
Abstract
Background:
Ankle arthrodesis (AA), or ankle fusion, is a surgical procedure used to treat severe ankle pathologies, particularly in patients with chronic pain and reduced mobility due to conditions like osteoarthritis, posttraumatic arthritis, and Charcot arthropathy. Diabetic patients undergoing AA often face higher risks of complications due to comorbidities such as dyslipidemia and hypertension. This study aims to compare the outcomes of AA in diabetic vs nondiabetic patients, using data from the Nationwide Inpatient Sample (NIS) from 2016 to 2019.
Methods:
Using the Nationwide Inpatient Sample database, 12 325 patients who underwent ankle arthrodesis were identified from 2016 to 2019 based on ICD-10 procedure codes. χ2 tests and t tests were used for univariate analysis, followed by multivariate logistic regression to assess complications between diabetic and nondiabetic patients. Temporal trends in surgical volume were analyzed using linear regression models, and risk ratios were calculated for perioperative complications during the index hospital stay.
Results:
Primary osteoarthritis was the most common cause, accounting for 55.4% of AA procedures. Multivariate logistic regression revealed that diabetes mellitus (DM) was significantly associated with increased risks of blood loss (odds ratio [OR] 1.59, 95% CI 1.23-2.05, P = .004), infection (OR 3.12, 95% CI 2.55-3.82, P < .001), heart failure (OR 1.35, 95% CI 1.06-1.73, P = .01), and acute kidney injury (OR 2.42, 95% CI 1.57-3.75, P = .001). No significant association was observed between DM and pneumonia (OR 2.27, 95% CI 1.645-4.605, P = .20).
Conclusion:
Diabetic patients undergoing AA have higher rates of comorbidities and postoperative complications, leading to longer hospital stays. These findings highlight the need for comprehensive preoperative and postoperative care to improve outcomes in this population.
Level of Evidence:
Level III, retrospective study.
Introduction
Ankle arthrodesis (AA), commonly known as ankle fusion, is a surgical procedure aimed at treating severe ankle pathologies by permanently joining the bones of the ankle joint. 1 With a growing population suffering from ankle arthritis, the incidence of ankle arthrosis is increasing, making it one of the most common problems for which patients seek treatment from foot and ankle orthopaedic surgeons.2,3 This condition often results in chronic pain, reduced mobility, and significant reduction in quality of life, necessitating effective surgical interventions such as AA to restore function and alleviate symptoms. 4 AA is typically indicated for cases of primary osteoarthritis, posttraumatic arthritis, severe deformities, and complications from previous surgeries, such as failed internal orthopaedic prosthetics (plates, screws, or implants). 5 Additionally, arthrodesis may be necessary for salvaging instability and addressing bone destruction caused by Charcot arthropathy. 6
Affecting roughly 25.8 million Americans, diabetes creates a unique subset of individuals undergoing ankle arthrodesis (AA) because of its complex effects. 7 Foot and ankle surgeons frequently encounter diabetic patients because of the high prevalence of related pathologies in this group, such as Charcot arthropathy, peripheral neuropathy, and diabetic foot ulcers. 8 Key causes and indications for AA in diabetic patients include diabetic neuropathy leading to Charcot arthropathy, primary osteoarthritis, and fractures resulting from decreased bone quality and poor wound healing.9,10 Diabetes has far-reaching effects on health, causing delayed wound healing, increased infection rates, and higher incidences of comorbidities such as dyslipidemia, hypertension, chronic kidney disease, and obesity, all of which complicate surgical outcomes. 11 A study of 1,000 patients revealed that those with complicated diabetes undergoing orthopedic foot and ankle surgery had a ten-fold greater risk of infection compared to non-diabetic patients and a six-fold greater risk compared to those with uncomplicated diabetes. 12 Infectious and noninfectious complications significantly impact patient satisfaction, increase the need for additional surgeries, and add to the economic burden. 8 Understanding the different outcomes of AA in diabetic vs nondiabetic patients is essential for improving surgical management and care.
