
Abstract
Joint arthroplasty of the first metatarsophalangeal (MTP) joint is an accepted surgical option for patients with hallux rigidus. However, this procedure has been reported to have a high complication rate and unpredictable survivorship. Implant arthroplasty failure is a devastating complication that results in significant osseous defect with altered biomechanics of the foot. Commonly, salvage options are limited to arthrodesis with bone grafting. However, outcomes are rarely reported. The purpose of this study is to investigate the fusion rates of first metatarsophalangeal joint arthrodesis after conversion from failed implant arthroplasty. A systematic review of electronic databases to find reports of conversion arthrodesis after failed implant arthroplasty was performed. Six studies involving a total of 76 patients with a weighted mean age of 54.9 met the inclusion criteria. Out of the 6 included articles, the nonunion rate was 16.5% at a weighted mean follow-up of 48.1 months. The nonunion rate in the current report is higher than reported nonunion rates of primary arthrodesis. More prospective studies with consistent and standard outcome measures are needed to further determine the success rate of this salvage procedure.
Introduction
First metatarsophalangeal (MTP) joint implant arthroplasty, developed initially in the 1950s, is a viable treatment option for patients wishing to achieve pain relief and deformity correction while also retaining joint motion.
1
Indications for the procedure include hallux rigidus, hallux valgus with arthritis, geriatric bunion deformity, iatrogenic and trauma-induced hallux metatarsophalangeal joint arthritis.
2
The procedure has long been recognized as an alternative to primary arthrodesis, which has demonstrated long-term success in pain relief, function and satisfaction rates.3,4 In addition, when compared with arthrodesis, first metatarsophalangeal joint arthroplasty has higher incidence of complications and hardware removal.
5
First metatarsophalangeal joint fusion following failed implant arthroplasty is often the only salvage procedure option. However, few studies exist that evaluate the success of first metatarsophalangeal joint arthrodesis following failed implant arthroplasty. “Investigation of fusion rates of first MTP joint arthrodesis after conversion from failed implant arthroplasty.”
A variety of products are currently available for first metatarsophalangeal joint arthroplasty, including silastic implants, polymer-based implants, polyethylene-on-metal and metal hemiarthroplasty implants. Still, the long-term efficacy of these implants remains highly variable, with the literature exhibiting revision rates for available implants ranging 5% to 74%.5 -13 Etiologies for various implant type failures include foreign body synovitis, clinical pain and deformation of joint supported by radiographic peri-prosthetic osteolysis, implant malalignment, direct implant fracture, indirect fracture caused by implant, and cystic bone formation.5,10,13,14
The goal of implant excision and subsequent joint fusion is to achieve pain relief, restore first ray length, and to reestablish limb function. Salvage procedures comprise of joint arthrodesis in combination with structural autograft bone, structural allograft bone, or distraction osteogenesis. 15 Current literature has documented fusion rates of several specific first metatarsophalangeal joint failed implant salvage procedures. However, a systematic review of the topic has yet to be created. The purpose of this study is to investigate the fusion rates of first MTP joint arthrodesis after conversion from implant arthroplasty.
Methods
We performed a systematic review of electronic databases and relevant peer-reviewed sources, including Cochrane, PubMed, and OvidSP Medline. We searched each identified study for pertinent references. Only those that involved first metatarsophalangeal arthroplasty or arthrodesis were included.
Three electronic databases, including Cochrane Database of Systematic Reviews (http://www.cochrane.org/reviews/; last accessed June 29, 2018); PubMed at (http://www.ncbi.nlm.nih.gov/pubmed/; last accessed June 3, 2018); and OvidSP Medline (http://ovidsp.tx.ovid.com/; last accessed July 14, 2018) were searched. No restrictions were placed on data or language. We performed the present systematic review in DATE with no restriction on the date or language, using an inclusive text word query “hallux” OR “great toe” OR “metatarsal-phalangeal” OR “metatarsophalangeal” AND “arthrodesis” OR “fusion” OR “arthroplasty” OR “replacement” OR “McKeever” OR “silastic” OR “Swanson” OR “implant” OR “union” OR “nonunion” where the uppercase words represent the Boolean operators used. Each investigator reviewed all manuscripts with unanimous decision used for final inclusion. The references from identified manuscripts were then manually searched for additional potentially pertinent published works, which were then secured for review.
To acquire the highest quality and most relevant studies available, the publications were eligible for inclusion only if they involved skeletally mature patients undergoing first metatarsophalangeal joint arthrodesis as a revision for failed implant arthroplasty. Studies additionally required mean follow-up of at least 6 weeks and inclusion of appropriate detail regarding complications, nonunion rates, and patient demographics. If a reference could not be obtained through purchase, library assistance, or electronic mail contact with the author, it was excluded. Case reports, studies involving the salvage of polyvinyl alcohol hemiarthroplasty, and other articles with less than 5 reported cases were excluded. Only references originally published in English were included.
