
Abstract
This is a visual representation of the abstract.
Keywords
Introduction
The early diagnosis and proper treatment of malignant musculoskeletal neoplasms are critical for patient survival and, when possible, limb salvage.14,54 The variable clinical presentation of malignant bone tumors of the foot and ankle, as well as a potential lack of awareness of such tumors on the differential diagnosis of masses in this body region, may explain the high number of delayed and incorrect diagnoses.9,58
The correct diagnosis of a primary malignant bone tumor requires histopathologic verification of the suspected clinical and radiologic diagnosis. Neoadjuvant and adjuvant treatment may vary and is based on accurate diagnosis. The histologic grading of the respective tumor entity will determine the type of tumor resection necessary. 63
In the calcaneus, several malignant tumors may be treated with wide resection. Basically, any tumor entity, both benign and malignant, can affect the calcaneus. The most common malignant primary bone tumors located at the calcaneus are chondrosarcoma, osteosarcoma, and Ewing sarcoma.48,56 In their 2005 publication on calcaneal tumors, Kilgore and Parrish 31 presented a comprehensive list of the most common entities. Reconstruction of large bony defects after trauma, infection, or tumor resection can be divided into extremity-preserving (limb salvage) and ablative procedures (amputation). Ablative procedures can be further divided into internal and external amputations.
At the foot and ankle, the Pirogoff amputation and its modifications are an example of a partial amputation with the goal of improving function. 3 The Pirogoff technique aims to preserve length and create a residual limb that can support weight while maintaining the stable soft tissue coverage of the heel skin. After amputation of the foot at the level of the Chopart articulation and astralgectomy, the calcaneus is rotated and tibiocalcaneal arthrodesis is performed. 32 Nevertheless, this procedure is not suitable for large defects of the heel bone.
Limb-preserving reconstructions are further divided into biological and allo-arthroplastic procedures. An alloplastic procedure uses synthetic material to reconstruct defects in the body. Using the calcaneus as an example, this might include the use of a 3D-printed calcaneus prosthesis made of titanium. An example of an alloarthroplastic reconstruction after extensive tumor resection of a tumor in the vicinity of the knee or hip joint is the modular megaprosthesis.55,57
Even though the principles of tumor resection according to Enneking (intralesional, marginal, wide, and radical) have been established for decades and are based on the dignity and grading of the lesion, the treatment remains a patient-specific and individual procedure. The same applies to the subsequent defect reconstruction and restoration of function. The purpose of this review is to present different options for defect reconstruction after total or subtotal calcanectomy for malignant tumors of the heel.
Principles of Defect Reconstruction and Surgical Approach
After complete resection of a primary malignant tumor, the main goal of reconstruction following total or subtotal calcanectomy is the restoration of a plantigrade weightbearing foot with preservation of the heel pad. Lower limb amputations are generally associated with a reduced quality of life compared to limb salvage.1,15,20 If the skin of the heel or the medioplantar neurovascular bundle cannot be preserved or reconstructed for oncologic reasons, ablative surgery should be considered.
Various plastic-surgical options are available for reconstruction of the heel pad, depending on individual factors.18,22,24,30 If the tumor is confined to the bone and there is limited soft tissue dissection, the risk of loss of sensation to the heel pad is typically no greater than with open reduction and internal fixation for calcaneal fractures using an extensive lateral approach. The need for osseous reconstruction of the calcaneal defect for subtalar support of the hindfoot is not clear, and the literature is mostly limited to case reports describing different surgical techniques.
Several factors determine the choice of surgical approach. If there are extraosseous tumor manifestations, the surgical approach is largely dictated by the tumor. In principle, it can be performed from lateral, similar to an extended lateral approach for traditional open reduction and internal fixation of calcaneal fractures, or from medial, following the neurovascular bundle. Several authors have described a circumferential Cincinnati incision26,34,36,42 and a bilateral approach from medial and lateral has been used by Farei-Campagna et al. 21 In our experience, however, a single medial or lateral incision is sufficient to facilitate partial and complete calcanectomy. Excess skin after resection arthroplasty is not a problem and does not require resection. The soft tissue envelope consolidates in a timely manner if tension-free wound closure can be achieved.
In the following sections, the options for osseous reconstruction are discussed based on the available literature and demonstrated by exemplary case studies.
