
Abstract
Background:
Interphalangeal coalition is characterized by fusion of interphalangeal joint between the middle and distal phalanges. Interphalangeal coalition fractures often result in delayed union or nonunion. The purpose of this study was to evaluate the results of focused extracorporeal shock wave therapy (ESWT) for painful delayed union or nonunion of fractures of the interphalangeal coalition.
Methods:
The study group consisted of 9 patients (9 feet) diagnosed with painful delayed union or nonunion due to persistent pain and no tendency toward bony union for at least 3 months after the interphalangeal coalition fracture on plain radiographs between 2021 and 2023 were included. The mean age was 51.3 years (23-64). Focused ESWT was performed in all patients. The mean time from the date of injury to the start of ESWT was 16.1 weeks (12-15). ESWT was performed every 2 weeks, with each session consisting of 3000 impulses (0.15-0.25 mJ/mm2). Plain radiographs were used to confirm bone union, and visual analog scale (VAS) scores were used for pain assessment.
Results:
Complete bony union was documented in all 9 patients. The application of focused ESWT was performed a mean of 2.7 times (2-4), and the mean duration from the initiation of treatment to the confirmation of bony union was 7.4 weeks (3.6-12.7). In all cases, the symptoms of swelling and pain were alleviated. The VAS scores exhibited significant improvement, with the mean VAS score decreasing from 3.8 (2-6) before ESWT to 0 after the achievement of union (P < .001).
Conclusion:
In this small cohort, all patients with painful delayed union or nonunion of fractures at the interphalangeal coalitions achieved complete bony fusion after focused ESWT. Moreover, bony union was observed within 2 months of ESWT initiation. These findings suggest that focused ESWT may be a valuable treatment option for painful delayed union or nonunion of interphalangeal coalition fractures.
Level of Evidence:
Level IV, case series.
Introduction
Interphalangeal coalition is characterized by fusion of the interphalangeal joint between the middle and distal phalanges, and it is seen in all lesser toes, with the fifth toe being the most common. 5 The incidence of interphalangeal coalition of the fifth toe has been reported as 37% to 44% in populations of European descent6,9,10 and in 73% of populations of Japanese descent. 11 Interphalangeal coalitions in other toes are less frequent, as 11.9% in the fourth toe and 0.8% in the third toe in Japanese. 11 It has been reported that fractures of interphalangeal coalition often result in delayed union or nonunion, although the clear reason is unknown. 13 Although a few case reports have been published on the treatment of painful delayed union or nonunion with long-term conservative treatment or surgical treatment, there are no coherent case series and no clear evidence of treatment has been established.2,13
Extracorporeal shock wave therapy (ESWT) is a well-known treatment for kidney stone fragmentation; however, over the past few decades, ESWT has been increasingly applied for bone growth stimulation. In 1991, Valchanou and Michailov 15 used ESWT for the management of delayed and nonunion fractures of both the upper and lower limbs. They reported achieving bony union in 70 of 82 fractures without complications. In recent years, numerous investigations have been conducted with respect to the potential of ESWT as a treatment for delayed union and nonunion fractures. The results of these studies suggest that ESWT has the potential to be an effective therapy for these conditions.8,18 Low-intensity pulsed ultrasound stimulation (LIPUS) has also been used to treat nonunions, but recent studies reported that ESWT modulates distinct signaling pathways of the fracture healing process better than LIPUS. 3 Surgery for nonunion of the interphalangeal coalition is technically challenging because of the small size of the bone, although its nonunion is difficult to treat without surgery. Therefore, if ESWT can achieve bone union and avoid surgery, ESWT could be a useful treatment option. However, there is currently a lack of literature on the efficacy of ESWT for painful delayed union or nonunion of interphalangeal coalition fractures.
This study aimed to evaluate the results of focused ESWT in patients with painful delayed union or nonunion of fractures of the interphalangeal coalition.
Material and Methods
Patients
This cohort study was approved by the Institutional Review Board of the hospital. Patients treated with ESWT between 2021 and 2023 for delayed union or nonunion of interphalangeal coalition fractures were eligible for inclusion in this study. The inclusion criteria for this study were as follows: (1) no signs of any callus formation on plain radiographs taken at least 3 months after the fracture, and (2) persistent pain. The presence of these 2 conditions was indicative of a painful delayed union. We did not include any cases in our study that demonstrated even a slight amount of callus formation 3 months after the injury.
