
Abstract
Background:
Treatment of osteonecrosis of the talus is challenging. Nonoperative management includes nonweightbearing treatment. Various types of hindfoot fusion procedures have been performed, but delayed union and shortening of the operated leg have reportedly occurred. In contrast, talar body prosthesis is a surgical procedure with potential that relieves pain, restores ankle joint function, and is not associated with leg-length discrepancy. The aim of this study was to investigate postoperative pain, clinical outcomes, activities of daily living (ADL), and quality of life (QOL) after total talar replacement in patients with osteonecrosis of the talus.
Methods:
Ten ankles in 10 patients with idiopathic osteonecrosis of the talus who were treated with a total talar replacement between 2007 and 2015 were included in the investigation. Scores according to the visual analog scale (VAS), Japanese Society for Surgery of the Foot (JSSF) ankle-hindfoot scale, Functional Independence Measure (FIM), and the Self-Administered Foot Evaluation Questionnaire (SAFE-Q) were assessed.
Results:
The VAS score significantly improved from a mean of 80 ± 8 points before surgery to 18 ± 22 points after surgery (P < .01). The JSSF ankle-hindfoot scale score significantly improved from a mean of 53 ± 12 points before surgery to 89 ± 7 points after surgery (P < .01). The FIM score significantly improved from a mean of 122 ± 1 points before surgery to 125 ± 1 points after surgery (P < .01). The mean postoperative SAFE-Q scores were as follows: 81 ± 10.3 points for pain, 78 ± 14.7 points for physical function, 90 ± 12.4 points for social function, and 83 ± 15.4 points for shoe-related.
Conclusion:
Total talar replacement is a useful treatment for patients with osteonecrosis of the talus. This replacement surgery preserves the function of the ankle and subtalar joints, and improves pain, ADL, and QOL.
Level of Evidence:
Level IV, case series.
Introduction
Treatment of osteonecrosis of the talus is quite challenging. Nonoperative management includes nonweightbearing for as long as 9 months with a patellar tendon-bearing brace.3,5,23 Various types of hindfoot fusion procedures have been performed, but delayed union and shortening of the operated leg have reportedly occurred.2,12,14,31 In contrast, talar body prosthesis, first introduced by Harnroongroj and Harnroongroj 6 and Harnroongroj and Vanadurongwan 7 is a surgical procedure that relieves pain, restores ankle joint function, and is not associated with leg-length discrepancy. Harnroongroj et al in 36 cases of stainless-steel talar body prosthesis, and Taniguchi et al26,27 in 55 cases of custom-made total talar prosthesis made of alumina ceramic designed with computed tomography (CT) from the healthy side, reported good surgical results. The aim of this study was to report on clinical outcomes, pain, activities of daily living (ADL), and quality of life (QOL) in patients with idiopathic osteonecrosis of the talus treated with a custom-made total talar prosthesis made of alumina ceramic (Figures 1 and 2).

Total talar prosthesis was custom-made from CT of the healthy side. (A) Lateral view. (B) Top view.

(A) Preoperative radiograph of the ankle. (B) Sagittal T1-weighted magnetic resonance image (MRI) shows a low-intensity area in the talus where osteonecrosis is seen. (C) Axial T2-weighted MRI shows a low intensity area in the talus where osteonecrosis is seen. (D) Radiograph after total talar replacement.
Materials and Methods
Between March 2007 and January 2015, 10 patients (10 ankles) with idiopathic osteonecrosis of the talus underwent total talar replacement in our hospital. We used a custom-made ceramic total talar prosthesis made using CT on the healthy side of the patient. Total talar replacement is surgery to remove a necrotic talus and insert a prosthesis. A below-knee walking cast is applied for 3 weeks. Weightbearing is avoided in the first week, partial weightbearing is allowed in the second week, and full weightbearing is allowed in the third week. 28 All surgeries were performed by 1 surgeon. All patients were women with a mean age of 65 ± 10.9 (range, 42-86) years and had idiopathic osteonecrosis of the talus. None was caused by alcohol abuse or steroids (Table 1). Patients were assessed clinically preoperatively and postoperatively at the time of the final examination using the scores of the visual analog scale (VAS), Japanese Society for Surgery of the foot (JSSF) ankle-hindfoot scale,19,20 Functional Independence Measure (FIM), 4 and Self-Administered Foot Evaluation Questionnaire (SAFE-Q).21,22 Patients’ range of motion of the ankle and ADL were also assessed. All patients were able to be followed up and evaluated. Evaluation was performed by 1 doctor.
Demographics of Patients (N = 10).