Resection Arthroplasty
Functional results after subtotal or total resection of the calcaneus without structural reconstruction are sparsely represented in the literature (Table 1). In 1993, Dhillon et al reported 3 cases of young patients with subtotal calcanectomy for giant cell tumor. Two cases were able to walk barefoot but with mild limping at 6 and 12 months, respectively, and the third case was lost to follow-up. 17 Özerdemoglu et al removed the calcaneus without replacement and transferred the Achilles tendon to the posterior talus in 2003 in a 36-year-old patient with a giant cell tumor of the calcaneus. At 1 year, the patient was pain free and able to return to work. 41 In 2012, Madhuri et al 36 reported the case of a 7-year-old child with a primitive neuroectodermal tumor of the calcaneus who underwent total calcanectomy and transposition of the Achilles to the posterior talus. At 32 months of follow-up, the patient had a smooth, natural gait and strong (4/5) plantarflexion strength. The patient only required a heel wedge in normal footwear.
Literature on Resection Arthroplasty of the Calcaneus.

Abbreviation: AOFAS, American Orthopaedic Foot & Ankle Society.
Article not in English.
No primary malignant bone tumor.
In 2023, we reported our experience of subtotal calcaneal resection for 3 tumor cases: a G2 chondrosarcoma in a 77-year-old female patient and 2 other patients with Ewing sarcomas aged 9 and 31 years. Figures 1 to 4 illustrate the case of the 77-year-old female patient after resection of a calcaneal chondrosarcoma, and Figure 5 the case of the 9-year-old patient with Ewing sarcoma and resection arthroplasty. All 3 patients were able to fully bear weight without assistive devices within 2-3 months of surgery. Two patients required silicone heel pads to compensate for the leg length discrepancy in regular shoes.

Intraoperative photograph after subtotal calcanectomy using an extended lateral approach in a 77-year-old female patient with G2 chondrosarcoma.

(A) Intraoperative fluoroscopy and preparation for transposition of the Achilles tendon to the posterior talus; postoperative magnetic resonance imaging with (B) T1-weighted turbo spin echo and (C) T1-weighted turbo spin echo fat suppressed without evidence of recurrence, suture anchor with transposed Achilles tendon (arrows).

Clinical findings 1 year after subtotal left calcanectomy. The patient was able to walk barefoot without pain and can stand on her left toes with little limitation (B). Clinical images with front (A), back (C) and side views (D).

Lateral weightbearing radiograph 1 year after subtotal calcanectomy with resection arthroplasty and transposition of the Achilles tendon to the posterior lateral talar process.

Radiologic follow-up in a 9-year-old patient with Ewing sarcoma of the calcaneus who underwent subtotal calcanectomy without reconstruction and transposition of the Achilles tendon to the posterior talar process: (A) preoperative, (B) 3 days postoperative, and (C) 10 months postoperative radiographs.
A complete listing of all cases of resection arthroplasty for neoplastic disease of the calcaneus published in the literature, including 1 publication for calcaneal metastases, is presented in Table 1.
Larger case series of total calcanectomies are available from treating infections, especially osteomyelitis of the calcaneus in the setting of diabetic heel ulcers.7,13,45,46,51,52,64,68 However, the results of this patient population, with high rates of revision surgery and reamputation, are not directly comparable with calcanectomy for tumors. Crandall and Wagner 13 reported an overall rate of failure after partial and total calcanectomy for infection and ulcerations of the heel in diabetics of 65%, leading to immediate or secondary amputation. Adequate treatment of the underlying condition, such as peripheral artery disease or diabetes, is critical in these indications.
Madhuri et al 36 analyzed the gait abnormality observed after calcanectomy without reconstruction and concluded that near-normal function is achieved after the operation. These authors, therefore, concluded that complex reconstruction is not necessarily indicated in every pediatric case. This is consistent with our observations for both pediatric and adult cases. 21 In conclusion, resection arthroplasty after total or partial calcanectomy eliminates the risk of implant- or graft-related complications and should be considered in any patient requiring (neo-)adjuvant tumor therapy. The disadvantage of resection arthroplasty is a leg length discrepancy. This can be compensated using orthotics such as silicone heel wedges or custom insoles.
Allogenic Reconstructions
The rationale for any complex calcaneal defect reconstruction is to restore limb length and the Achilles tendon lever arm with the goal of normal ambulation and a plantigrade foot. Structural allograft reconstruction offers the advantages of potential osseous ingrowth from adjacent bone and better availability in some regions compared with patient-specific alloarthroplastic implants. Autologous grafts will always involve some degree of donor site morbidity. In the literature, structural allografts used for calcaneal reconstruction are mostly limited to either allogenic calcaneus or femoral head.