Statistical analysis of the pooled data included the weighted mean, and the associated range for the duration of follow-up and patient age. The data were weighted as follows. For each sample size, the numeric results were summed and then divided by the total sample size for all included studies (ie, the weighted mean age was determined by taking the mean age for all patients in 1 study and multiplying it by the number of patients in the study and then repeating this for each study; total number was then divided by the total number of patients and resulted in the weighted mean age). A statistical description of the pooled data was then compiled and is provided in the present report.
A complication was defined as dehiscence, infection, hardware complications, deep venous thrombosis (DVT) or pulmonary embolus (PE), neurovascular injury, nonunion, or malunion. A reoperation was defined as an unplanned operation subsequent to the initial arthrodesis that was aimed to address a complication. A revision was defined as a reattempt at first metatarsophalangeal joint arthrodesis.
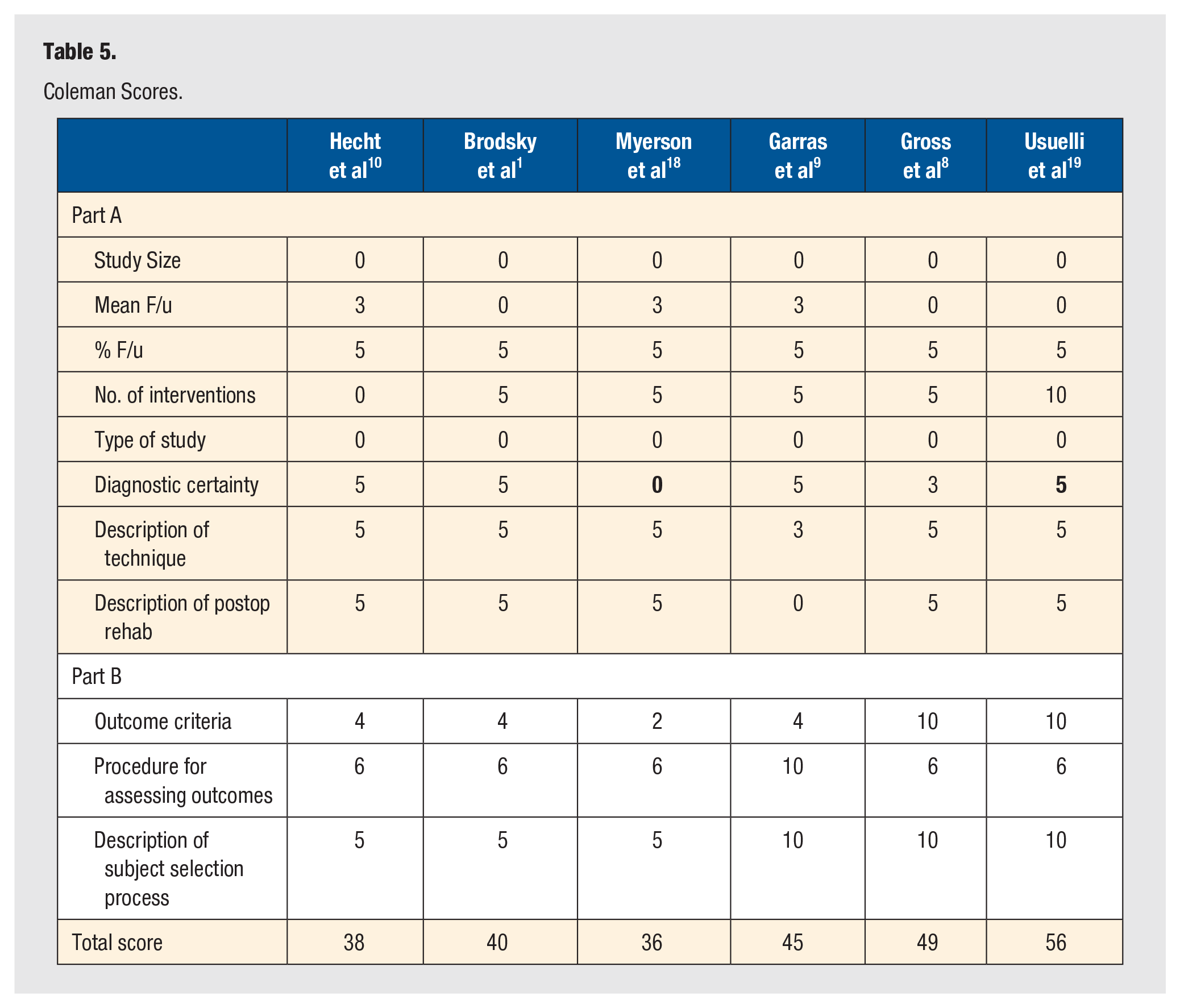
The guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) were used to design our review of the literature. PRISMA is a 27-item checklist that is intended to improve review quality. 16 This was supplemented by generating review quality scores. The methodological quality of the included studies was assessed using the Coleman Score. 17 A score of 100 indicates the most high-quality study with no confounding factors or other biases. Two independent reviewers (MW and AC) assessed the methodological quality of each included study. Conflicting scores for the various items were discussed until consensus was reached.
