
Abstract
Neuropathic arthropathy (NA) is a progressive degenerative and destructive joint disease associated with underlying chronic neurologic deficit. A 34-year-old woman was referred to our tumor clinic with swelling and destruction of her left elbow joint. Except for a 5-year history of multiple sclerosis (MS), she had no other underlying diseases. Suspected of tumor involvement, she had been undergone an open biopsy. The pathologic report was fibromatosis, which was not compatible with imaging studies and clinical presentations. Second surgical inspection and cellular study didn’t prove tumoral involvement. Magnetic resonance images (MRIs) showed multiple hyper signal plaques in her cervical spine. MRI findings, clinical features, surgical observations, and disproportionate painless elbow destruction all confirmed the MS NA diagnosis.
Introduction
Neuropathic arthropathy (NA) or Charcot joint is considered as a progressive degenerative arthropathy associated with a chronic neurologic disorder. Charcot joint usually presents with a swollen and erythematous joint. Any condition resulting in long-lasting decreased peripheral nerve sensation, proprioception, or fine motor control can cause Charcot joint disease. NA accompanies different underlying diseases such as syringomyelia, leprosy, diabetes mellitus, end-stage renal disease, Tabes dorsalis, gigantism, chronic alcoholism, intra-articular steroid injections, congenital insensitivity to pain, meningomyelocele, multiple sclerosis (MS), myelodysplasia, Chiari malformation, and any type of peripheral neuropathy. 1,2
Usually, joint symptoms happen earlier than neurologic symptoms. 3 Some authors described three phases of Charcot joint: first is the destructive phase, where the joint is hyperemic and swollen so that there is osteoclastic bone resorption associated with repetitive trauma. Second is the reparative phase, where there is a formation of dense fibrous tissue and coalescence of the debris, and finally, the quiescent phase, where there is a decreased vascularity and osseous sclerosis. 4
Elbow Charcot joint is a rare diagnosis. Patients may experience painful or painless joints, joint instability, swelling, and dysfunction. History of trauma is not routinely reported, and most patients with a neuropathic elbow present elbow instability and/or subluxation. 5 –7 Physical examination usually reveals joint laxity, crepitus, effusion, and decreased muscle strength. 1 Hypertrophic changes such as severe joint destruction, osteophytes, fractures, osseous debris, and new bone formation are found more in the elbow. 6
Case presentation
A 34-year-old woman with MS that was diagnosed 5 years ago was referred to our tumor clinic with diffuse swelling of her left elbow and proximal of forearm. She had mild pain and weakness in the elbow. The patient had been undergone a surgical procedure to take a biopsy in another clinic. The pathologic report was fibromatosis. Blood serum analysis including cell count, fasting blood sugar, and thyroid function tests was in normal range. Venereal disease research laboratory (VDRL) blood test was nonreactive. Biochemical analysis, tumor markers, rheumatoid factor, erythrocyte sedimentation rate, and C-reactive protein all were in normal values. Plain radiography showed a mild diffuse joint destruction and new bone formation and sclerosis, indicating chronic inflammatory process like a chronic infection (Figure 1). Also, tumor involvement was in our differential diagnosis list. Magnetic resonance images (MRIs) of elbow showed diffuse inflammatory involvement without a typical neoplastic lesion (Figure 2).
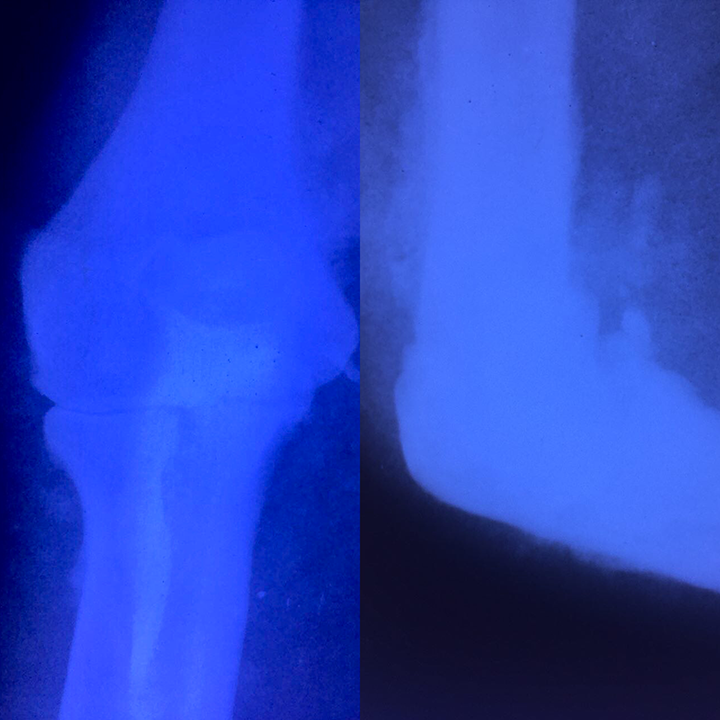
The first plain radiography of the patient’s elbow showed joint degeneration, sclerosis and new bone formation.