Treatment Protocol
Focused ESWT was applied to the nonunion site using the DUOLITH SD-1 T-TOP Ultra (Storz Medical AG, Tägerwilen, Switzerland). We performed ESWT every 2 weeks, with each session consisting of 3000 impulses. The energy flux density was set at 0.15 to 0.25 mJ/mm2, depending on the patient’s pain tolerance limit.
Outcome Analysis
ESWT was performed at least twice in all patients and evaluated using plain radiographs approximately 1 month after treatment initiation. If any signs of callus formation were observed at this point, ESWT was normally terminated, but continued if the patient wished to continue. ESWT was continued until callus formation was finally observed on plain radiographs. In this study, plain radiographs were used to confirm bone fusion, and visual analog scale (VAS; maximum of 10) scores were used for pain assessment.
Statistical Analysis
Descriptive statistics are presented as means and standard deviations for continuous variables. A paired t test was performed to compare the pre- and post-ESWT VAS scores. Differences were considered statistically significant at P < .05. All statistical analyses were performed using SAS Software, version 9.3 (SAS Institute Inc, Cary, NC, USA).
Results
Patient Demographics
In total, 9 patients (9 toes) diagnosed with painful delayed union or nonunion due to persistent pain and no tendency toward bony fusion at least 3 months after fracture of the interphalangeal coalition were identified, all of whom were treated with ESWT. All patients were included in this study, including 2 male and 7 female patients. None of the patients were lost to follow-up. The fourth toe was present in 3 cases, and the fifth toe in 6 cases. Previous treatments included taping in 7 cases and no taping, splint, or brace in 2 cases. The mean patient age was 51.3 ± 12.2 years (range, 23-64). The mean time from the date of injury to the start of ESWT was 16.1 ± 4.1 weeks (range, 12-25 weeks). There were no patients with significant comorbidities such as diabetes or smokers.
Complete bony union was documented in all 9 patients. The application of focused ESWT was carried out a mean of 2.7 ± 0.8 times (range, 2-4 times), and the mean duration from the initiation of treatment to the confirmation of bony union was 7.4 ± 2.6 weeks (range, 3.6-12.7 weeks). In all cases, the symptoms of swelling and pain were successfully alleviated. The VAS scores exhibited significant improvement, with the mean VAS score decreasing from 3.8 ± 1.4 (range, 2-6) before ESWT to 0 after the achievement of union (P < .001). In particular, even 2 weeks after the first ESWT, all patients showed improvement in pain, with a mean VAS of 2.4 ± 0.8 (range, 1-4), which was significantly better than before the start of ESWT (P = .019). No complications were observed in this cohort. Cases are presented in Figures 1 to 3.
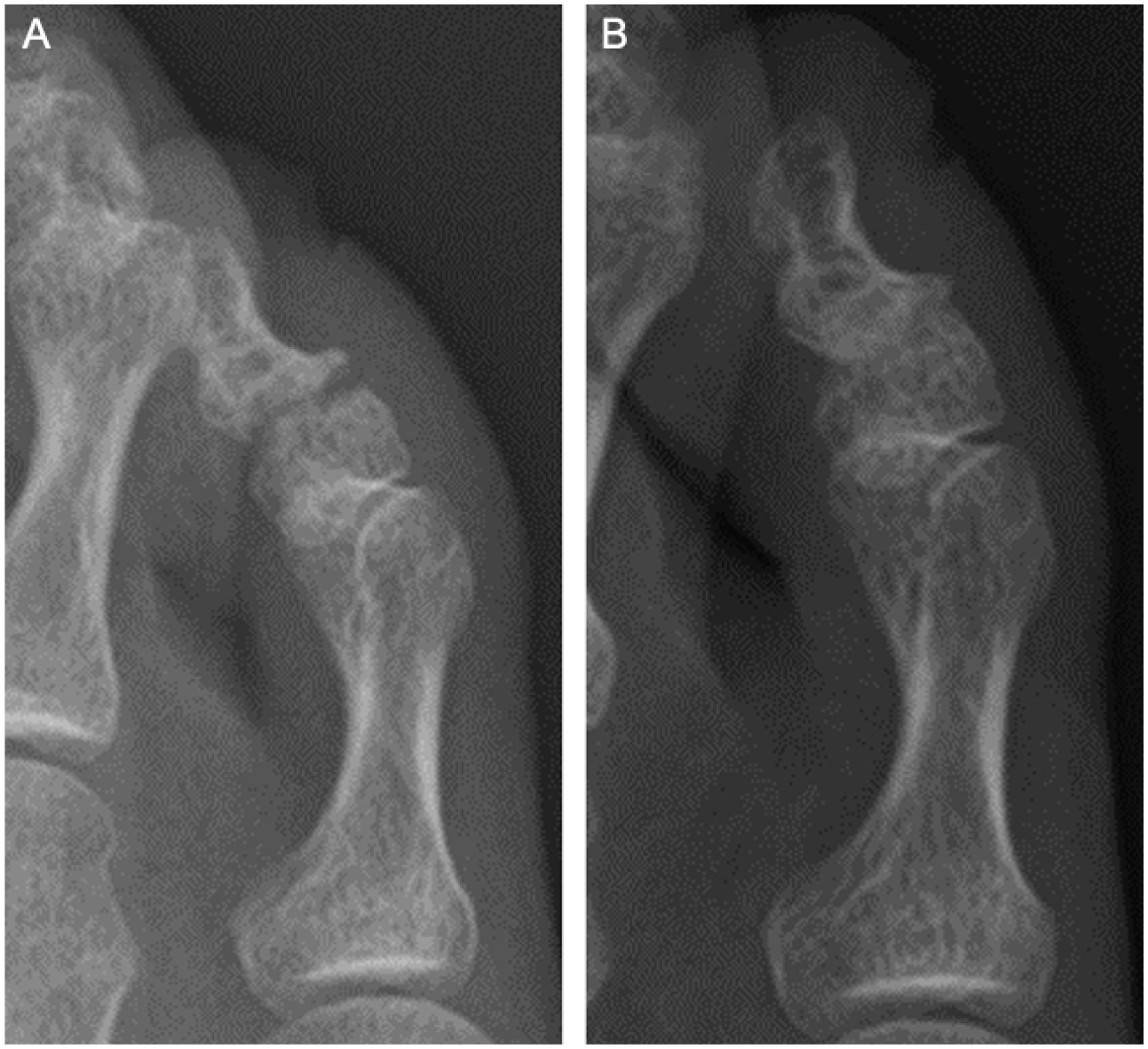
Sixty-four-year-old woman. (A) Nonunion on radiograph 3 months after the injury. (B) Bone union on radiograph 1 week after 3 ESWT sessions (7 weeks after ESWT initiation). ESWT, extracorporeal shock wave therapy.

Fifty-eight-year-old woman. (A) Nonunion on radiograph 3 months after the injury. (B) Radiograph 1 week after 2 ESWT sessions (5 weeks after ESWT started) showed bony bridging and improvement in pain. (C) Bone union was seen on radiograph 1 week after 4 ESWT sessions (7 weeks after the start of ESWT), and pain disappeared. ESWT, extracorporeal shock wave therapy.