Although AA remains a traditional surgical treatment of choice for patients where conservative treatments or joint-preserving options have failed, it is associated with several severe complications. 13 The most common complication is nonunion of the ankle joint, with diabetes and other factors identified as risk contributors in the previous literature. 14 Other frequent postoperative complications of ankle arthrodesis include malunion, infection, nonunion (previously referred to as aseptic loosening), malalignment, wound complications, and nerve injury.15- 17 In diabetic patients, the risk of postoperative complications is significantly higher.8,12,18 Additionally, a study using the Nationwide Inpatient Sample database from 2002 to 2011 evaluated the impact of diabetes mellitus on perioperative complications and hospitalization outcomes after AA and TAA. Their findings reported that diabetic patients undergoing AA tend to have longer hospital stays compared with nondiabetic patients. 19
Understanding the causes and complications of AA in diabetic vs nondiabetic patients is crucial. Although previous studies have highlighted the impact of diabetes on AA outcomes, our study aims to provide more up-to-date insights by using data from the Nationwide Inpatient Sample (NIS) from 2016 to 2019. This research will perform a comparative analysis of AA procedures in these 2 populations, examining epidemiology, etiology, patient characteristics, comorbidities, postoperative complications, and length of hospital stay. By providing a comprehensive understanding of the differential outcomes associated with AA in these patient groups, the findings aim to inform clinical practices and improve patient management strategies.
Methods
Data Source and Study Population
This retrospective analysis utilized data from the Nationwide Inpatient Sample (NIS), a large administrative database capturing inpatient stays in the United States. We included patients who underwent AA identified using specific International Classification of Diseases, Tenth Revision (ICD-10), procedure codes (provided in Table 1). The study period spanned from January 1, 2016, to December 31, 2019, which is the latest available data within the NIS system at the time of the study.
International Classification of Diseases, Tenth Revision (ICD-10), codes.
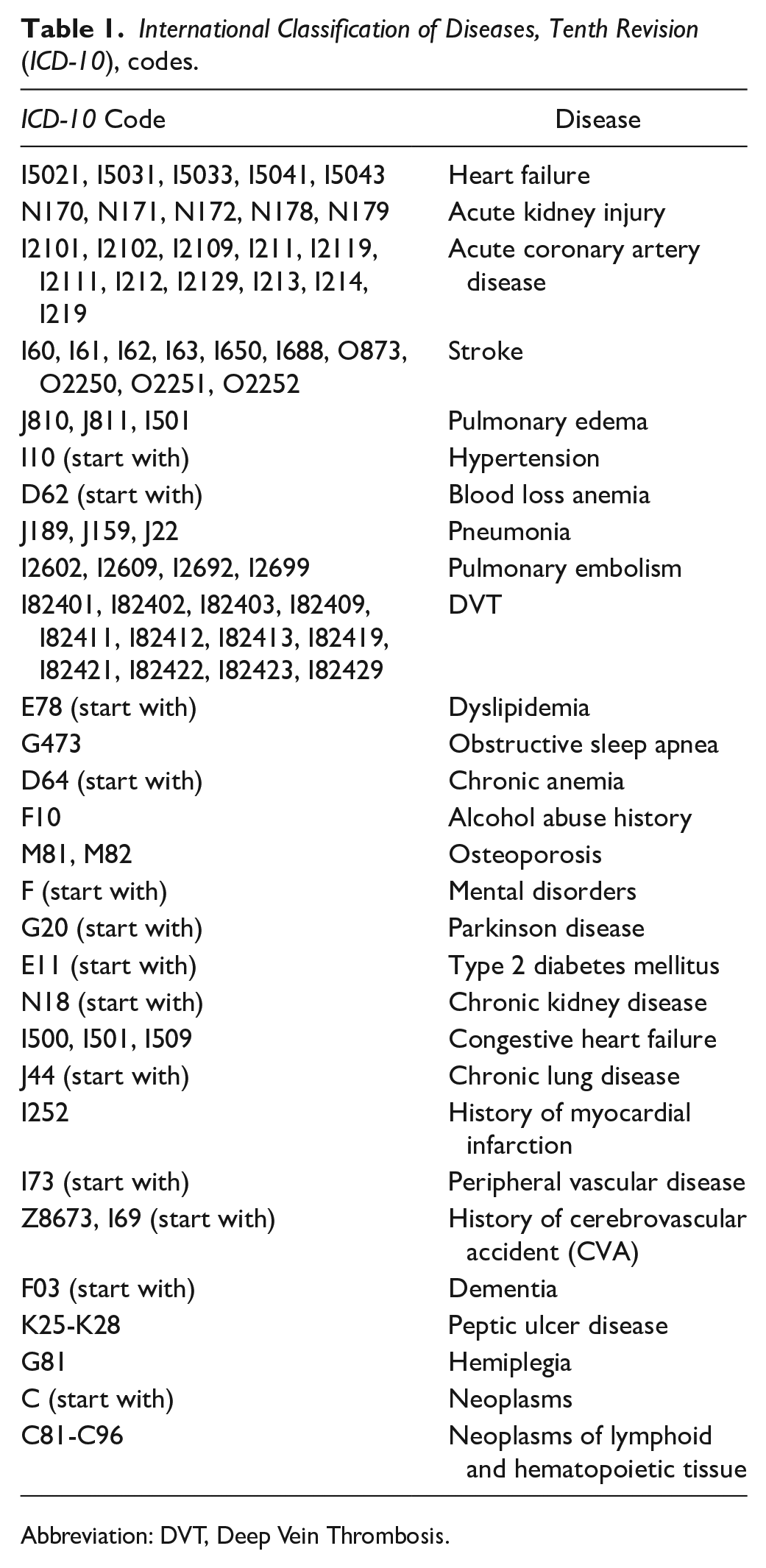
Abbreviation: DVT, Deep Vein Thrombosis.