Table 2 summarizes the available literature on allogenic reconstruction after calcanectomy for aggressive and primary malignant tumors. Interestingly, the first allograft reconstruction using a cadaveric calcaneus after calcanectomy was described as early as 1949 by Ottolenghi and Petracchi 39 in a 14-year old boy suffering from chondrosarcoma. Their technique was subsequently described in the English language in 1953 for a case of chondromyxosarcoma. 40
Literature on Structural Allograft Reconstructions of the Calcaneus.

Article not in English.
The longest postoperative interval after reconstruction with allogenic calcaneus graft was reported in 2000 by Musculo et al 38 with a follow-up of 9 and 32 years, respectively, with only mild collapse of the donor bone but a very good functional outcome for daily activities without relevant pain. 40 In 2016, Ayerza et al 5 reported a case series of 6 patients with total allogenic calcaneal transplantation for defect reconstruction and a 5- and 10-year allograft survival of 83%, including a previously reported case. Of the 6 calcaneal allografts in their series, only 1 required further surgery due to an infection. Nevertheless, all patients remained asymptomatic, including a case that had a fracture. All were able to bear full weight without support and had no relevant cosmetic deficit at the last follow-up. 5
Given the rarity of calcaneal defect reconstruction for malignant bone tumors, data from other regions of the musculoskeletal system should be consulted to evaluate the survival of massive allografts. In a series of 718 cases with long-term follow-up of structural allograft reconstruction for bone tumors, Mankin et al reported that after the first year of susceptibility to infection (10%) and the third year of increased risk of fracture (19%), the grafts become stable. Approximately 75% are retained by patients and are considered to be successful for >20 years after implantation.37,38
Figures 6 to 9 illustrate the biological reconstruction using a structural femoral head allograft after wide resection of a poorly differentiated osteosarcoma of the calcaneus in a 41-year-old female patient. During adjuvant chemotherapy, the patient developed a wound dehiscence requiring multiple revisions with wound debridement, negative-pressure wound therapy, and a microsurgical flap. No deep infection was detected, and the graft was preserved. Because of this complication, full weightbearing was not achieved until 5 months after the initial surgery. At the latest follow-up, 2.5 years after subtotal calcanectomy and allogenic reconstruction, the patient was using regular shoes and could walk 400 m without pain.

Preoperative axial MRI of the right calcaneus: (A) T1-weighted turbo spin echo, (B) proton density-weighted fat suppressed, (C) fat-suppressed with intravenous contrast. Note the large extraosseous tumor component medially (arrows).

Intraoperative situs from medial. Achilles tendon (A) looped and (B) anchored to the allograft (black star). The posteromedial neurovascular bundle was looped with blue vessel loops. FDL, flexor digitorum longus; FHL, flexor hallucis longus; PB, peroneus brevis; PL, peroneus longus; PTT, tibialis posterior tendon.

Intraoperative fluoroscopy: (A) marking of the anterior resection plane, (B) lateral projection after “talofemoral” arthrodesis and fusion to the anterior calcaneal process, (C) anteroposterior view.

(A) Lateral and (B) axial radiographs of the calcaneus 12 months postoperatively showing fusion between the residual calcaneus anteriorly and the collum femoris and between the talus and the allogeneic strut graft in the subtalar joint without evidence of screw loosening or implant failure.
In short, reconstruction with allogenic structural grafts, such as femoral head or calcaneal transplants, offers the advantage of restoring physiologic leg length and providing subtalar support. Patients should be counseled regarding the risk of graft subsidence or infection, especially in the presence of adjuvant chemotherapy and radiation therapy. Because allograft reconstruction does not require the microsurgical techniques of autologous osteocutaneous flaps, this type of reconstruction can be performed by the foot and ankle surgeon without assistance from other specialties.
Autologous Reconstruction
Structural autologous bone grafts offer the advantage of optimal healing properties and can be combined with extensive autologous soft tissue reconstruction as warranted for extra-osseous tumor manifestations, including the heel fat pad and skin. The limited availability and the unavoidable donor site morbidity have to be taken into account. Microsurgical techniques for osteocutaneous flaps may require an even more complex approach, with multidisciplinary surgical teams and specialized rehabilitation protocols.