Results
The search for potentially eligible information for inclusion in the systematic review yielded a total of 3691 manuscripts. All references identified were obtained and reviewed by each investigator in July 2018. After considering all the potentially eligible references, 6 (0.16%) met our inclusion criteria (Figure 1). All included studies were retrospective case series. 1 ,8 -10,18,19 A total of 79 feet in 76 patients with a weighted mean age of 54.9 years, were included (Table 1). The most common indication for first MTP implant arthroplasty revision to arthrodesis was persistent pain in 86.1% (n = 68/79 feet), followed by aseptic implant loosening in 16.3% (n = 8/49 feet) and infection or septic implant loosening in 7.6% (n = 6/79 feet) (Table 2). Of the studies that reported interval time between the primary implant arthroplasty procedure and the revision arthrodesis procedure, the average duration was 42.0 months (Table 1).
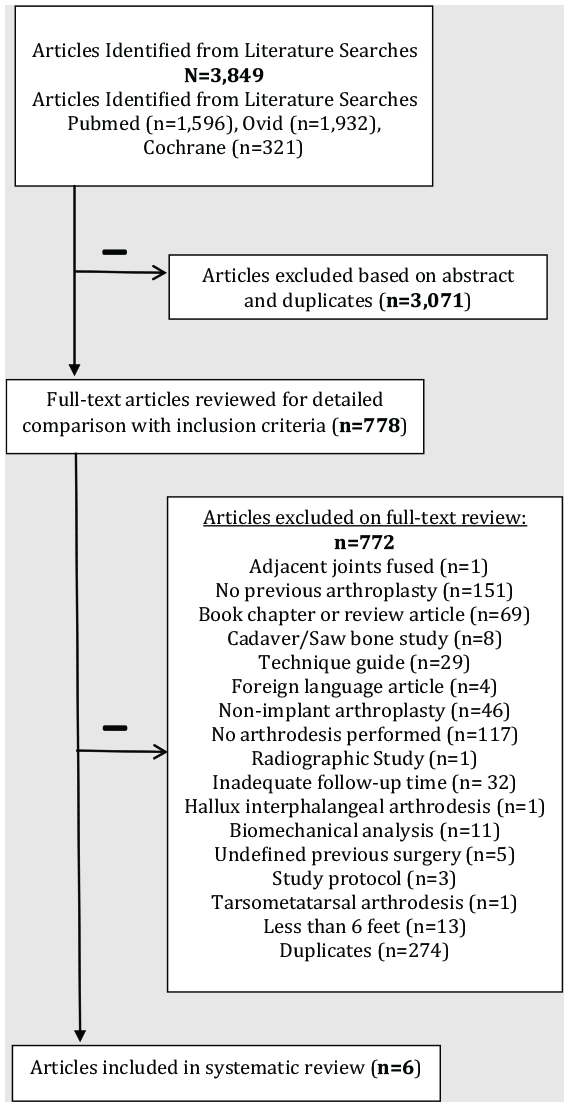
Flowchart of identified reports during selection process.
Demographic Data Included in Systematic Review.