Inclusion and Exclusion Criteria
We identified 12,325 patients undergoing ankle arthrodesis during the study period. The analysis was restricted to elective admissions, as ankle arthrodesis is predominantly an elective procedure for end-stage ankle pathology. Nonelective admissions were excluded to minimize confounding factors from emergency presentations and ensure a more homogeneous study population for analyzing diabetes-related outcomes.
Outcome Measures
We compared the following outcomes between diabetic and nondiabetic patients: trends in AA procedures over time, etiologic distribution, patient characteristics, comorbidities, postoperative complications, and length of hospital stay.
Statistical Analysis
Statistical analyses were conducted using SPSS 26. Univariate analyses included χ2 tests for categorical variables, independent samples t tests for continuous variables, and crosstab analysis. Risk ratios were calculated to determine the likelihood of postoperative complications in diabetic patients compared to nondiabetic patients. Complications assessed included heart failure, infection, acute kidney injury, blood transfusion, pneumonia, acute coronary artery disease, and blood loss anemia.
Variables showing significant associations in univariate analysis (P < .05) were subsequently included in multivariate logistic regression models. Separate regression models were constructed for each complication, adjusting for potential confounding variables including age, gender, and relevant comorbidities. Results are presented as odds ratios (ORs) with 95% CIs and corresponding P values.
Trend analysis was performed using linear regression models to assess changes in surgical volume over time for both diabetic and nondiabetic groups. The models included year as the independent variable and number of surgeries as the dependent variable. An interaction term between year and diabetes status was included to evaluate differences in trends between groups. Annual growth rates were calculated using the compound annual growth rate formula. Statistical significance was set at P <.05 for all analyses.
Results
Among the 12 325 patients who underwent AA, 4170 (33.8%) had diabetes mellitus and 8155 (66.2%) were nondiabetic. The analysis focused on trends over time, etiology, patient characteristics, comorbidities, complications, and hospitalization metrics, comparing diabetic and nondiabetic patients (Figure 1).