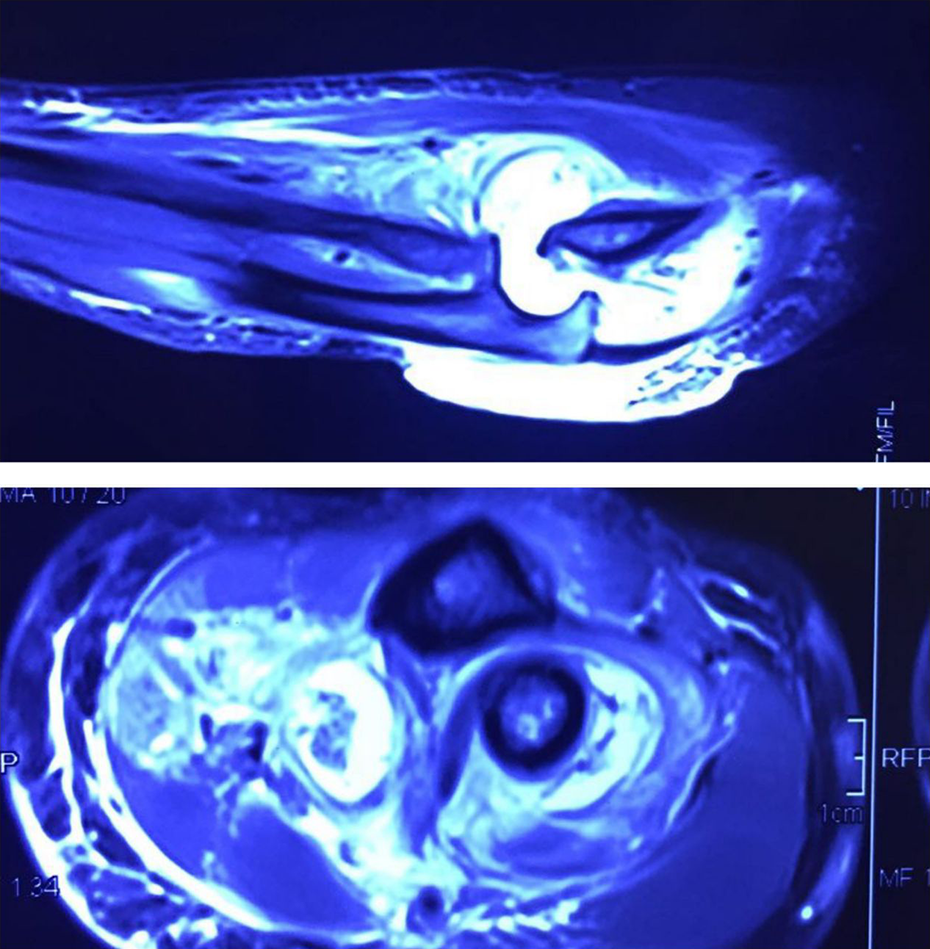
Suppression of fat signal in MRI of the elbow illustrated excessive liquid accumulation within the intra-articular space and pre-articular structures.
Sonography showed soft tissue inflammation and joint effusion with normal venous flow. Whole body bone scan was done to roll out concurrent lesions. It was a single focal lesion with a hypervascular pattern, involving bony structures of the left elbow. The first electromyogram and nerve conduction velocity (NCV) study were normal. In the second NCV, left ulnar nerve entrapment in elbow level was reported. In her second surgery, we opened the elbow and saw diffuse articular surface destruction with ligaments rupture and joint instability, without finding neoplastic tissue or infectious pus. After extracting enough tissue for pathologic evaluation, we repaired the ruptured elbow capsule and repaired the collateral ligaments. We entered the K-wire from the capitulum to radial head to support our soft tissue repair, and finally we released the ulnar nerve.
