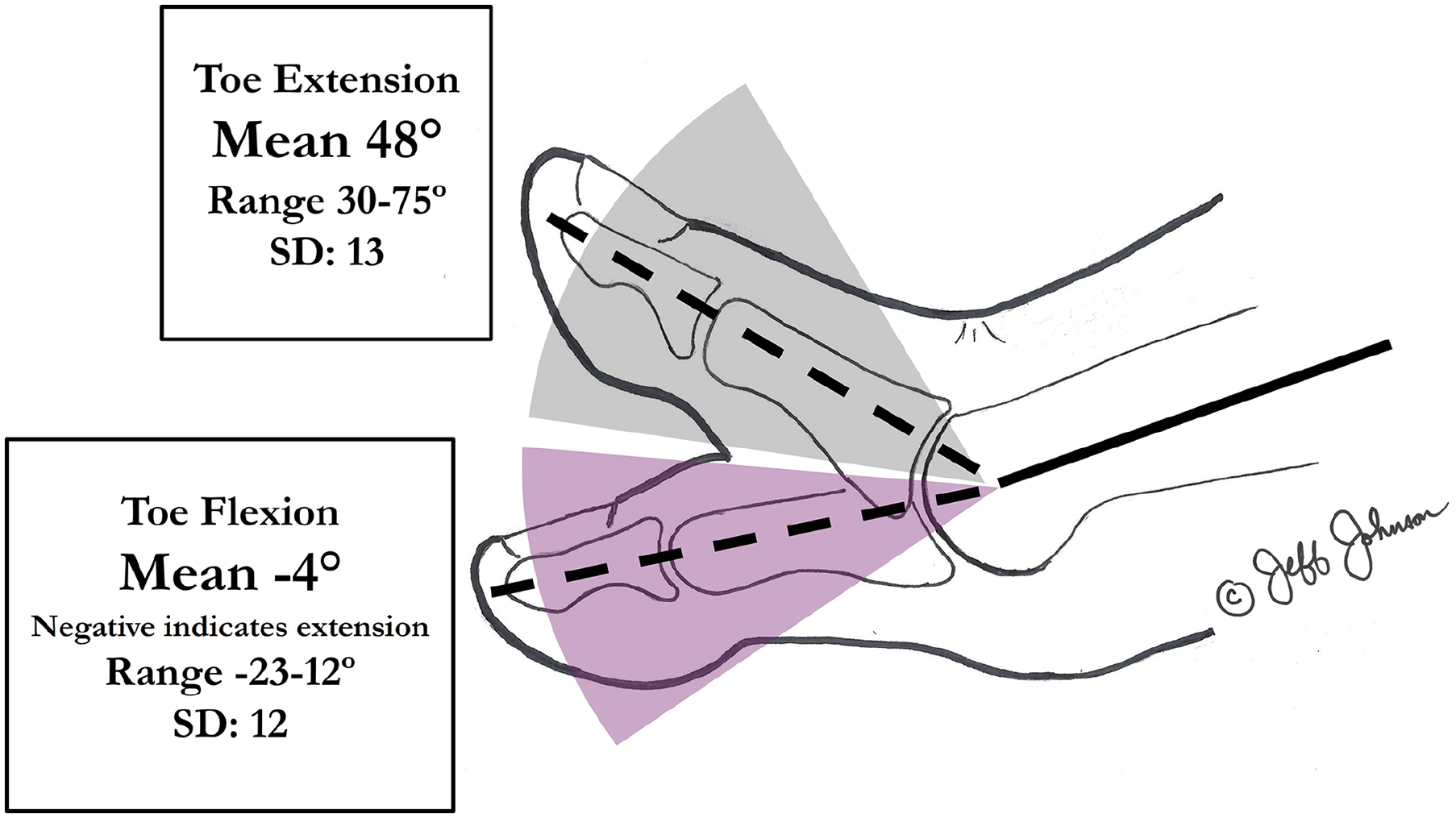
Goniometric measurement of passive toe extension and passive toe flexion were recorded as independent variables. The shaded area indicates the range of toe extension and flexion.
Patient-Reported Outcomes
The MOKCIA group had a small but significantly lower VAS pain scale and higher satisfaction VAS scores (Table 4). This did not meet the minimal clinically important difference (MCID) for hallux rigidus. 31 There were no differences between groups on Foot and Ankle Ability Measure sports and activities of daily living and PROMIS survey results. No patients in the MOKCIA study group (0 of 15) had a revision surgery, and 2 patients in the arthrodesis group (2 of 20) underwent hardware removal for a painful dorsal plate. There were no other complaints such as hypertrophic or sensitive scars or toe malposition.