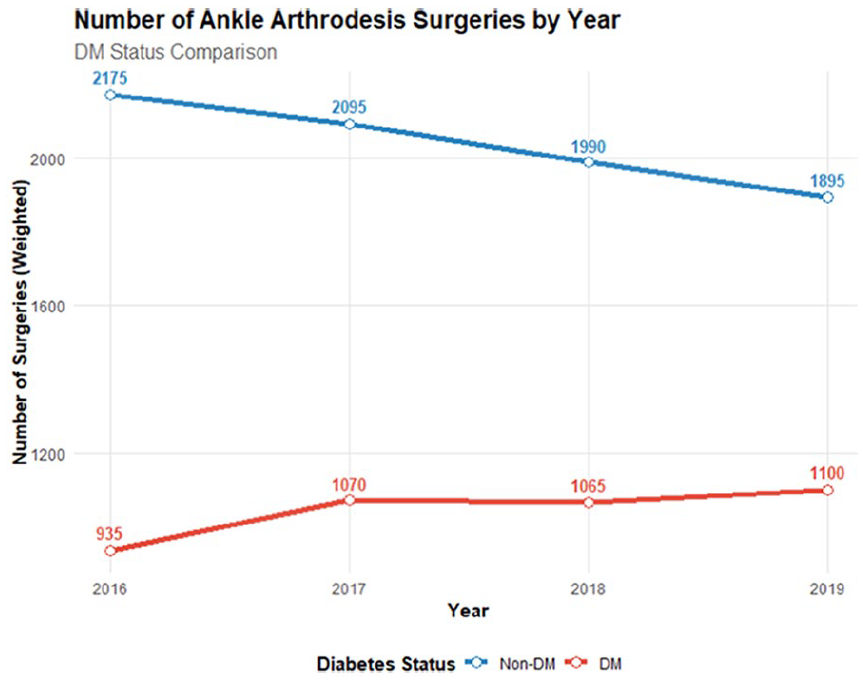
Number of Ankle Arthrodesis Surgeries among Diabetic and Non-Diabetic Patients by Year.
Trends in Ankle Arthrodesis Procedures
Trend analysis of ankle arthrodesis surgeries revealed divergent patterns between diabetic (DM) and nondiabetic (non-DM) patients over the study period. Nondiabetic patients showed a significant decreasing trend in surgical volume (P = .005), with a 12.9% decrease over 4 years (annual growth rate: –4.49%). In contrast, diabetic patients demonstrated an increasing trend (P = .13), with a 17.6% increase in surgeries (annual growth rate: 5.57%). The interaction model confirmed a significant difference in trends between the 2 groups (P = .009), indicating distinctly different temporal patterns in surgical utilization between diabetic and nondiabetic populations.
Etiologies for Ankle Arthrodesis in DM vs Non-DM Patients
The distribution of etiologies differed significantly between DM and non-DM patients (P <.001; Table 2).
Comparison of Underlying Etiologies for Ankle Arthrodesis Between Diabetic and Nondiabetic Patients. a
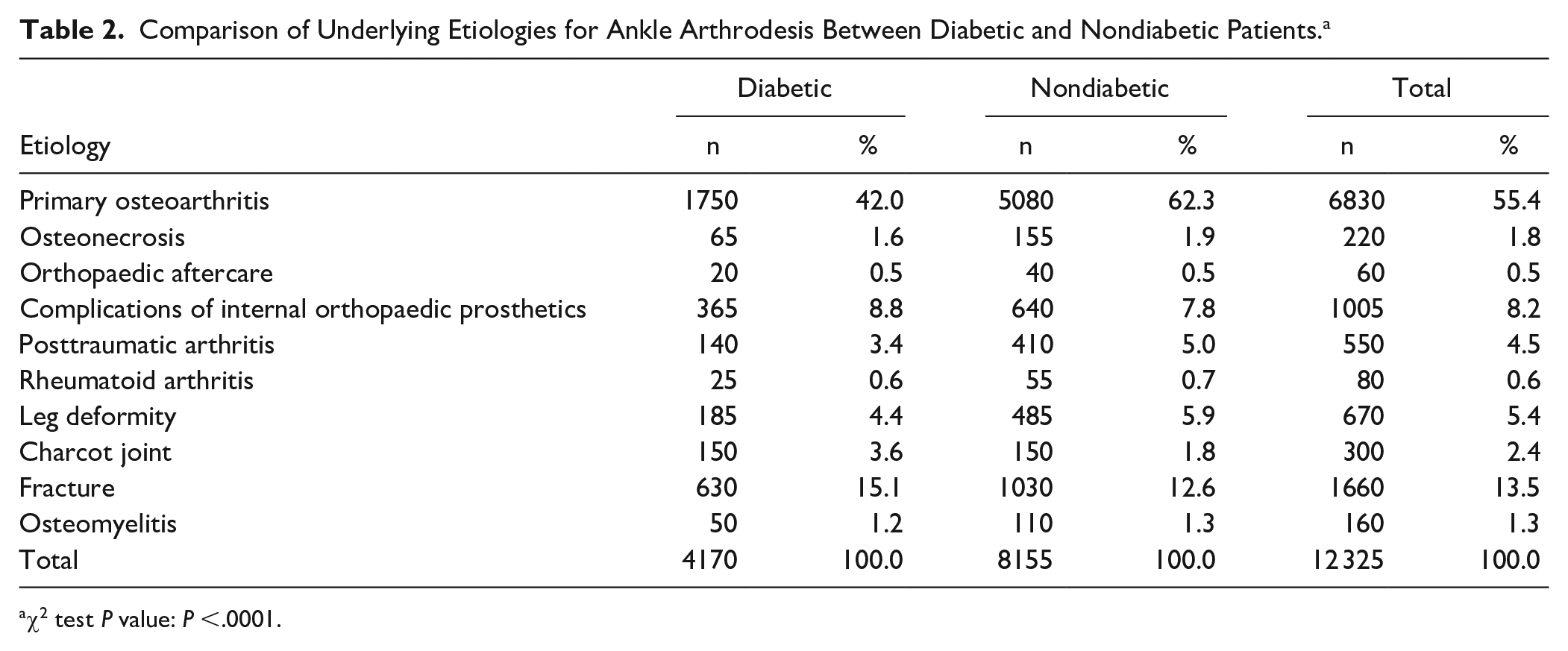
χ2 test P value: P <.0001.
Primary osteoarthritis remained the most common indication for ankle arthrodesis in DM patients (n = 1750, 42.0%), followed by diabetes-related conditions (n = 790, 18.9%) and fracture (n = 630, 15.1%). Other notable indications included complications of internal orthopaedic prosthetics (n = 365, 8.8%), Charcot joint (n = 150, 3.6%), and posttraumatic arthritis (n = 140, 3.4%).
In non-DM patients, primary osteoarthritis was markedly more prevalent (n = 5080, 62.3%), followed by fracture (n = 1030, 12.6%) and complications of internal orthopaedic prosthetics (n = 640, 7.8%). Posttraumatic arthritis and leg deformity were more common in non-DM patients (5.0% and 5.9%, respectively) compared with DM patients (3.4% and 4.4%, respectively).