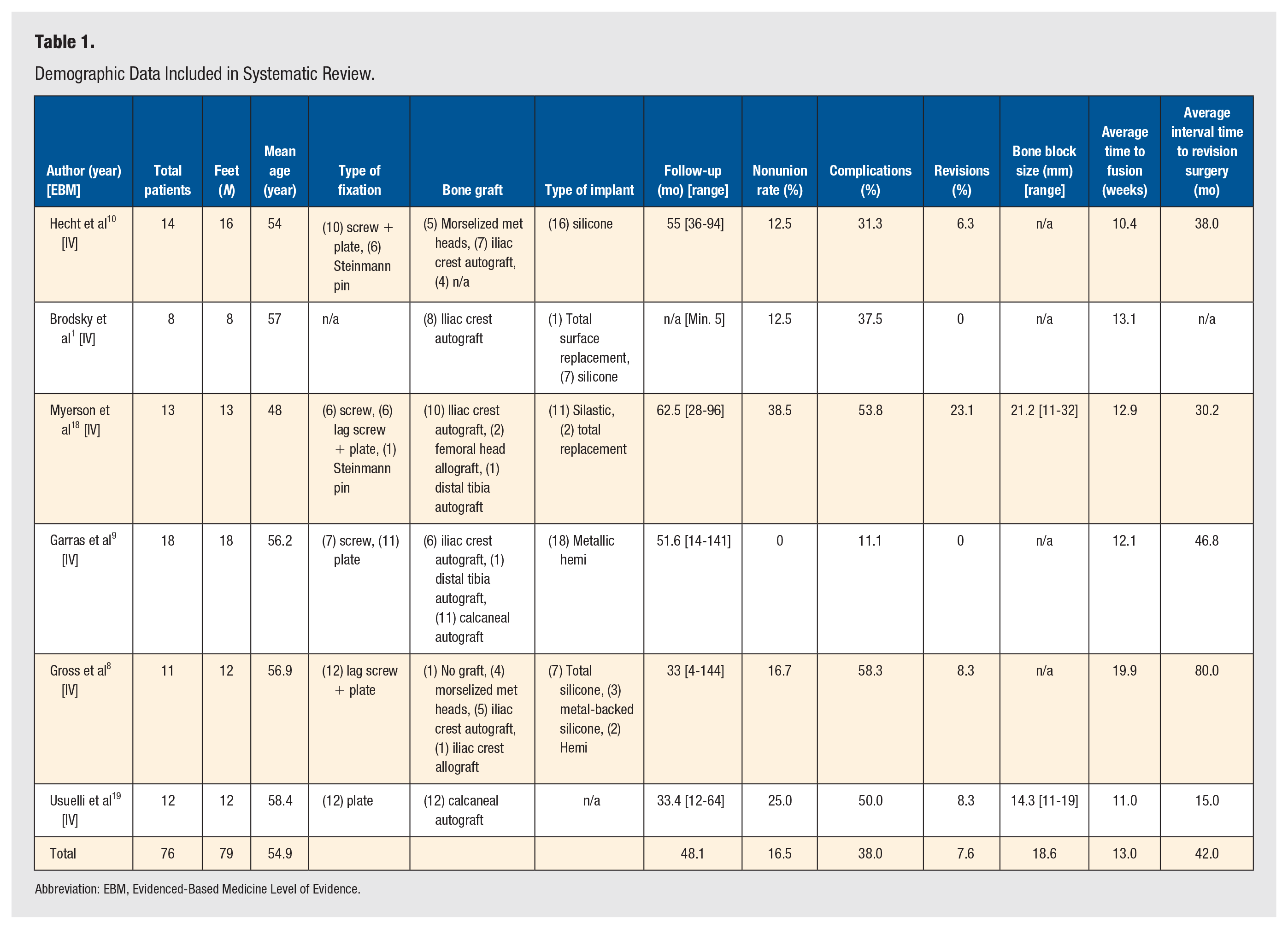
Abbreviation: EBM, Evidenced-Based Medicine Level of Evidence.
Etiology and Indication for Revision.
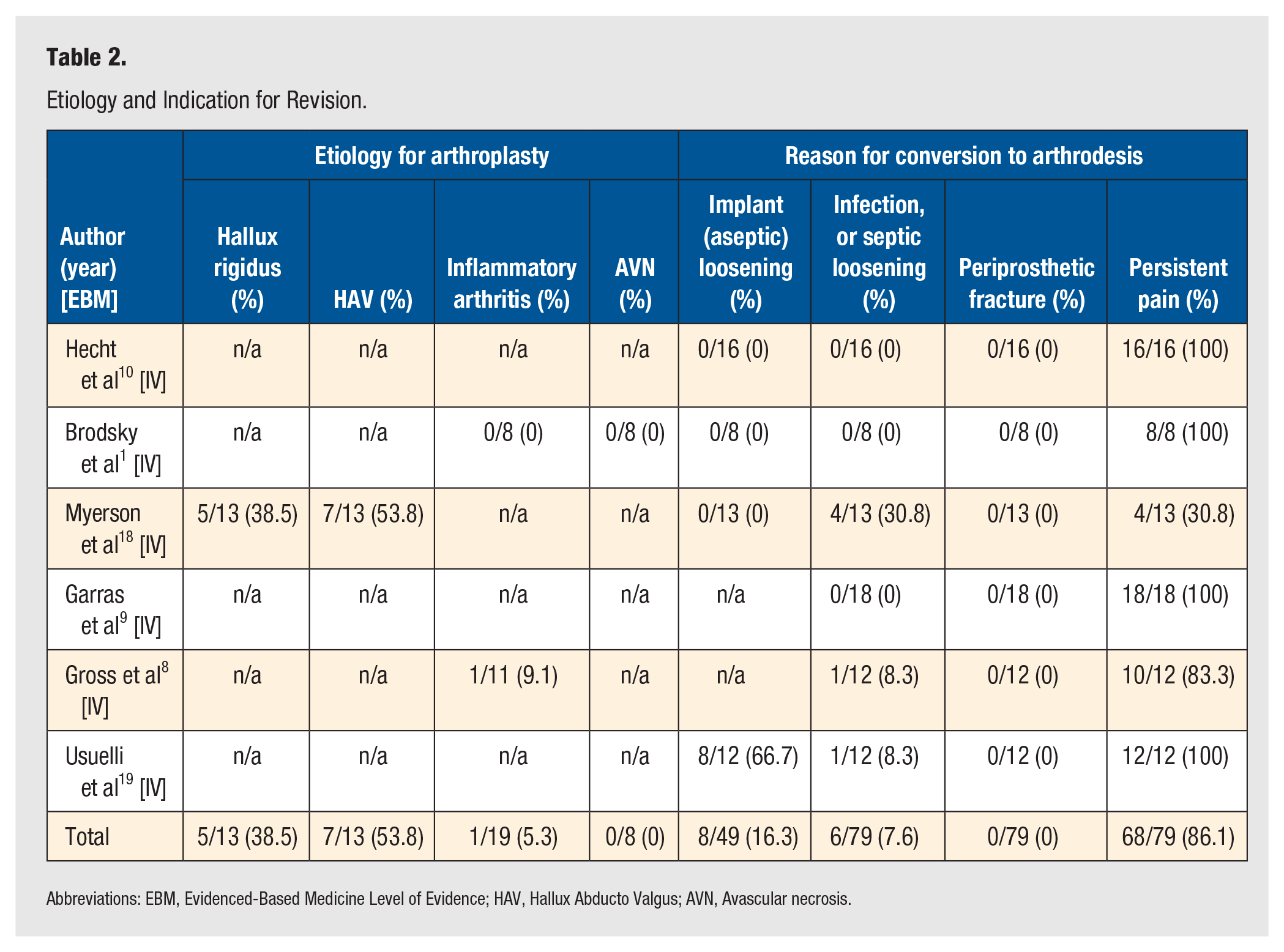
Abbreviations: EBM, Evidenced-Based Medicine Level of Evidence; HAV, Hallux Abducto Valgus; AVN, Avascular necrosis.
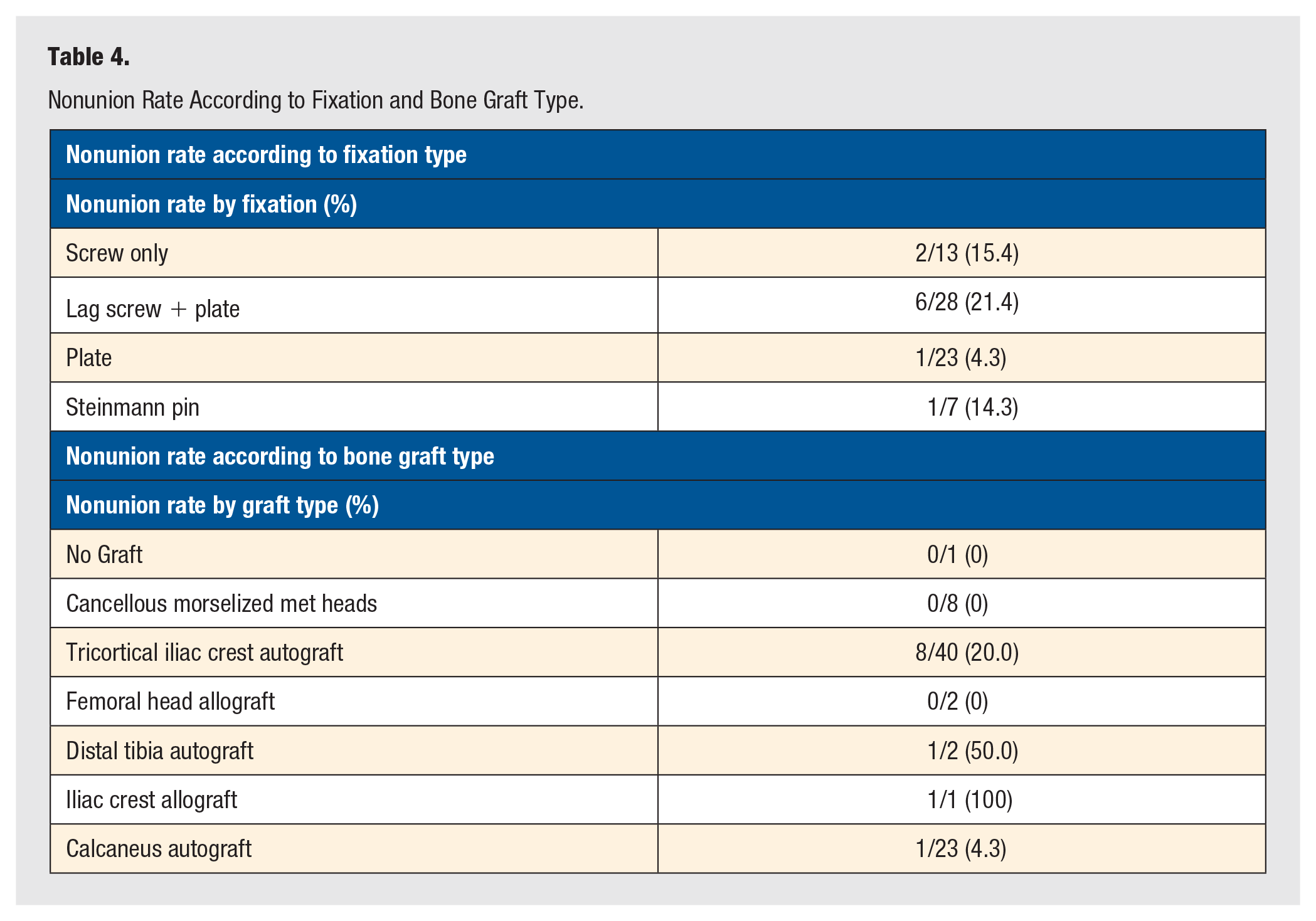
Out of the 6 included articles, radiographically confirmed nonunion rate was 16.5% (n = 13/79 feet) at a weighted mean follow-up of 48.1 months (Table 1). The average time to fusion was 13.0 weeks (Table 1). The revision rate for nonunion was 7.6% (n = 6/79 feet) (Table 1). The overall complication rate across all included studies was 38.0% (n = 30/79 feet) Hardware complications were the most common complication other than nonunion at 10.1% (n = 8/79 feet), followed by wound dehiscence at 6.3% (n = 5/79 feet) and superficial infection at 5.1% (n = 4/79 feet). The incidence of unplanned surgical removal of hardware occurred was 10.1% (n = 8/79) (Table 3). The overall incidence of reoperation was 15.2% (n = 12/79). There was a wide variety of bone graft types used, with iliac crest autograft most common at 48.0% (n = 36/75 feet), followed by calcaneal autograft at 30.7% (n = 23/75 feet) and morselized resected metatarsal heads at 12.0% (n = 9/75 feet). Of the 6 included studies, 2 reported the size of bone block used to fill bone deficits. Of these 2 studies, the average size of the bone block was 18.6mm (Table 1).18,19 The most common form of fixation that led to nonunion was combined screw and plate fixation with a nonunion rate of 21.4% (n = 6/28 feet) (Table 4). The most common bone grafting technique that led to nonunion was tricortical iliac crest autograft with a nonunion rate of 20.0% (n = 8/40 feet) (Table 4).
Complication and Reoperation Rate.