Second pathologic report was nonspecific papillary synovitis and destructive arthritis.
Considering the results of second biopsy and the surgical observations, we were highly suspicious about two differential diagnosis: 1—unusual infection like Mycobacterium tuberculosis and 2—Charcot arthropathy. Caseous necrosis had not been detected and the tuberculosis (TB) culture was negative, so TB infection was rolled out. Three weeks after surgery, the patient came back with elbow dislocation and bended wire, but she had disproportionate mild pain. We removed the wire surgically and put an external elbow brace. After 4 weeks, she came back with a painless burn in the left elbow due to contact with steam. So, the chance of Charcot joint diagnosis intensified. Then, we evaluated her cervical spine with MRI to find a spinal cord disease like syringomyelia. Surprisingly, the cervical MRI showed multiple hyper signal plaques indicating cord involvement by MS (Figure 4). After that, we have preferred to observe her elbow without any more surgical intervention. Now, after 1 year, she had painless dislocated elbow with a full range of motion in both flexion and extension, either in supination and pronation (Figure 3).
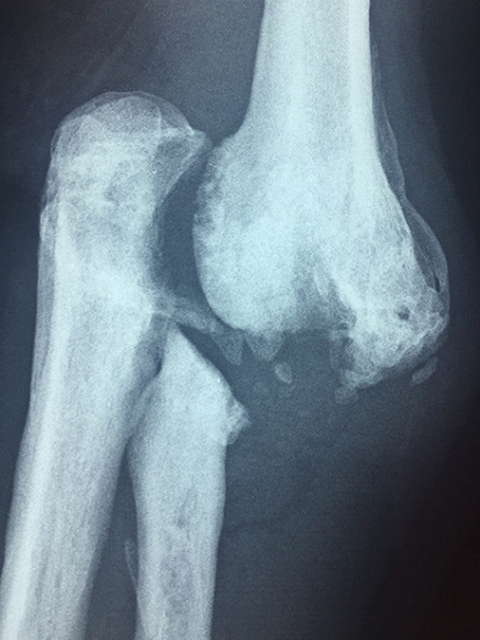
Destruction and complete dislocation of the elbow 1 year after the diagnosis.
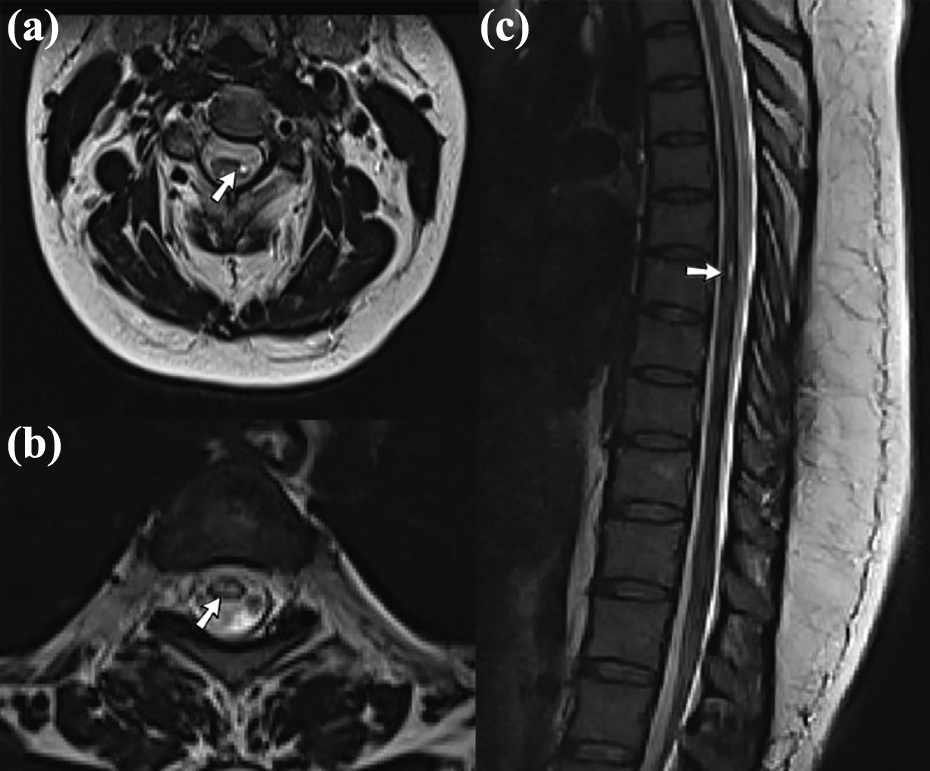
Axial T2W images of cervical (a) and thoracic (b) spine show hypersignal plaques in the cord (arrows in (a) and (b)). Sagittal T2W image depicts a short-segment hypersignal plaque located in the thoracic cord (arrow in (c)).