Patient Characteristics and Hospitalization Data by Etiology
Statistical analyses comparing diabetic and nondiabetic patients across all etiologies were performed using the Mann-Whitney test, reflecting the study's approach to comparing these independent groups for age, and length of stay. (Table 3).
Clinical and Characteristics of Diabetic vs Nondiabetic Patients by Orthopaedic Etiology. a

Abbreviation: DM, diabetes mellitus.
Values are presented as mean ± SD.
P <.05, **P <.01, ***P <.001.
Age differences
Significant age differences between diabetic (DM) and nondiabetic (non-DM) patients were observed in several etiologies. Patients with primary osteoarthritis and diabetes were significantly older than their nondiabetic counterparts (62.7 ± 10.4 vs 58.6 ± 14.3 years, P < .001). Similarly, in posttraumatic arthritis, diabetic patients were substantially older (64.6 ± 11.8 vs 54.0 ± 13.9 years, P < .001). Patients with fractures and diabetes were also significantly older than nondiabetic patients (61.1 ± 11.0 vs 56.5 ± 15.5 years, P = .005). Other etiologies showed no significant age differences between diabetic and nondiabetic groups.
Length of stay
The length of hospital stay showed significant variations between diabetic and nondiabetic patients in several categories. Diabetic patients with primary osteoarthritis had longer hospital stays compared with nondiabetic patients (2.9 ± 2.1 vs 2.3 ± 1.8 days, P < .001). Similarly, patients with fractures and diabetes required longer hospitalizations (4.0 ± 3.4 vs 3.2 ± 3.2 days, P = .004). Posttraumatic arthritis patients with diabetes also showed longer stays (3.3 ± 2.8 vs 2.2 ± 1.0 days, P = .03). Notably, although not statistically significant, patients with complications of internal orthopaedic prosthetics and diabetes showed a trend toward longer stays (3.9 ± 3.3 vs 3.1 ± 2.6 days, P = .07).