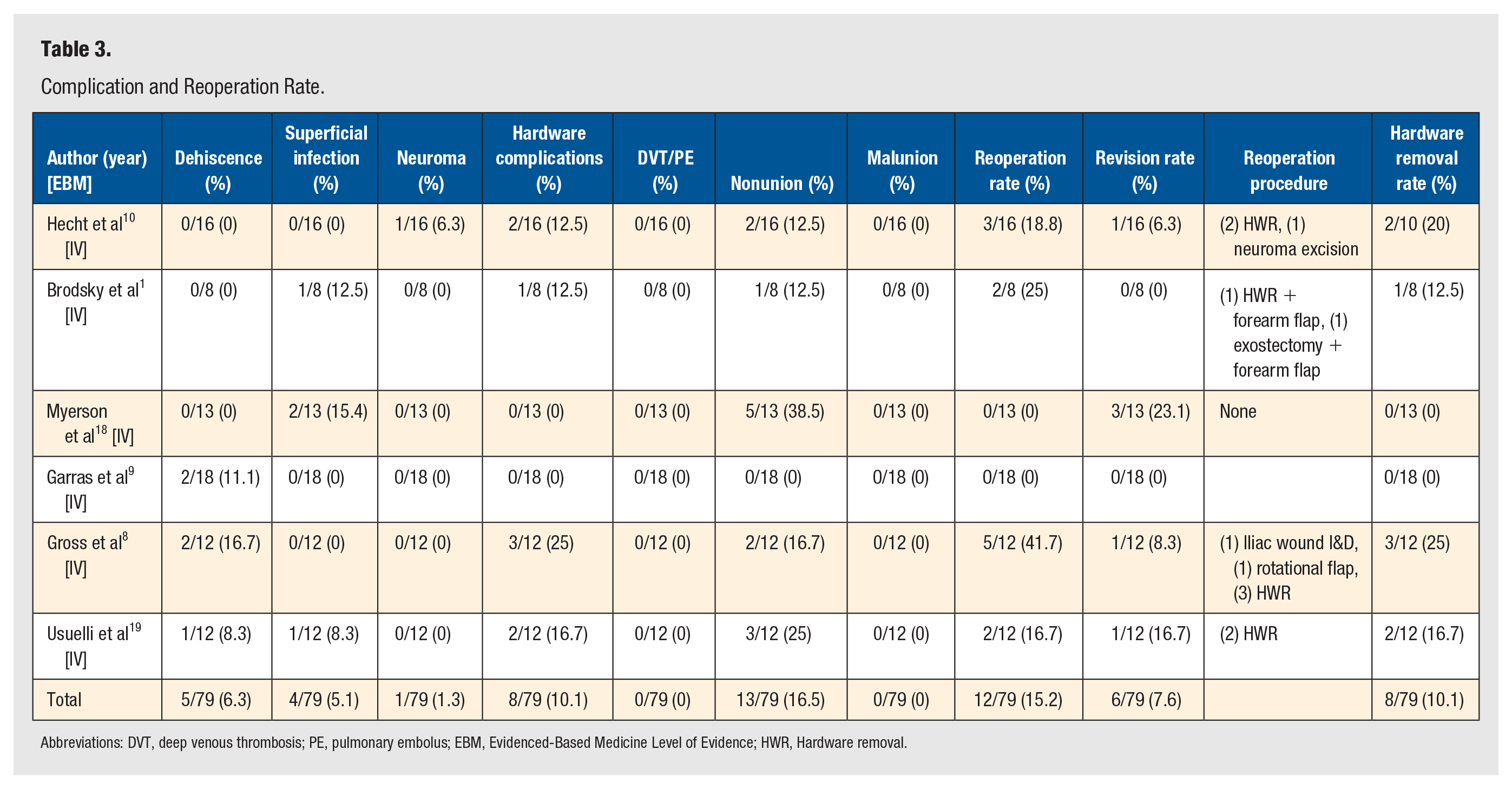
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolus; EBM, Evidenced-Based Medicine Level of Evidence; HWR, Hardware removal.
Nonunion Rate According to Fixation and Bone Graft Type.
The methodological quality of the included studies was generally poor. With regard to Coleman Score Appraisal of the included studies, zero scored above 70 (Table 5). The average Coleman score was 44 (range, 36-56) (Table 5). All included studies provided level IV evidence (Table 1). There was heterogeneity in study type, fixation technique, indications for surgery, and study size among the included studies (Table 1).
Coleman Scores.
Discussion
The purpose of the present systematic review was to evaluate the incidence of nonunion of first MTP joint arthrodesis as a salvage procedure for failed implant arthroplasty. Six studies were identified that met the inclusion criteria. 1 ,8 -10,18,19 Review of the presented data allows for some generalized statements regarding salvage arthrodesis of the first metatarsophalangeal joint. The incidence of nonunion is 16.5% at a weighted mean follow-up of 48.1 months. The weighted mean time to union was 13.0 weeks. The included references were retrospective case series, which may be prone to selection bias. There was considerable variability and heterogeneity among included surgical techniques and reported outcome scores (Table 5). In addition, subgroup or meta-analysis comparing incidence of nonunion among various fixation constructs and bone grafting techniques lacked appropriate power to provide meaningful results. As data are presented using weighted means and summed percentages, the results should be interpreted with caution. Plain radiographs are commonly used to assess union of arthrodesis; however, studies have shown radiographs to be of limited capacity in determining osseous union. 20 In practice, clinical evaluation is essential and incorporates an assessment of pain, tenderness, and inability to bear weight. Details of these factors were not presented in the reviewed studies. Furthermore, the definition of nonunion was not standardized in the included reports. 1 ,8 -10,18,19
In a biomechanical study comparing 5 different fixation constructs for the first MTP joint, the most stable technique for obtaining fusion was the combination of an oblique lag screw and a dorsal plate. 21 The addition of a lag screw to a dorsal locking plate improves stability and union rates compared with dorsal locking plate alone.22,23 Interestingly, nonunion in the current systematic review was most notable with a plate and screw fixation technique (Table 4). This finding raises the question of the optimal fixation technique in the setting of salvage arthrodesis and structural bone graft.