In 2019, Innocenti et al 29 described 4 cases with a mean follow-up of 13 years (range 6-19 years) using a structural autologous iliac crest secured with screws to the talus and cuboid after total calcanectomy. The triceps surae was reconstructed using nonabsorbable sutures to secure the distal Achilles tendon to the graft. Reported complications included fracture of the donor bone, screw breakage, and wound dehiscence. None required surgical revision. All 4 patients had high Musculo Skeletal Tumor Society scores with a mean of 95% (range 90%-97%). The Musculo Skeletal Tumor Society score is a widely used tool for functional evaluation of reconstructive procedures following surgical treatment of musculoskeletal tumors, with higher scores representing better function and less pain. 19 Gait analysis demonstrated an almost normal gait pattern without relevant asymmetry between the 2 limbs in 3 patients and only a mild gait asymmetry in 1 patient, which normalized with shoes. 29 Two of those cases had been previously published in a separate article in 2009. 50
Li et al 34 reported on 5 cases of autologous reconstruction using a distally pedicled osteocutaneous fibular flap. After total calcanectomy for primary malignant bone tumors, pain was completely absent in all patients at the latest evaluation at an average of 50 months postoperatively (range, 32-76 months). No special shoes were needed. Four patients had no evident limp or limitation of daily activities. One patient had a mild limp. All patients could walk for more than half an hour. All but 1 patient were unable to run or jump, though. 34
Other authors have reported the use of a free deep circumflex iliac artery osteocutaneous flap after wide resection of aggressive bone tumors (chondroblastoma and giant cell tumor) or reconstruction of a posttraumatic calcaneal defect situation. 47 Various microsurgical techniques using autologous osteomyocutaneous flaps with fibula, ribs, or tricortical iliac crest have been described after subtotal calcanectomy for bone defects following trauma or infection.2,8,44,47,50
In 2010, Tsuchiya et al 61 reported on a different approach of structural autograft reconstruction using tumor-affected autografts treated with liquid nitrogen. With this technique, hypothermia is used to treat tumor-containing autografts and sterilize tumor cells in the bone. The bone-containing tumor is partially excised from the limb, rotated and immersed in an adjacent container of liquid nitrogen to create a pedicle frozen autograft. 62 In their series of 33 malignant bone tumors, there was 1 case treated for calcaneal pleomorphic sarcoma and involved pedicle freezing that maintained contact with the body via the Achilles tendon. Reconstruction involved arthrodesis using screws. An excellent outcome without complications was reported after 9 months of follow-up. 61
Meanwhile, Wang et al 66 replanted a tumor-affected calcaneus after chemical inactivation. A 73-year-old male patient with chondrosarcoma of the heel bone underwent total calcanectomy and reconstruction with his inactivated calcaneus and bone cement. The resected calcaneus was inactivated using ethanol and fixed to the talus and cuboid using multiple cannulated screws to obtain a construct resembling talocalcaneal and calcaneocuboid arthrodesis. The cement was used to fill the bone defect after intralesional tumor resection, and microscopic tumor remnants were deactivated by ethanol. The Achilles tendon was reattached using a nonabsorbable suture passed through a bone tunnel in the posterior part of the graft. 66
Table 3 provides an overview of the available data on autologous calcaneal defect reconstruction. In summary, autologous reconstruction with structural grafts are usually associated with donor site morbidity. This is obviated, however, by techniques in which the tumor-affected bone is chemically or thermally inactivated and then reimplanted. Time to union and full weightbearing is reported to range between 6 and 9 months.35,61 With both allograft and autologous (vascularized) reconstruction, subtalar joint mobility is lost, and the primary benefit is the lever arm for triceps surae function and leg length preservation.
Literature on Structural Autograft Reconstructions of the Calcaneus.