Comorbidity Rates in Diabetic vs Nondiabetic Patients
The average age of diabetic patients is 61.6 years compared to 58.2 years for nondiabetic patients (P < .0001). Table 4 lists the rates of various comorbidities in diabetic vs nondiabetic patients. Diabetic patients had significantly higher rates of dyslipidemia (59% vs 27.7%, P < .0001), hypertension (52.8% vs 45.9%, P < .0001), and chronic kidney disease (29% vs 5.8%, P < .0001), among others. Venous thromboembolism rates are 0.2% for diabetic and nondiabetic patients (P = .51), and pulmonary edema rates are 0.1% for both groups (P = .28).
Comorbidity Rates in Diabetic vs Nondiabetic Patients. a
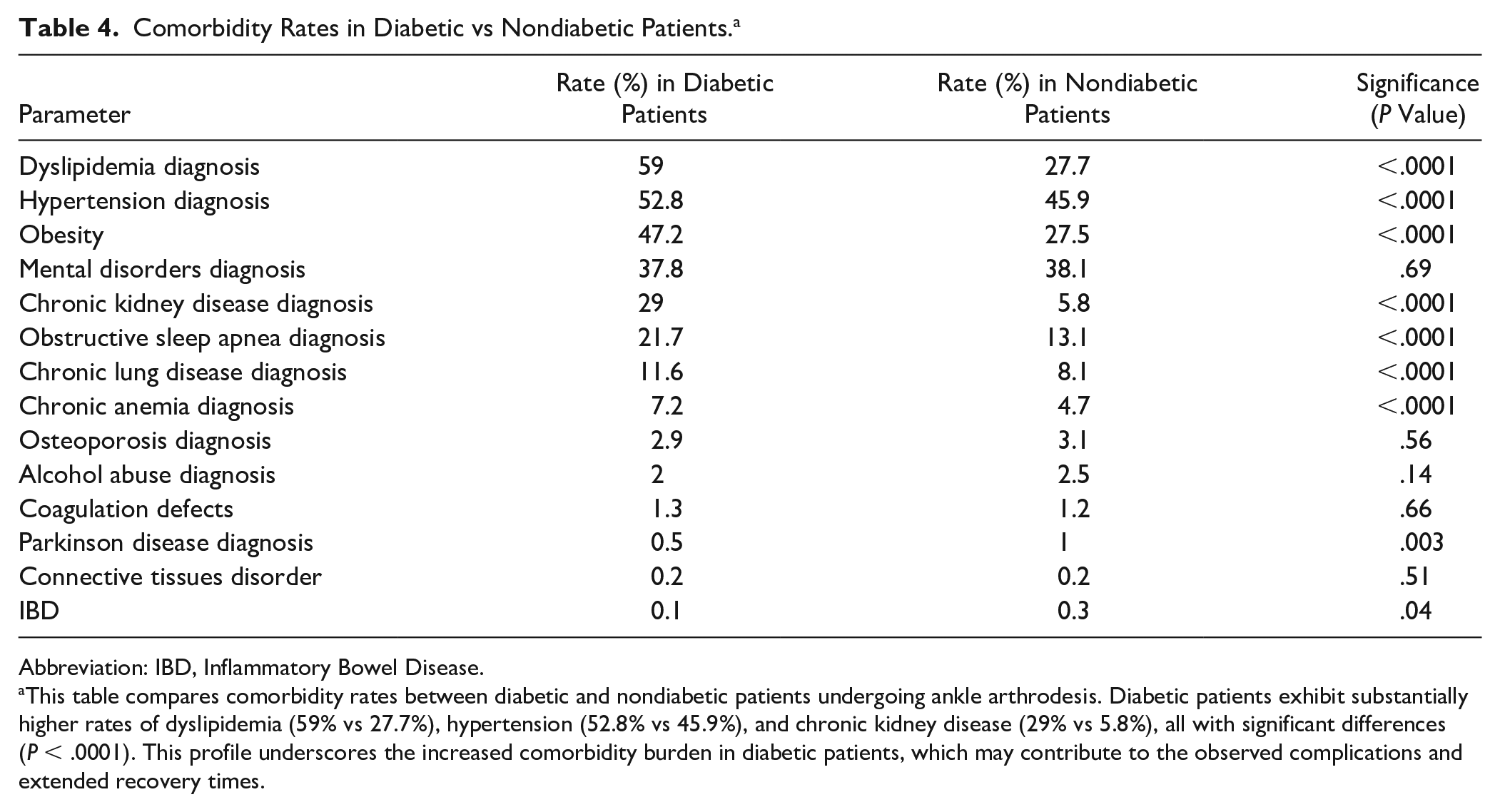
Abbreviation: IBD, Inflammatory Bowel Disease.