The incidence of nonunion was highest with the use of iliac crest bone autograft (Table 4). Iliac crest bone autograft is accepted to be the “gold standard” bone graft, despite its known morbidities. 24 In a previous systematic review investigating outcomes of first MTP joint arthrodesis using autogenous iliac crest bone after failed Keller-Brandes resection arthroplasty, nonunion rate was reported to be 4.8%. 25 This differs greatly from the nonunion rate of 16.5% found in the current systematic review. One possible reason for this difference is an increased osseous defect both during implantation and removal of the implant during first MTP joint replacement, when compared with resection arthroplasty without implant. The use of autograft presents a challenge to precisely contour the structural graft to regain maximum length while achieving appropriate axial and sagittal plane alignment, and is even more challenging to achieve consistent union at 2 primary bone-healing interfaces. The bone defect left secondary to bone resection and osteolysis can be difficult to revise and often requires a segmental bone graft.1,26 As a consequence of greater bone resection at the time of implant arthroplasty, the nonunion rate of salvage arthrodesis is higher compared with primary arthrodesis of the first MTP joint according to historical data. In a systematic review after primary arthrodesis of the first MTP joint, the nonunion rate was found to be 5.4%. 27 The weighted mean interval to radiographic union was 64.3 days or approximately 9 weeks. 27 Therefore, according to historical data, the rate of nonunion after primary arthrodesis is considerably lower and time to union is shorter compared with salvage arthrodesis after failed implant arthroplasty compared with primary arthrodesis. In addition, our finding of complications in 38.0% (Table 3) further reiterates the challenge of these salvage cases. Further research should emphasize the optimal biologic environment to promote osseous union for salvage arthrodesis of the first MTP joint.
Weaknesses of this study are acknowledged. The search for references for inclusion was performed using an electronic database. Although relevant peer-reviewed journals were also manually searched, it is possible that not all pertinent references were identified by our methods. The inclusion criteria for our study included only articles written in the English language. This may have excluded studies that could have otherwise affected our conclusions, and it may have given bias toward research emanating from English speaking countries. Only published data are included in this trial, and thus our conclusions must be interpreted in light of the publication bias. In clinical practice, salvage first MTP arthrodesis for failed first MTP implant arthroplasty may be less efficacious than it would appear in this review due to less successful results being less likely to be published. It should be noted that despite recent studies reporting data using polyvinyl alcohol hydrogel implants, these studies were excluded from the current systematic review due to the lack of robust long-term outcomes in the first MTP joint. In conjunction with the paucity of high-quality evidence regarding clinical and functional outcomes, practical concerns still exist regarding optimal preparation fixation technique and surgical indications.
Strengths of this study include unanimous agreement regarding included studies and inclusion criteria. There is clarity and reproducibility of our search strategy using multiple evidence-based databases. PRISMA guidelines for the reporting of systematic reviews were used throughout in order to increase transparency and reduce the risk of publication bias. 16 The mean follow-up time of 48.1 months is of clinical importance. Lastly, there are no previous guidelines or meta-analyses to determine the nonunion rate of first MTP joint arthrodesis as a revision exclusively for failed implant arthroplasty. Thus, the current systematic review is the first study to address this gap in knowledge.
In conclusion, our pooled results demonstrate that first MTP joint arthrodesis remains a useful salvage procedure to manage large osseous voids and compromised anatomy after failed implant arthroplasty with unavoidable nonunion and complication rates. The identified weighted nonunion rate is 16.5% at weighted mean follow-up of 48.1 months for first metatarsophalangeal arthrodesis as salvage for failed implant arthroplasty. Resultant to the significant nonunion rate for this salvage procedure, proper patient counseling of risks, benefits, complications, and potential outcomes is paramount prior to performing this revision procedure. Moreover, proper patient counseling is equally imperative prior to the index first MTP implant arthroplasty procedure, so the patient is appropriately educated regarding the complexity and risks associated with the anticipated salvage procedure in the event of failure of the index arthroplasty procedure. Further research is warranted, including methodologically sound, appropriately powered prospective cohort studies focusing on long-term outcomes comparing joint preparation techniques and fixation constructs. Beyond the need for standardized patient reported outcomes, additional outcome measures should include union rates, functional assessment, complications and cost-benefit analysis. The evidence in the current literature precludes strong recommendations with regard to any singular fixation construct, bone graft type, or surgical technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.