The Wilcoxon signed rank test was used to compare variables. A P value of <.05 was considered to be significant.
Results
The mean follow-up time was 5 ± 3 (range, 2-10) years. The mean VAS score was significantly reduced from 80 ± 8 (range, 68-92) preoperatively to 18 ± 22 (range, 0-66) postoperatively (P < .01, Wilcoxon signed rank test) (Figure 3). Postoperative VAS score was 0 in 4 cases, 10 to 20 in 4 cases, and 50 to 70 in 2 cases. The mean JSSF ankle-hindfoot scale score significantly improved from 53 ± 12 (range, 26-62) points to 89 ± 7 (range, 81-100) points (P < .01) (Figure 4). The mean FIM score significantly improved from 122 ± 1 (range, 121-125) points to 125 ± 1 (range, 124-126) points (P < .01) (Figure 5). No patient had wound dehiscence or infection that required reoperation.

The mean VAS score was significantly reduced from 80 (range, 68-92) preoperatively to 18 (range, 0-66) postoperatively (P < .01, Wilcoxon signed rank test).
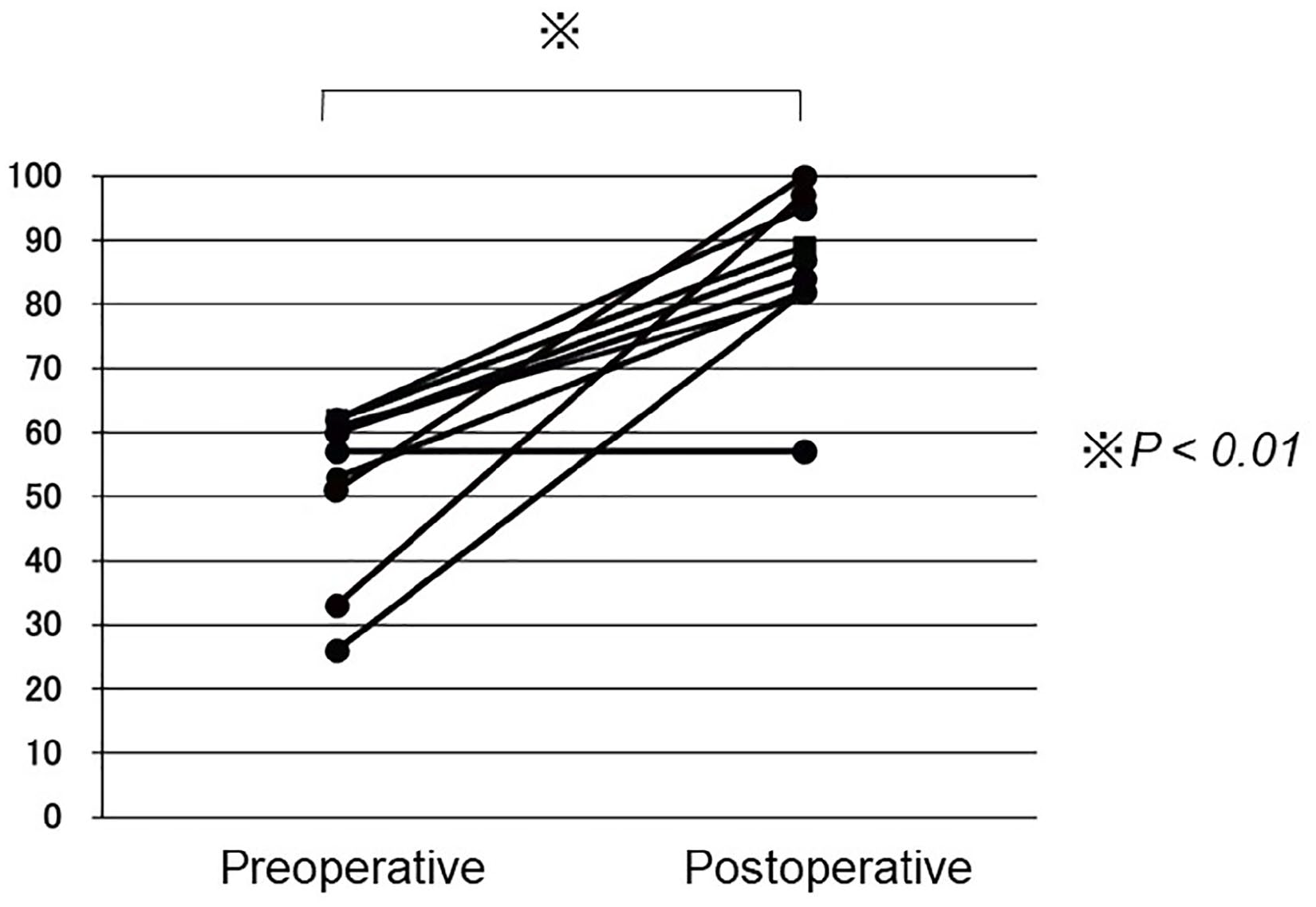
The mean JSSF ankle-hindfoot scale score significantly improved from 53 (range, 26-62) points to 89 (range, 81-100) points (P < .01).