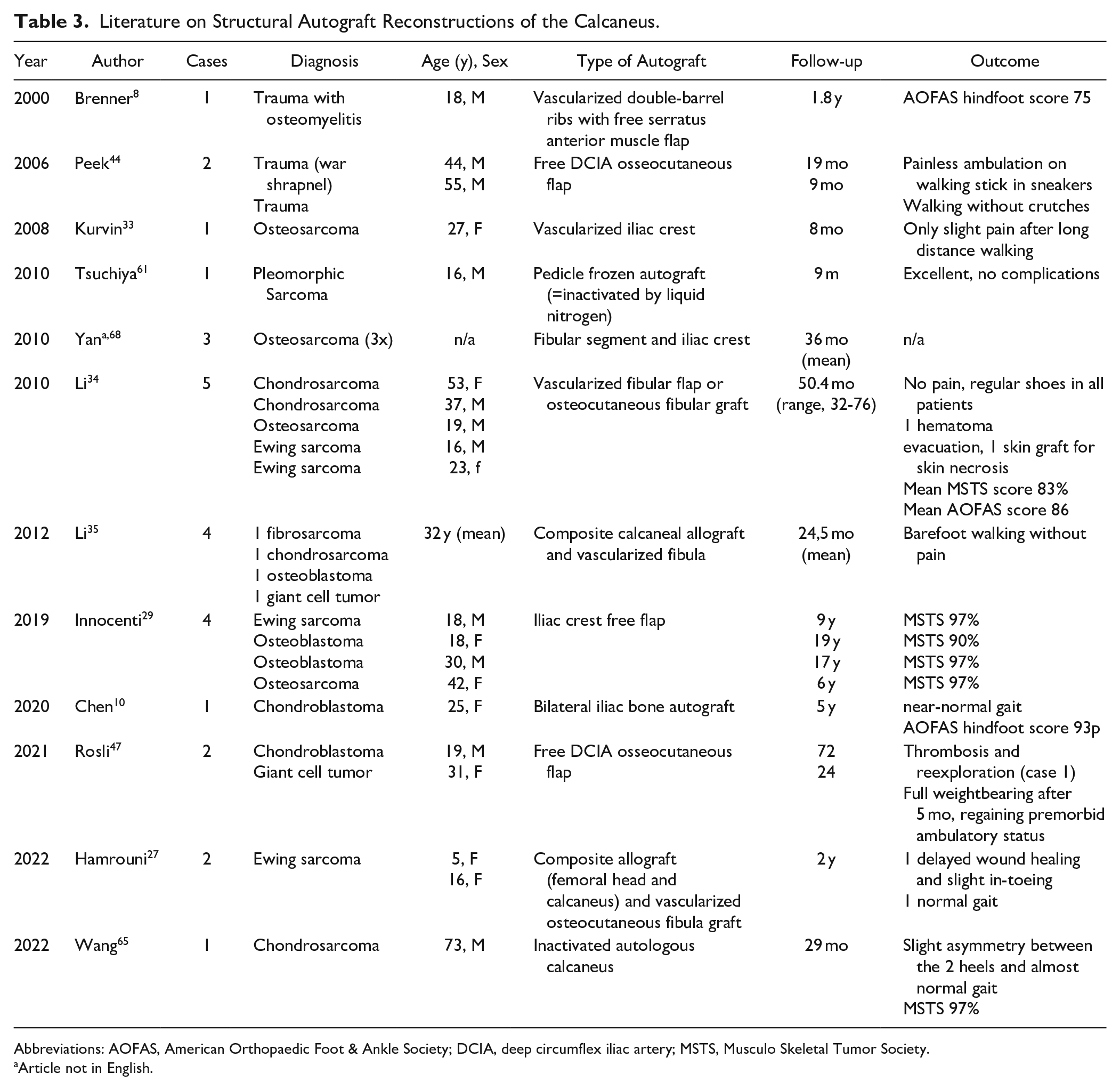
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; DCIA, deep circumflex iliac artery; MSTS, Musculo Skeletal Tumor Society.
Article not in English.
Alloplastic Reconstruction
Alloplasty can be defined as a surgical procedure performed to substitute and repair defects with the use of synthetic material. Alloarthroplasty is the surgical method of reconstructing and replacing a damaged or deformed joint. Numerous implant types from various manufacturers have been on the market for decades. However, no joint replacement is available for the subtalar or calcaneocuboid joints. For this reason, reconstruction after total calcanectomy most often necessitates fusion between the calcaneal implant and talus to ensure subtalar stability. Some authors described the use of a smooth and polished joint surface to preserve the subtalar joint.28,43 Generally speaking, calcaneal alloplastic implants are custom-made and patient-specific.
Table 4 lists the current state of the scientific literature on alloplastic calcaneal replacement. Publications on defect reconstruction after trauma are not included but can provide helpful information on this rare indication.49,53,70
Literature on Alloplastic Reconstructions of the Calcaneus.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; MSTS, Musculo Skeletal Tumor Society.
Article not in English.
In 1998, Chou et al 12 first reported a limb-sparing surgery with a custom calcaneal prosthesis for a high-grade osteosarcoma in a 31-year-old female patient. The calcaneal prosthesis had been constructed using a 3D CT scan and incorporated a porous coating to allow for soft tissue ingrowth and screw holes for fixation to the talus. The dimensions were identical to the patient’s calcaneus, including the articular facets. At the 36-month follow-up, the patient was able to walk well using an orthotic device with minimal pain in her plantar heel. Radiographs showed no loosening of the prosthesis or evidence of recurrence. 12 The same case was published again in 2007, now providing long-term follow-up of 12 years. The patient was still tumor-free and reported mild to moderate pain at the plantar heel fat pad with weightbearing activities, leading the authors to conclude that a calcaneal prosthesis is a viable option for reconstruction after calcanectomy. 11
In 2015, Imanishi et al 28 first described the use of additive manufacturing to create a prosthetic calcaneus. The implant was a mirror image of the contralateral calcaneus and was produced using an electron beam melting 3D printer. The corresponding articular surfaces were polished, and the rest of the prosthesis showed a mesh structure to promote tissue integration.
