
Abstract
Background:
Intraosseous talar tumors are rare and usually require complex surgery such as tibiocalcaneal fusion with allograft, resulting in a poor functional outcome. Total talus replacement (TTR) has been primarily described predominantly after trauma for talar avascular necrosis in the absence of peri-talar arthrosis. We present our small initial case series of this novel indication for a TTR to treat a localized talus tumor with no associated osteoarthritis.
Methods:
Four patients underwent total talus replacement with a custom-made 3D-printed talar implant for an isolated intraosseous talar tumor between February 2021 and December 2022. The pathologies were fibrous dysplasia, a primary vascular tumor, and 2 cases each with an isolated metastatic endometrial carcinoma. All 4 cases were performed by the same surgical team. The Manchester-Oxford Foot Questionnaire (MOXFQ) and EuroQoL–5 Dimensions (EQ-5D) questionnaire were recorded pre- and postoperatively.
Results:
At a mean follow-up of 26 months (range, 14-37) all our patients showed an improvement in their MOXFQ and EQ-5D scores. Average MOXFQ scores decreased from 57.3 to 20.3. Three of the 4 patients showed an improvement in their function and ability to perform usual activities. One patient scored an improvement in their mobility. None had any intraoperative or postoperative complications.
Conclusion:
TTR is an alternative technique for the management of isolated talar tumors, which will maintain movement and provide better function than previous options.
This is a visual representation of the abstract.
Introduction
Complex talar pathology such as avascular necrosis, post-traumatic talar deformity or talar tumors, pose a difficult treatment challenge for any foot and ankle surgeon. 10 Management options include pantalar fusion, tibiotalocalcaneal fusion with or without allograft, or a talectomy with tibiocalcaneal fusion. With the latter procedure in particular, the resulting leg length discrepancy may require tibial lengthening procedures. Although these procedures provide a stable limb for ambulation, they have a long recovery period, high complication rate, and at best achieve an inefficient gait and suboptimal functional outcomes.7,13 Over the past few years, total talus replacement (TTR) has increased in popularity as an alternative treatment option for chronic avascular necrosis or acute talar fractures or extrusion. 7 Bone tumors isolated entirely within the talus are rare conditions. Usually there is limited access to the tumor, which even when still contained may have already caused articular damage. They are especially challenging to treat and have needed significant bone grafting of a large bone void created after removal of the tumor or pseudo-tumor. We present our case series of total talus replacements performed in a single quaternary referral unit for isolated talar tumors.