Forty-four-year-old woman. (A) Nonunion on radiograph 3.5 months after injury; (B) Bone union on radiograph 1 week after 2 ESWT sessions (5 weeks after ESWT started). ESWT, extracorporeal shock wave therapy.
Discussion
The most important finding of this study was that all 9 cases of painful delayed union or nonunion achieved complete bony fusion following focused ESWT. Moreover, bony union was observed within 2 months of ESWT initiation in most patients. The current study suggests that focused ESWT is a valuable treatment option for achieving bony fusion in cases of painful delayed union or nonunion of fractures at the interphalangeal coalitions.
Most toe fractures are caused by direct external forces and are often observed in the most lateral fifth toe. A fracture occurring at an interphalangeal coalition of the middle and distal phalanges may be the result of a stiffened toe with fewer motion segments and a decreased ability to absorb the energy of trauma. 13 Coalition sometimes exhibits fissures that partially divide the bone into proximal and distal parts. This notch may act as a stress riser, predisposing it to fracture. Finally, the fused phalanx is usually longer than a separate distal or middle phalanx, resulting in a longer lever arm, which may make it more susceptible to fractures. Rozen et al reported a case in which this fracture was mistaken for a 3-phalangeal fracture by another physician, 12 but the high frequency of phalangeal fusion in the fifth toe is not always well recognized, and many of these fractures may have been missed. The radiographic appearance of a fracture through a toe coalition can be mistaken for a normal joint, particularly if the toe is flexed, and a true anteroposterior view of the toe is not obtained. A radiograph of the opposite foot is helpful because up to 94% of fifth toe coalitions are bilateral. 14
It is not clear why the fracture of the interphalangeal coalition results in delayed bone healing. This may be due to the fact that this fracture site is difficult to immobilize and most patients also apply weightbearing quickly. In addition, because the fusion is an inherently articulated area, the extrinsic and intrinsic muscles of the toe work to move the joint in the same way as the nonfused toe, and fractures at the coalition are likely to be unstable. 13 In normal phalangeal fractures, bone fusion is expected to be achieved within 2-3 months, with appropriate immobilization. In the case of fracture of the interphalangeal coalition, there have been reports of bone fusion taking 3-6 months.7,13 Yamaji et al 19 reported a case in which bone union took 15 months. It may also be asymptomatic, even if it is a nonunion. However, surgical treatment is considered if painful nonunion occurs. Foo and Wee 4 reported a case of a fourth toe fracture that was still a nonunion at 5 months after the initial injury, which was consequently treated with screw fixation. It is not known if, over time, bone fusion would occur without surgery, and how long it would take. There have been no comprehensive case series for either surgical or conservative treatment of painful nonunion of fractures at interphalangeal coalitions.