Combined Questionnaire Results (n = 35).

Abbreviations: FAAM, Foot and Ankle Ability Measure; PROMIS, Patient-Reported Outcomes Measurement Information System.
Boldface indicates significance (P < .05).
Correlations
For the MOKCIA group, the proximal phalanx extension angle on the lateral radiograph was associated with less MTPJ flexion goniometric range of motion (rho = −.59, P = .03). Greater MTPJ flexion goniometric range of motion in the MOKCIA group is associated with greater VAS satisfaction scores (rho = .70, P = .01).
Power Analyses
The second-toe deviation radiographic measures (P = .06) and first-toe peak pressure during walking (p = 0.09) were close to being significant. A total sample size of 58 and 72, respectively, would be required to detect the significant difference between the MOKCIA and Arthrodesis group (power = 0.8, significance = 0.05).
Discussion
Our study reports the longest follow-up of patients with hallux rigidus who were treated with a MOKCIA (average follow-up 15 years) and compared outcomes to a cohort of similar patients who underwent arthrodesis (average follow-up 13 years). 11 There was high VAS satisfaction and low pain in both groups but the MOKCIA group was slightly, but significantly, better in both domains, had a passive arc of flexion and extension range of motion of 44 degrees, and did not require revisions. These data suggest that a joint-preserving MOKCIA procedure may be capable of providing slightly greater pain relief and satisfaction and no progression of toe deformity for late-stage hallux rigidus as compared to arthrodesis.
The static extension angle of the proximal phalanx to the floor on the weightbearing lateral radiographic view indicated the MOKCIA had a more plantarflexed position of the hallux than the arthrodesis group (7.9 degrees plantarflexion vs 2.8 degrees plantarflexion, P = .02). This indicates the MOKCIA group did not have an intrinsic minus toe deformity with cock-up or clawing, but had more flexion at the MTPJ than the arthrodesis group, on average. The MOKCIA group benefited when the static great toe extension was lower (ie, less dorsiflexed) because a lower static extension angle was correlated with greater flexion range of motion and greater flexion range of motion was correlated with greater VAS satisfaction.
Our study indicates a small but consistent and significantly lower VAS pain and greater satisfaction in MOKCIA group compared with the arthrodesis group. However, the difference we measured in VAS pain (0.9) between the groups does not exceed the MCID reported by Sutton et al, for pre- and post-hallux valgus surgery (1.8 and 5.2) and thus the surgical outcomes could be considered to be similar. 31 Coughlin and Shurnas 7 used VAS and AOFAS Hallux scores to report 77% excellent and 23% good results at an average of 6.7 years in 34 patients with isolated hallux rigidus. Studies on arthrodesis for other etiologies, including hallux rigidus, have shown high rates of satisfaction, low rates of nonunion, and advantages to a plate-and-screw construct in short-term follow-up.6,9,12,14,28,33
Because of a desire to retain joint motion in hallux rigidus patients, many different types of arthroplasty procedures have been reported previously. The results of many of the metal, ceramic, and silicone and other synthetic implants have been mixed, with generally short-term follow-up, high rates of revision, and inferior results when compared to fusion.2,5,22 Although initial Level I studies on a polyvinyl alcohol (PVA) hydrogel implant were promising and shown to be noninferior to arthrodesis at 1 and 2 years, reports by other surgeons were not able to reproduce the same results, and the use of this implant has decreased.1,4,5,10,30 Although there are numerous reports on hallux interposition arthroplasty, all but a few are Level IV case series using multiple different surgical techniques and interposition materials, without comparison to arthrodesis. 11 In a systematic review, Emmons and Carreira 11 noted there was “significant interest” in defining the efficacy of arthrodesis vs a motion-preserving interposition arthroplasty technique and based on the available data, “interposition arthroplasty appears to be a viable option” as a motion-sparing treatment for late-stage hallux rigidius. There are relatively few reports of results of the MOKCIA procedure technique as described in this study. Ayanardi et al, 3 reported on 133 patients using the MOKCIA technique in 77 patients and acellular dermal allograft in 56 patients with a 65% excellent and 24% good results with a 3.8% revision rate and 31 complications at 5.2 years, but without comparison to arthrodesis. Mackey et al 26 reported clinical and biomechanical outcomes on 10 MOKCIA patients compared with 12 hallux arthrodeses at 4.5 years and demonstrated equivalent clinical outcomes but with a 54-degree arc of MTP joint motion and a more normal plantar pressure pattern with ambulation in the MOKCIA group.