Methods
Case Series
Four patients underwent total talus replacement with a custom made talar implant between February 2021 and December 2022. The selected patients had isolated talar disease involving >50% of their talar volume without degeneration of the adjacent joint surfaces; and would have previously undergone a salvage procedure in the form of a tibiocalcaneal or tibiotalocalcaneal fusion. Case 1 was a 14-year-old female adolescent with polyostotic fibrous dysplasia with associated collapse of the talar dome and irregularity of the talar articular surface secondary to the condition (Figure 1A). She had previously undergone 2 arthroscopic ankle debridements. However, because of the progressive collapse of the subchondral bone of her talar dome, her pain deteriorated further, such that she was struggling to attend school. The alternative management of tibiotalar fusion was discussed with the family. There was no role for stabilization with a structural bone graft because the talar articular surface was destroyed. Case 2 was a 34-year-old man with an arteriovenous malformation involving the entire talus and with extraosseous soft tissue extension (Figure 2A). Following discussion in the sarcoma multidisciplinary team (MDT) meeting, the vascular surgeons deemed that the patient was not a suitable candidate for any interventional radiologic procedures. Both case 3 (Figure 3) and case 4 (Figure 4) had isolated endometrial metastases in the talus. In the hindfoot, strict wide local excision is compatible with the maintenance of joint movement as it would destroy the essential stabilizing features of the ankle and subtalar joints. Case 3 did not require any neoadjuvant or adjuvant chemo- or radiotherapy. However, case 4 was found to have further metastasis postoperatively and was given adjuvant chemotherapy and palliative radiotherapy. None of the 4 patients exhibited clinical signs or 3-dimensional imaging appearances of adjacent joint osteoarthritis. All patients were discussed in the Foot and Ankle MDT meeting and in the Sarcoma MDT. In addition, the 14-year-old patient received ethical clearance after discussion in the Pediatric MDT.
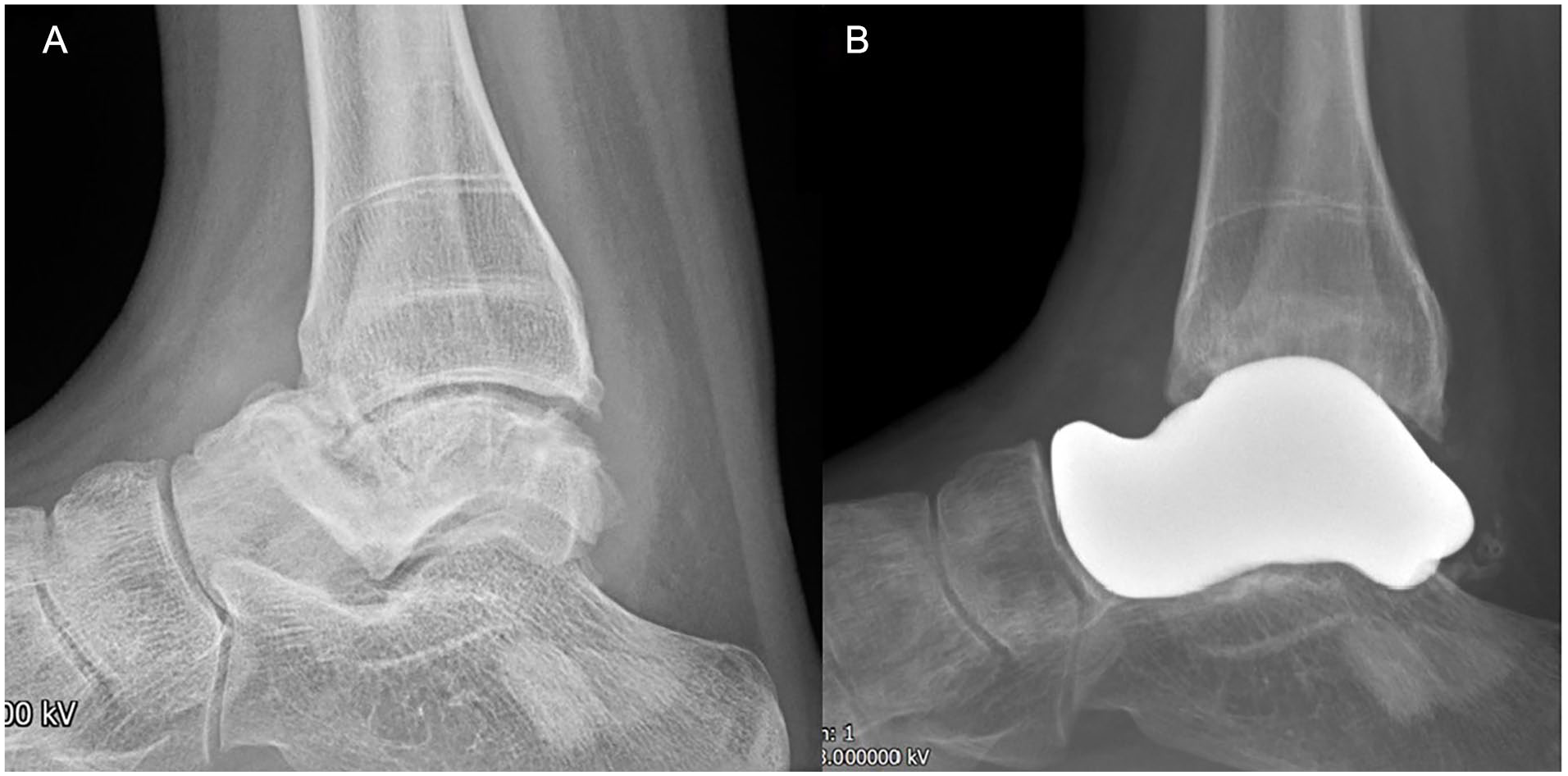
Lateral radiographs of patient 1 with polyostotic fibrous dysplasia (A) preoperatively and (B) postoperatively.