This table compares comorbidity rates between diabetic and nondiabetic patients undergoing ankle arthrodesis. Diabetic patients exhibit substantially higher rates of dyslipidemia (59% vs 27.7%), hypertension (52.8% vs 45.9%), and chronic kidney disease (29% vs 5.8%), all with significant differences (P < .0001). This profile underscores the increased comorbidity burden in diabetic patients, which may contribute to the observed complications and extended recovery times.
Risk Ratios for Postoperative Complications in Diabetic Patients
Univariate logistic regression revealed that Table 5 presents the risk ratios for several postoperative complications in diabetic patients compared with nondiabetic patients undergoing ankle arthrodesis. Heart failure and infection had the highest risk ratios. Heart failure had a risk ratio of 8.885 (95% CI 4.474-17.648, P < .0001), and infection had a risk ratio of 8.593 (95% CI: 4.895-15.083, P < .0001). Acute kidney injury had a risk ratio of 5.574 (95% CI: 4.572-6.797, P < .0001), blood transfusion had a risk ratio of 3.588 (95% CI: 2.831-4.546, P < .0001), and pneumonia had a risk ratio of 2.753 (95% CI: 1.645-4.605, P < .0001). Acute coronary artery disease had a risk ratio of 2.94 (95% CI: 1.32-6.551, P = .006), and blood loss anemia had a risk ratio of 1.978 (95% CI: 1.753-2.232, P < .0001).
Risk Ratios for Postoperative Complications in Diabetic vs Nondiabetic Patients.

Multivariate logistic regression analysis revealed several significant associations between comorbidities and postoperative complications. DM was significantly associated with multiple adverse outcomes, including increased risk of blood loss (OR 1.59, 95% CI 1.23-2.05, P = .004), infection (OR 3.12, 95% CI 2.55-3.82, P < .001), heart failure (OR 1.35, 95% CI 1.06-1.73, P = .01), and acute kidney injury (OR 2.42, 95% CI 1.57-3.75, P = .001). However, DM showed no significant association with pneumonia (OR 2.27, P = .20).
Hospitalization Metrics in Diabetic vs Nondiabetic Patients
Diabetic patients had significantly longer hospital stays compared to nondiabetic patients (3.6 days vs 2.6 days) with a difference reaching statistical significance (P < .0001).