Discussion
MS is a rare cause for Charcot joint. The most prevalent features of MS in the musculoskeletal system are muscle weakness and joint contracture. Elbow involvement was very rare in MS. Of 156 MS patients investigated in Australia, less than 5% had elbow involvement. 8
In a study conducted by Eichenholtz, there was only three neuropathic elbows in a series of 94 joints. 9 Syringomyelia and Tabes dorsalis are the most common causes of NA of the elbow. 2,10 –12
Not only the elbow is a rare location for Charcot joint, but also MS is an extra ordinary cause for Charcot joint. Therefore, this patient was a rare case in scientific literature.
In a patient with NA of elbow or shoulder, cervical MRI should be done to roll out cervical spine pathology. 13 In our patient, the Charcot joint was an exclusive diagnosis. We did the cervical MRI when surgical evaluations failed to find the etiology, and then we found cervical cord MS plaques. Although spinal cord atrophy is a common finding in MS, 14 association between MS spinal cord involvement and Charcot joint has not been reported in the literature.
There was a misleading open biopsy and pathologic report before she was referred to our clinic. Fibromatosis was not compatible with her clinical signs and her elbow MRIs. So, this deceptive diagnosis conducted us to the second surgery in which we couldn’t find neoplastic tissue. Findings such as destructive features of the elbow joint, destruction of the chondral surface of humerus in the elbow, subluxation, and collateral ligament failure led us to Charcot joint diagnosis.
In the neuropathic elbow, most suggested protocol is mobilization, physical therapy, and functional bracing. 7,15
Indications for neuropathic elbow surgery include persistent pain and the inability for activities of daily living, 15 which our patient had none of them. The results of surgical intervention are often unpredictable with high rates of complications. 16 Vaishya performed a successful elbow arthrodesis in a patient with paraplegia and a traumatic syrinx which causes elbow neuroarthropathy. 17
In elbow Charcot joint, prosthesis arthroplasty is considered a contraindication because of protective sensation deficit, lack of normal reflexes, osteopenic bone, and ligament weakness. 15 Kwon and Morrey have obtained good results in resection arthroplasty of the elbow in three patients with elbow instability.
Our patient has functional dislocated elbow. She has no pain, surprisingly full range of motion both in flexion–extension and in forearm rotation. She has just minor limitation for heavy daily activities, but she was not seeking treatment for this problem. So, we decided to carry out physical therapy and external dynamic bracing.
In neuropathic elbow, ulnar and posterior interosseous nerve compression can develop till the elbow level. 16 Aly et al. reported a patient with bilateral Charcot elbow and ulnar neuropathy who underwent successful bilateral ulnar nerve decompressions. 18 Our patient underwent NCV evaluation for two times. The only NCV finding was left ulnar nerve entrapment about elbow level, which diminished after the second surgery due to ulnar nerve release. No definite electrodiagnostic signs of peripheral poly neuropathy or root involvement were found.
Advanced NA is characterized by the 5Ds: Debris, increased Density (sclerosis), Destruction, Disorganization, and Dislocation 19 and our patient got them all during her illness progression.
Conclusion
Charcot joint due to cervical spine MS plaques is a very rare presentation, but we should keep that in our differential diagnosis list.
Although biopsy is a reliable method to determine tumor lesions, compatibility between pathologic findings and imaging studies is necessary to make a precise diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.