Patient 2 imaging. (A) Sagittal MRI view showing the arteriovenous malformation involving the entire talus and with extraosseous soft tissue extension. (B) Postoperative lateral radiograph.

Preoperative sagittal magnetic resonance imaging cut of patient 3 showing an isolated endometrial metastasis to the talus.

Preoperative sagittal magnetic resonance imaging cut of patient 4 showing an isolated endometrial metastasis with near complete involvement of the entire talus and extraosseous extension.
Clinical and radiologic data were collected during preoperative and routine postoperative visits. All patients underwent standing radiographs and had a computed tomography (CT) scan of both ankles preoperatively. Follow-up was at 2 weeks, 6 weeks, 12 weeks, 6 months, and 12 months, with radiographs taken at 2 and 6 months and 1 year. Further biannual radiographic and clinical follow-up will be undertaken.
Patient-reported outcome scores were collected preoperatively and at their most recent clinic appointment. The Manchester-Oxford Foot Questionnaire (MOXFQ) was used to assess functional outcome, and the EuroQoL–5 Dimensions (EQ-5D) score was used to assess health-related quality of life.
Preoperative Planning and Implant Manufacturing
The patient’s preoperative CT scans were used to design the custom-made talar implant. The images were converted into a computer-aided design (CAD) format and reconstructions of both the ipsilateral diseased talus and the contralateral normal talus were created. The reconstructions of the 2 images were superimposed onto each other to determine the extent of bone loss, talar collapse, or extrusion of the diseased talus (Figure 5). The lead author adjusted the design in 3 dimensions to compensate for these deformities. In cases where there had been a significant loss of talar height, the decision was made for the height of the talar prosthesis to be 50% between that of the damaged and the undamaged contralateral talus. The CAD directed the additive manufacturing (3-dimensional [3D]) printing of the final implants. The implants are coated with titanium niobium. In this early series, we created 100%, 90%, and 80% titanium implants as well as nylon trials (Figure 6). Sterile 3D models of the hindfoot anatomy were also made for use in the operating room to rehearse the reduction maneuver (Figure 7).

Auto-CAD reconstruction of contralateral normal talus superimposed onto diseased ipsilateral talus.

Operating room tray containing 2 nylon trial handles and the 80%, 90%, and 100% nylon trials and titanium implants.

3D model of the hindfoot anatomy for use in the operating room showing the total talus replacement sitting within the mortise.
Operative Technique
The procedure was performed by the same surgical team for all cases. The patients were positioned supine and a thigh pneumatic tourniquet used throughout the procedure. A standard anterior approach to the ankle was used with Z-opening of the extensor retinaculum. A coronal osteotomy was performed through the talar neck with an osteotome to allow easy resection of the head of the talus. The entire talus was collected and sent for histopathologic examination. Subsequent progressive sagittal cuts into the talar body permitted complete removal of the talus without penetrating the joint capsule, which was especially important in the 2 metastatic malignant cases to reduce the risk of tumor seeding. For both the benign and the malignant conditions, care was taken to minimize dissection beyond the capsule, and the surgical site was lavaged with water. Complete removal of the talus was confirmed with the image intensifier. A vascular surgeon was present in the operating room for the primary vascular tumor.
The 90% and then 100% trials were reduced into the joint to assess which model provided the best stability, and the corresponding customized implant was inserted (Figure 8). In all 4 cases, the 100% trial reduced well and was stable. Finally, the range of movement of the ankle and subtalar joints was assessed on table and static fluoroscopic images taken.

Intraoperative photograph of Patient 2’s ankle with final implant in situ.
Postoperatively, all patients were put into a below-knee removeable fiber cast and advised not to bear weight until the wound healed at around 2 weeks. They were subsequently allowed to fully bear weight in a new below-the-knee cast that was worn until 6 weeks in order to allow the lateral and deltoid ligaments to tighten by scar contraction. At 6 weeks postoperatively, the cast was removed and patients were given gentle mobilization exercises of the ankle. Postoperative radiographs for patients 1 and 2 can be seen in Figures 1b and 2b. Patients were advised to avoid impact sports indefinitely.
Results
There were 3 females and 1 male in our case series with an average age of 46 years (range, 14-69) at the time of their procedure. Patient demographics and outcomes are shown in Tables 1 and 2. Patients were followed up for an average of 26 months (range, 14-37). At their latest follow-up visit, hindfoot alignment was maintained with persistence of the good range of movement of both the ankle and subtalar joints. The anterior talofibular, calcaneofibular, and deltoid ligaments remained stable to stress testing with no delayed development of laxity. MOXFQ scores of the 3 adults improved from an average of 57.3 to 20.3 postoperatively. MOXFQ scores for our pediatric patient were not included because the score is not validated for use in pediatric patients. With regard to the EQ-5D scores (Table 2), 3 patients scored an improvement in their function and ability to perform usual activities. Only 1 patient scored an improvement in their mobility.
Patient Demographics and MOXFQ Outcome Scores.