Our current study results were remarkably similar to those of Mackey et al 26 and 93% of our patients reported no pain 15 years after surgery. Our data add to the evidence that the MOKCIA procedure can preserve motion without compromising important outcomes like pain and toe alignment. The fact that the MOKCIA group subjects did not need to sacrifice their range of motion to achieve superior pain relief may offer a reason for their greater satisfaction in comparison to the arthrodesis group.
Limitations
Limitations to this current study include the small sample size with a recruitment rate of 15 of 29 MOKCIA subjects and 20 of 55 arthrodesis subjects who had isolated hallux rigidus and met the minimum 9.7-year follow-up criteria. Given the small sample, the addition of even a small number of less satisfied patients in either group could significantly affect the results. Because the study did not randomize individuals to their intervention, there could also be selection bias. Given the retrospective design of the study, the criteria that the 2 MOKCIA surgeons and the 3 arthrodesis surgeons used to determine what procedure to offer these patients is unknown. Although the arthrodesis surgical approach and joint preparation with hemispherical reamers was standardized, there was a slight variation in the type of fixation with either crossed screws or a single screw and dorsal plate. This could potentially introduce differences in the arthrodesis outcomes; however, both fixation constructs have shown similar results in the literature with high union rates for both screws and screw/plate configuration and there were no nonunions noted in the arthrodesis group regardless of fixation technique in our study.9, 14 ,28,33 All radiographs were taken using our standardized weightbearing protocol; however, errors in positioning could alter the radiographic measures. Sampling and courtesy bias could be present as more satisfied MOKCIA patients could have been more likely to participate in this study. It should be noted that all patients in this study underwent autologous dorsal capsular interposition arthroplasty. No dermal allografts were used and therefore generalization of the results to other interposition materials should not be made. A prospective study is needed to better understand the differences between MOKCIA and arthrodesis procedures.
Conclusion
Patients in the MOKCIA group had a significant decrease in pain and increase in satisfaction while preserving joint motion without deformity progression or the need for surgical revisions at an average 15 years of follow-up. The arthrodesis group had clinically equivalent pain and satisfaction with similar functional outcomes. Plantar pressures were not impacted by the surgical intervention performed. Given the limitations of this study, these results suggest the MOKCIA procedure may be a reasonable alternative option compared with first MTPJ arthrodesis for long-term treatment of late-stage hallux rigidus in patients who desire to preserve great toe range of motion and serve as a foundational study for future prospective research.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251322766 – Supplemental material for Fifteen-Year Follow-up of the Modified Oblique Keller Capsular Interposition Arthroplasty Compared to Arthrodesis for Treatment of Advanced First Metatarsophalangeal Joint Arthritis
Supplemental material, sj-pdf-1-fao-10.1177_24730114251322766 for Fifteen-Year Follow-up of the Modified Oblique Keller Capsular Interposition Arthroplasty Compared to Arthrodesis for Treatment of Advanced First Metatarsophalangeal Joint Arthritis by Jeffrey E. Johnson, Andrea R. Phinney, Mary K. Hastings, Hyo-Jung Jeong, Ling Chen, Andrew P. Thome, Jeremy J. McCormick and Jonathon D. Backus in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
The authors acknowledge the significant contribution of Carrie Burk, MHS, a senior clinical research coordinator in the Washington University Department of Orthopedic Surgery, for subject recruitment, testing, and data collection and Victoria Goldman for assistance with original artwork.
Author Note
This article was a finalist for the Roger Mann Award, for best clinical paper at the 2024 AOFAS Annual Meeting, Vancouver, BC.
Ethical Approval
This study was approved by the Washington University Institutional Review Board (IRB) and complied with all university guidelines in obtaining consents and conducting this research.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jeffrey E. Johnson, MD, reports general disclosures of equity in Rubber City Bracing (veroankle.com); and equity in Extremity Design Company (none relevant to this manuscript) and disclosures relevant to manuscript from AOFAS Grant (No. 2023-8S). Mary K. Hastings, PT, DPT, MSCI, ATC, and Hyo-Jung Jeong, PT, PhD, MS, report disclosures relevant to manuscript from AOFAS Grant (No. 2023-8S), which includes partial salary support. Jeremy J. McCormick, MD, reports consulting fees and royalties from Stryker, Inc. (none relevant to this manuscript). Jonathon D. Backus, MD, reports general disclosures from consulting fees, royalties, and research support from Medline Unite. Disclosure forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by a grant from the American Orthopaedic Foot & Ankle Society with funding from the Orthopaedic Foot & Ankle Foundation (grant 2023-8S).
Data Availability
The data for this study reside in a password-secure REDCap database and will be retained according to Washington University IRB protocol.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.