Papagelopoulos published a staged approach of 2 cases of Ewing sarcoma requiring total calcanectomy that were reconstructed using a custom-made, 3D-printed implant. First, a handmade cement spacer was used to fill the resection defect after calcanectomy. Histologic examination showed tumor-free surgical margins. After the completion of adjuvant chemotherapy and 9 months after the initial operation, the patients were scheduled for calcaneal reconstruction. The authors noted that the implants were designed to be smaller than the original bone to permit soft tissue coverage and avoid wound closure complications. The implant was fitted with a stem that was introduced and fixed to the talus with the use of a customized impactor. The Achilles tendon was reattached to the posterior surface of the implant using nonabsorbable sutures. 42
In a series of 41 patients treated with a 3D-printed custom-made prosthesis for reconstruction of bone defects after resection for a bone tumor or challenging revision surgeries, Angelini et al reported 1 case of calcaneal reconstruction in a 60-year-old female patient with chondrosarcoma. Skin necrosis and wound dehiscence required surgical debridement, antibiotic therapy, negative-pressure wound therapy, and finally revision surgery with a musculocutaneous flap without implant removal. 4
Farei-Campagna et al reported their experience with 3 cases of alloarthroplastic calcaneal replacement for malignant bone tumors in 2023. Two cases resulted in transtibial amputations: In the first case, a 20-year-old female patient had total calcaneal resection and replacement for Ewing sarcoma. The joint became stiff and painful, yet ambulation was possible without the use of orthotic devices. One year after the surgery, a fall down the stairs led to avulsion of the Achilles tendon. Subsequent wound breakdown