Abbreviations: MOXFQ, Manchester-Oxford Foot Questionnaire; TTR, total talus replacement.
Preoperative and Postoperative EQ-5D Scores.

Abbreviation: EQ-5D, EuroQol–5 Dimensions.
1 = no problems, 2 = some problems, 3 = confined to bed.
1 = no problems, 2 = some problems, 3 = unable to wash/dress myself
1 = no problems, 2 = some problems, 3 = unable to perform usual activities
1 = no pain/discomfort, 2 = moderate pain/discomfort, 3 = extreme pain/discomfort
1 = not anxious/depressed, 2 = moderately anxious/depressed, 3 = extremely anxious/depressed.
None of our patients had any intraoperative or postoperative complications. Postoperative radiologic assessment showed no evidence of early wear at any of the neighboring joints.
Discussion
The use of total talus replacements has increased recently with advances in additive manufacturing. 8 The unique anatomy of the talus and its lack of tendon attachment makes it possible for an anatomical implant to be inserted, theoretically with good functional outcomes. 1 Furthermore, the complexity of current surgical solutions (and their complications) used to manage talar pathology drives the need to improve the design of talar replacement and consider further novel indications.
The first talus replacement was inserted in 1974 in Thailand. 4 These first-generation partial implants consisted of a 316L stainless steel talar body implant with an anterior stem cemented into the talar neck. Slit-scanograms of the contralateral normal talus were used to design and size the final implant. The procedure was performed using a transmedial malleolar approach. All but 2 of the 16 patients had satisfactory results in Harnroongroj’s series with an average of 9.9 years’ follow-up. One patient was revised at 8 months postoperatively to an arthrodesis because of erosion of the posterior facet of the subtalar joint, whereas the second patient was revised at 13 years postoperatively to another talar implant of the same size because of erosion into the talar head. In 2014, the same authors subsequently published a long-term follow-up study of between 10 and 36 years. 5 Four cases failed within 5 years of their primary procedure because of size mismatch, infection, and talar head and neck osteonecrosis. The remainder of the surviving implants showed promising results with mean American Orthopaedic Foot & Ankle Society (AOFAS) ankle- hindfoot scores of 75 at a minimum 10-year follow-up, and 74 at a minimum 20-year follow-up, which was maintained for the partial talus replacements that reached at minimum 30-year follow-up. Of relevance to this study, one of the 33 patients included in their early study had been diagnosed to have a benign giant cell tumor of bone. However, this patient developed a malignant transformation after 5 years and needed a below-knee amputation.
In 2012, Taniguchi et al 12 published his results of 22 partial talus replacements, which were ceramic talar body implants for avascular necrosis. Their initial design of implant included a peg for insertion into the talar neck and was used in 8 patients. Within a year there was radiologic evidence of loosening around the peg and talar head necrosis in all 8 patients. This prompted a design change to a second-generation partial replacement implant without a peg with the aim of reducing stresses at the fixation point. AOFAS scores were favorable in 57% of their patients. However, 2 of the 14 patients required revision to a total talus replacement because of severe loosening, talar neck fractures, or head fractures. Therefore, because of the high complication rate, the authors did not recommend partial talar replacements for the management of avascular necrosis and advised total talus replacements instead.
The current third-generation implants are true total talar replacements. With the evolution of 3D printing, patient-specific custom-made implants can be made using the patients’ preoperative CT images. This ensures near-native joint congruence 6 and reduces the risk of size mismatch. Total talus replacements have been made using stainless steel, alumina ceramic, and cobalt chrome. 6 However, titanium implants are becoming more popular because of better tribologic properties.6,14
The short-term advantages of a total talus replacement include reduced stiffness, less limb length discrepancy, faster pain relief, prompter recovery, shorter period of cast immobilization, and less restriction of weightbearing. The long-term advantage is that it may delay the need for a future complex fusion procedure. In a recent systematic review published in 2023, 68.4% of 80 patients receiving an isolated TTR showed a significant improvement in their functional outcome score. 6
In patients with adjacent tibial plafond osteoarthritis, current implants can also be linked with a customized tibial component and polyethylene insert. This will need to be followed as a distinct group in arthroplasty registries. In the 2023 review, the smaller number of patients who had a TTR with an associated tibial prosthesis had an improved postoperative range of ankle dorsiflexion and total range of movement but also only a nonsignificant trend toward improvement in functional scores. 6
Similarly, another group of customized implants exist where the talus is replaced and additionally the prosthesis is fixed to the calcaneum. These will also need distinct long-term study.