Discussion
Analyzing data from the Nationwide Inpatient Sample (NIS) from 2016 to 2019, we compared AA procedures in diabetic vs nondiabetic patients, revealing several key differences. First, we noted divergent trends in AA procedures during the study period, with a significant decline in nondiabetic cases but an increase in diabetic cases. The decline in nondiabetic cases likely reflects advancements in joint-preserving treatments and a growing preference for TAA. 20 However, the increasing trend in diabetic patients suggests that AA remains an essential procedure for this population, particularly given their complex pathologies and potentially limited alternative treatment options. 21
Primary osteoarthritis emerged as the most common cause of AA, followed by fractures and complications from internal orthopaedic prosthetics. These findings are consistent with existing literature and underscore the need for AA in treating severe degenerative joint diseases and injuries.3 Diabetic patients undergoing AA were generally older and had significantly higher rates of comorbid conditions such as dyslipidemia, hypertension, chronic kidney disease, and obesity. Our results confirmed higher risk ratios for complications in diabetic patients, including infection, nonunion, heart failure, acute kidney injury, and the need for blood transfusions. These findings corroborate previous studies that reported a greater risk of infection in diabetic patients undergoing orthopaedic surgeries.1 Moreover, according to a comparison study based on the NIS database, diabetes is an independent risk factor for increased blood transfusion, increased risk for urinary tract infections, irrigation and debridement, and myocardial infarction. 22
According to our analysis, diabetic patients experienced longer hospital stays compared to the non-diabetic group. This finding aligns with a previous study using NIS data, which demonstrated that diabetic patients undergoing AA had a 0.4-day longer length of stay compared to those undergoing TAA. 19 By examining patient demographics, comorbidities, and a range of perioperative outcomes, we aimed to identify tailored management strategies to improve AA outcomes for diabetic patients. Enhanced preoperative optimization (eg, glycemic control and cardiovascular screening), close perioperative monitoring, and proactive postoperative care may mitigate complication risks in this population. For instance, targeted infection prevention protocols, optimized discharge planning, and specific care pathways could address the unique risks associated with AA in diabetic patients.
AA has benefits and drawbacks, which are important to consider when evaluating it against alternatives like total ankle arthroplasty. It is highly effective in reducing pain, increasing stability, and offering durability. On the other hand, it reduces the ankle's mobility and requires longer recovery times, including extended non-weightbearing periods. 23 TAA, in contrast, seeks to preserve joint mobility and has shown better functional outcomes in some studies, albeit with the potential for higher complication rates and revisions. Thus, the choice between AA and TAA should consider individual patient factors such as age, activity level, and specific health conditions, with AA remaining viable for patients needing pain relief and stability in cases of significant joint damage. 19
This study has several important limitations. Although the NIS database provides robust data on index hospitalizations, it does not capture outpatient surgical services or outpatient follow-up data, or postdischarge outcomes such as reoperations, limiting our understanding of long-term complications and treatment success. Additionally, our study could not account for variations in surgical techniques and perioperative care practices, which might influence outcomes. Lastly, our focus on elective admissions, while allowing for better control of perioperative variables, may introduce selection bias, as these patients likely represent a more optimized population with well-controlled comorbidities.
Despite its limitations, our study provides insights into the impact of DM on AA outcomes, highlighting significant differences in complication rates and hospital stay between diabetic and nondiabetic patients. Future studies should consider focusing on specific outcomes, such as reoperation rates, to assess whether DM directly influences the success and durability of AA. For example, examining the proportion of reoperations among diabetic vs nondiabetic patients could provide a clearer understanding of diabetes as a risk factor for surgical failure or recurrence.
To conclude, over the study period, AA procedures declined significantly in nondiabetic patients but increased in diabetic patients, indicating distinct utilization trends. Diabetic patients were older, had longer hospital stays, and exhibited a significantly higher burden of comorbidities, including dyslipidemia, hypertension, and chronic kidney disease. Complication rates were notably elevated in diabetic patients, with multivariate regression demonstrating increased risks of infection, acute kidney injury, heart failure, and blood loss. These findings underscore the need for enhanced perioperative management strategies to mitigate risks and improve outcomes for diabetic patients undergoing AA.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251315122 – Supplemental material for Ankle Arthrodesis: Epidemiology, Etiology, and Complications in Diabetic vs Nondiabetic Patients Using US Nationwide Inpatient Sample Data
Supplemental material, sj-pdf-1-fao-10.1177_24730114251315122 for Ankle Arthrodesis: Epidemiology, Etiology, and Complications in Diabetic vs Nondiabetic Patients Using US Nationwide Inpatient Sample Data by Assil Mahamid, MD, David Maman, MD, Summer Sofer, Mykhail Pavlenko, MD, Amr Mansour, MD, Marah Hodruj, MD, Yaron Berkovich, MD and Eyal Behrbalk, MD in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
The study was conducted under exempt status granted by the institutional review board, and the requirement for informed consent was waived because of the deidentified nature of the NIS data set.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.