of the irradiated skin (after neoadjuvant radiation therapy) with deep infection necessitated transtibial amputation. Five years after the amputation, the patient was a high-level athlete. In the second case, transtibial amputation was required for extracompartmental tumor recurrence in a 39-year-old male patient with grade II chondrosarcoma with Ollier disease 1 year after complete tumor resection and total calcaneal replacement (Figures 10-12). The third patient in this series was a 45-year-old woman who was treated with a hemicalcaneal replacement for hemangioendothelioma. She had a stress fracture of the sustentaculum tali, which required no further surgical intervention. 21
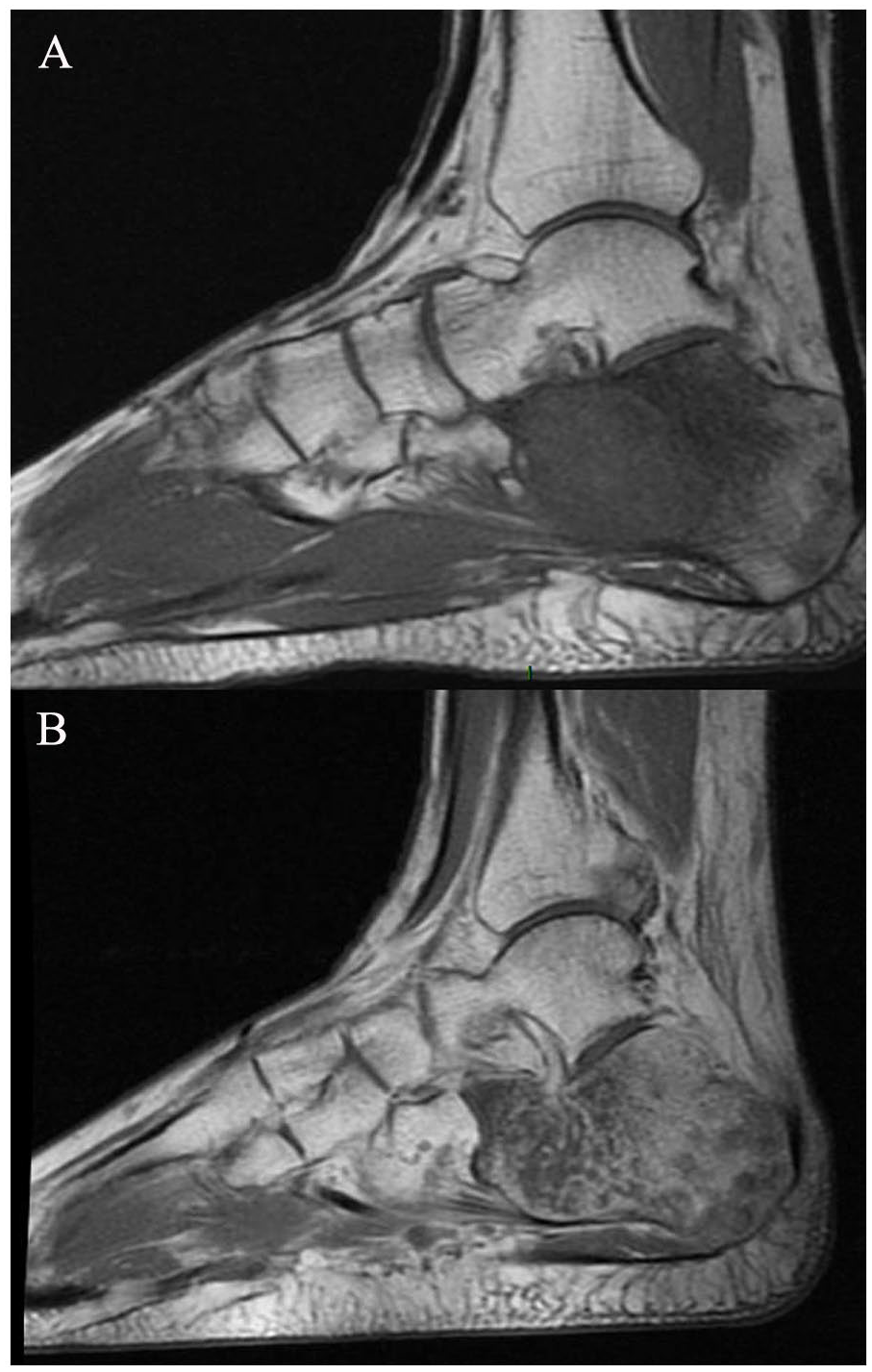
(A) Preoperative sagittal T1-weighted magnetic resonance imaging and (B) after gadolinium administration with a chondrosarcoma in a 39-year-old male patient with Ollier disease.
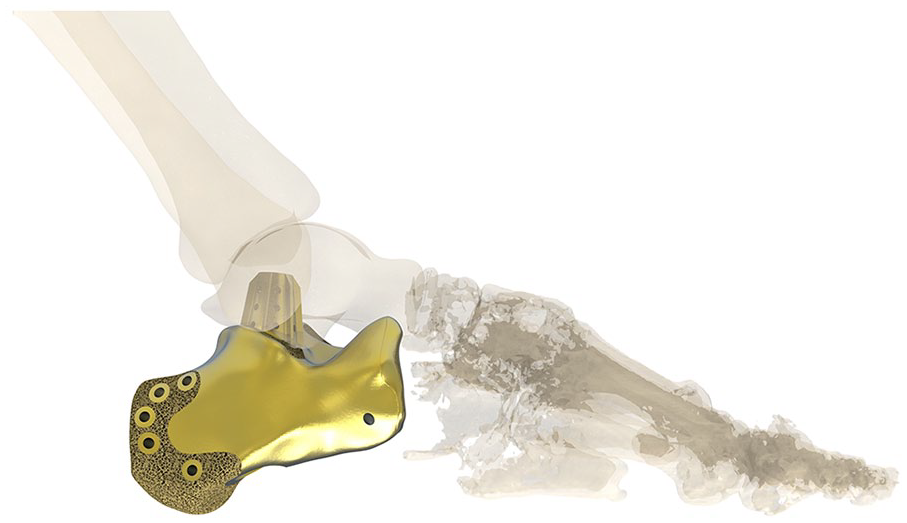
Preoperative rendering of the implant.

(A) Immediate postoperative lateral radiograph and (B) 1-year postoperative radiograph. Eventually the patient required transtibial amputation for an extracompartmental tumor recurrence.
In conclusion, alloplastic calcaneal defect reconstruction eliminates the risks associated with allogenic bone (eg, fracture/subsidence, potential disease transmission) or autologous grafts (donor site morbidity, microsurgery) but is not free of complications either. Implant-related infections can ultimately lead to below-knee amputation. The combination of massive metal implants and limited soft tissue coverage always carries an increased risk of failure, especially in patients requiring adjuvant systemic tumor or local radiation therapy. As noted by Farei-Campagna et al, 21 radiotherapy should be considered a relative contraindication for alloplastic reconstruction.