The most common indication for TTR is avascular necrosis, with a recent literature review reporting that 67 of the 115 (58%) TTRs reported by 2023 had undergone surgery for avascular necrosis. 6 There is sparse literature on the use of total talus replacements in tumor cases. To our knowledge, there were no case series of fully articulating total talus replacements. There are case reports describing use of a total talus replacement with calcaneal fixation. Fang et al 3 presented a single case report of their technique of using a press-fit implant for a malignant mesenchymal sarcoma of the talar body in West China. The implant consisted of a superior modular component of ultrahigh-molecular-weight polyethylene for articulation with the ankle mortise and an inferior porous titanium alloy component for articulation with the calcaneus and navicular. It also had predrilled holes for fixation into the calcaneus and navicular to further stabilize the arthrodesis. At 6 months, their patient was tumor-free and scored an improvement in the Musculoskeletal Tumour Society (MSTS) score from 19 to 26 and an AOFAS score from 73 to 91. In 2021, Yang et al 15 reported a single procedure in their patient who had a giant cell tumor of the bone involving the talus, managed with a 3D-printed talar prosthesis, with 2 screw channels for fixation to the calcaneum and a porous undersurface to aid bony ingrowth. At only the 6-month follow-up, they reported a comparable AOFAS score of 89. Below-knee amputation is another alternative treatment option, especially for complex unreconstructible foot tumors. Both Refaat et al 11 and Zahlten-Hinguranage et al 16 showed minimal difference in quality of life between amputation and reconstruction for lower limb sarcoma, but their data were not specific for the foot. More recently, however, limb salvage has resulted in good functional outcomes, scoring higher than for amputation.2,9
In our series, the implants used were 3D-printed out of titanium and then coated in titanium niobium to produce a polished smooth surface. Initially, three sizes of trials and implants were manufactured; however, because only the 100% implant was being used, we have discontinued making the 80% implant, which helped reduce the costs.
At a minimum of 14 months, our patients showed an improvement in their functional scores that is similar to what is seen in the literature for TTRs used for posttraumatic conditions. However, the more general quality of life score EQ-5D showed much less improvement in our patients. We believe this to be due to the complex systematic nature of the underlying conditions. For example, our first patient with polyostotic fibrous dysplasia, who is the youngest described in the literature receiving a TTR, had to undergo subsequent hip surgery. Furthermore, one of the patients believed to have an isolated endometrial carcinoma developed micro-metastases requiring further chemotherapy. All these other interventions lead to a reduced overall EQ-5D score. Our key objective was to improve our patients’ mobility and ability to perform activities of daily living, which was confirmed both on the MOXFQ and the subcomponents of the EQ-5D.
This technique of intralesional resection is appropriate for benign and isolated metastatic lesions, but we think it would not be appropriate for a primary malignant talar tumor.
Despite the favorable clinical results of TTRs, the cost of the implant remains a concern. The design and manufacturing of the trials and implants in this early series costs approximately £12,000 (2021-22) and are therefore not easily available in all hospitals. However, price in 2024 has fallen to £6000, as our unit performs more of these procedures. The manufacturing and preparation of this implant involves stages in Milan, Italy, and the United Kingdom requiring a minimum of 4 weeks. The use of a TTR in the management of isolated tumors of the talus must be performed in cooperation with a regional tumor service. The patients in our small case series continue under medium-term follow-up.
Conclusion
Total talus replacement is a promising alternative treatment option for isolated tumors involving destruction of the talus and no adjacent joint arthritis. Careful patient selection and preoperative planning must be combined with close adherence to appropriate tumor resection principles.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251318732 – Supplemental material for A Novel Indication for 3D-Printed Titanium Total Talus Replacements in Isolated Talar Tumors
Supplemental material, sj-pdf-1-fao-10.1177_24730114251318732 for A Novel Indication for 3D-Printed Titanium Total Talus Replacements in Isolated Talar Tumors by Martina Galea Wismayer, Harriet Branford-White, Mark B. Davies and Rick Brown in Foot & Ankle Orthopaedics
Footnotes
Ethical approval
Ethical approval for this study was waived by UKRI Medical Research Council Review and IRAS assessment. Hospital Trust approval was granted.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mark B. Davies, BM, FRCS(Tr&Orth), reports disclosures relevant to manuscript from MeshWorks, Alloyed, and Oxford: consultancy and royalty payments. NB MeshWorks products were used in this study, but they manufacture custom talus replacements. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.