The mean FIM score significantly improved from 122 (range, 121-125) points to 89 (range, 81-100) points (P < .01).
The postoperative SAFE-Q scores were 81 ± 10.3 points for pain, 78 ± 14.7 points for physical functioning, 90 ± 12.4 points for social functioning, 83 ± 15.4 points for shoe-related, and 86 ± 12.4 points for general health.
The mean range of motion of the ankle was significantly improved from 3.5 ± 6 (range, −10 to 10) degrees preoperatively to 11 ± 6 (range, 0-20) degrees postoperatively in dorsiflexion (P < .05), and from 22 ± 8 (range, 0-30) degrees preoperatively to 38 ± 4 (range, 30-40) degrees postoperatively in plantarflexion (P < .01) (Figure 6).

The mean range of motion of the ankle was significantly improved from 3.5 (range, −10 to 10) degrees preoperatively to 11 (range, 0-20) degrees postoperatively in dorsiflexion (P < .05), and from 22 (range, 0-30) degrees preoperatively to 38 (range, 30-40) degrees postoperatively in plantarflexion (P < .01).
In postoperative ADL, 9 patients were able to walk without a cane, and 1 patient required a cane. It was possible for 8 patients to get up from the chair without using the handrail, and for 2 patients using the handrail. Four patients were able to go up and down the stairs without using the handrail, and 6 patients needed to use the handrail. Before surgery, only 1 patient was able to go up and down the stairs without using the handrail, and 9 patients used a handrail.
Discussion
The talus is the third most common site of idiopathic osteonecrosis after the femoral head and femoral condyle. 18 The blood supply to the talus through the periosteum is limited because approximately 60% of the surface of the talus is covered with articular cartilage 17 and the talus has no muscular or tendinous attachments. 16 Osteonecrosis of the talus is caused by talus fracture13,30, heavy alcohol consumption, excessive steroid use 1 , hemophilia,10,15 and systemic lupus erythematosus. 8 At our hospital, all of our cases had idiopathic osteonecrosis.
Treatment of osteonecrosis of the talus poses challenges when considering operative options after nonsurgical treatment has failed. Conservative therapy can preserve ankle function and does not require hospitalization or surgery. However, a long nonweightbearing period is required, the results are unstable, and there are many cases that require surgery. 23 Hawkins reported of patients treated with nonweightbearing and had 1 excellent, 2 good, 12 fair, and 9 poor results. Only 7 of 24 (29%) had no pain at final follow-up. 9 Surgical treatments include hindfoot fusion, vascularized bone graft, and core decompression. 5 Hindfoot fusion such as Blair fusion and tibiocalcaneus fusion have been performed. Kitaoka et al 11 reported on 19 patients treated with hindfoot fusion and had 7 excellent, 6 good, 3 fair, and 3 poor results. Three of the 19 (16%) experienced nonunion. 11 Hindfoot fusion has good long-term results if bone fusion is achieved, but it has disadvantages such as high rate of nonunion, loss of ankle function, and leg-length discrepancies.12,14,31
Total talar replacement reduces pain, is not associated with leg-length discrepancy, and improves ankle function; however, it may result in long-term osteoarthritis of the ankle. 29 Talar body prosthesis was first introduced by Harnroongroj and Vanadurongwan 7 and was made from stainless steel. Harnroongroj and Harnroongroj 6 and Harnroongroj and Vanadurongwan 7 introduced a stainless-steel talar body prosthesis designed by slit scanography and reported a postoperative median score >75 points on the American Orthopaedic Foot & Ankle Society ankle-hindfoot scoring system. Takakura et al24,25 developed and introduced an alumina ceramic total talar prosthesis. Computed tomography of the healthy side of the talus is obtained to make a customized implant. 28 Taniguchi et al have reported that 55 ankles in 51 patients with talar osteonecrosis were treated with a total talar replacement, and the JSSF ankle-hindfoot scale score improved from 42.2 ± 17.4 points to 89.1 ± 8.6 points. Ankle inversion stress radiography showed a talar tilting angle of 5.0 ± 3.6 degrees and an anterior drawer distance of 1.4 ± 0.5 mm, with no ankle instability. Dislocation or migration of the implant was not observed. 27
In this study, scores of the VAS, JSSF ankle-hindfoot scale, and FIM and range of motion of the ankle improved significantly after surgery compared to before surgery. The postoperative QOL was evaluated using SAFE-Q, and the score was good, ranging from 78 points to 90 points. In ADL, 9 of the 10 patients were able to walk without a cane, and all patients did not require human assistance.
The limitations of this study are the small number of patients, a short follow-up period, and no control group. Therefore, additional follow-up is necessary to identify the clinical outcome of total talar replacement.
Conclusion
Total talar replacement is a useful treatment for patients with osteonecrosis of the talus. This replacement surgery does not cause shortening of the lower limbs but preserves the function of the ankle and subtalar joints and improves pain, ADL, and QOL.
Footnotes
Ethical Approval
This study was conducted with the approval of the Ethics Review Committee of Fukushima Medical University (approval no. 2022-008). Written informed consent was obtained from all patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.