In an effort to achieve bony union more rapidly and noninvasively, over the last decade, ESWT has emerged as a promising alternative to surgery. Focused ESWT on bone promotes the production of substances such as transforming growth factor-β1, endothelial nitric oxide synthase, and vascular endothelial-derived growth factor, which in turn stimulates angiogenesis and bone formation.16,17 It has been reported that focused ESWT is effective in promoting the healing of delayed union fractures.1,8 In a systematic review, Willems et al reported that ESWT is as effective as surgery for the treatment of delayed unions and nonunions with less severe complications. 18 To our knowledge, there are no reports of treatment with ESWT for delayed union or nonunion of fractures at interphalangeal coalitions. In this study, painful delayed union or nonunion due to persistent pain and no tendency toward bony fusion at least 3 months after fracture were included, and ESWT was started at a mean of 16.1 weeks (12-25 weeks). Bone union was observed in all cases. Furthermore, most patients achieved bone union within 2 months of the start of treatment (a mean of 7.4 weeks in this study), with the earliest being 1 month. With bone union, pain and swelling disappeared in all patients. However, there is still a possibility that bone union could have been achieved in either case if the patient had waited longer. The lack of a control group is undoubtedly a major limitation. On the other hand, the present study included only those cases in which no callus formation was seen at the start of ESWT, and if a solid complete bone fusion can be achieved around 1-2 months after the start of ESWT, it could be considered as a treatment option. Although the number of cases is small (9), it should be noted that bone union was achieved in all cases. In addition, in all cases, even a single ESWT showed a reduction in pain, possibly due in large part to the pain-relieving effect of ESWT; however, it is also possible that the process of bone fusion was initiated even after only 1 ESWT. Therefore, after firm consultation with the patient, ESWT can be considered for painful delayed union cases of fractures at the interphalangeal coalitions.
Our study has several important limitations. First, this was a retrospective analysis. Second, the small number of patients involved in the study may not appropriately represent the true results from treating nonunion of fracture of the interphalangeal coalition with ESWT and may limit the ability to generalize our results to all patients. Another limitation is that there was no control group and this was not a comparative study. In addition, as mentioned above, there may have been cases in which bone union could have been achieved if treatment had been continued without ESWT. However, we believe that ESWT is likely an effective adjunctive treatment because bone union is achieved within 1-2 months after the start of ESWT.
Conclusion
Fractures occurring at interphalangeal coalitions have been reported to require a considerable amount of time for bony union, and surgical intervention has been reported in cases of painful delayed union or nonunion. However, in our small cohort study, all 9 cases of painful delayed union or nonunion achieved complete bony fusion after focused ESWT. Moreover, bony union was observed within 2 months of ESWT initiation in most patients. These findings may suggest that focused ESWT is a valid treatment option for achieving bony union in cases of painful delayed union or nonunion of fractures at the interphalangeal coalitions.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241268307 – Supplemental material for Focused Extracorporeal Shock Wave Therapy for Painful Delayed Union or Nonunion of Fractures of Interphalangeal Coalition
Supplemental material, sj-pdf-1-fao-10.1177_24730114241268307 for Focused Extracorporeal Shock Wave Therapy for Painful Delayed Union or Nonunion of Fractures of Interphalangeal Coalition by Yoshiharu Shimozono, Daisuke Mori, Yasuyuki Mizuno, Noboru Funakoshi, Masahiko Kobayashi, Shuichi Matsuda and Fumiharu Yamashita in Foot & Ankle Orthopaedics
Footnotes
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board (approval no. 2021-003).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.