Technical Considerations for Alloplastic Calcaneal Reconstruction
The data used to design and create an individual prosthesis of the calcaneus usually comes from a CT of the opposite side and is mirrored. From the digital 3D data, the structure and geometry of the implant component is built up layer by layer by applying an electron beam of titanium alloy powder (TiAl6V4). The implants can be covered with a highly porous surface, which should allow ingrowth of bone tissue and soft tissues and thus long-term secondary anchorage. An additional thin, bioactive calcium phosphate layer can be applied to support osteointegration. The implant may have perforations that facilitate the attachment of the Achilles tendon. The fabrication process requires approximately 4 weeks, which must be considered when planning the definitive tumor resection and reconstruction. Temporary defect filling with polymethyl-methacrylate spacers allows time to await final histopathology results.
It is recommended that the custom-made implant be planned 10% smaller than the original bone to ensure a better fit and less stress on the soft tissue envelope. This also takes into account the cartilage layer, which is not shown on CT, and thus will avoid overstuffing. The plantar contact point of the implant should be designed as wide as possible to avoid point-loading and pain on weightbearing. Attachment of the plantar fat pad to the implant is recommended to avoid heel pad migration, similar to its fixation after Syme amputation.
If fusion of the subtalar joint is desired, a short porous talar stem can provide additional stability. If the subtalar joint will be preserved, the joint surface of the implant has to be smooth and polished. A meshed metal or hydroxyapatite-coated surface, with multiple free holes for suturing the Achilles tendon and surrounding ligaments, provides adherence to the adjacent soft tissues with scarring for long-term stability.23,43 For total calcanectomy, fusion of the calcaneocuboid joint should be considered as instability can develop in the Chopart joint.
The lead time to definitive surgery will be further reduced by advances in the manufacturing process for customized prostheses. It is expected that modern implant designs will help to improve primary stability and, therefore, the long-term survival of the prosthesis.
Discussion
To date, the literature provides limited data regarding the options for calcaneal defect reconstruction after wide resection of malignant bone tumors. Most reports are limited to single cases or small case series. Based on the available scientific evidence and this review, it is not possible to create an algorithm that guides definite management. Given the different resources available to reconstruct large bone defects, the existing reports tend to reflect only 1 technique, and no comparative studies have been performed.
Although most reports describe complex and technically demanding techniques, including composite allograft-autograft transplantation procedures with microsurgical osteocutaneous anastomoses or custom-made 3D-printed implants, reports of simple resection arthroplasty without sophisticated reconstruction may be underrepresented. The advantages of resection arthroplasty are shorter operation times, faster rehabilitation (no osseous consolidation required), and lower costs. Moreover, all implant- and graft-related complications, such as periprosthetic infection and graft or hardware failure are eliminated. According to the literature, resection arthroplasty may be superior to complex reconstruction in a select group of patients.36,21,41
Because of the rarity of calcaneal defect reconstruction for neoplasia, there is also a lack of comparison with limb ablation techniques. However, it is generally accepted that limb salvage improves patients’ quality of life, including better functional outcomes and emotional acceptance.1,15,20 Radical tumor resection, which is equivalent to amputation when the hindfoot is involved, does not provide better oncologic results.
Conclusion
A complete, wide resection with tumor-free margins is a prerequisite for the long-term tumor-free survival of patients suffering from malignant primary bone tumors. The type of tumor resection and reconstruction is primarily the responsibility of the orthopaedic surgeon and requires a thorough knowledge of all available treatment options.
The advantages and disadvantages of the different procedures must be individually assessed. Numerous factors, such as comorbidities, age, activity level, and adjuvant forms of therapy should be considered in the decision-making process. Complex reconstructions may not be indicated in patients with diminished immune response, impaired blood circulation, and older age. Resection arthroplasty is a suitable alternative to structural biological grafting or custom-made prostheses for calcaneal defect reconstruction, reducing the stress on the adjacent soft tissues and decreasing the risk of severe perioperative complications.
Regardless of the type of reconstruction, most patients can expect to walk barefoot without the use of orthotic devices. Although tumors of the foot and ankle are rare and their treatment is often left to colleagues with subspecialty training in orthopaedic oncology, the expertise of a foot and ankle surgeon may play an important role in reconstructing defects following the resection of aggressive or malignant tumors.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241266247 – Supplemental material for Principles of Defect Reconstruction After Wide Resection of Primary Malignant Bone Tumors of the Calcaneus: A Contemporary Review
Supplemental material, sj-pdf-1-fao-10.1177_24730114241266247 for Principles of Defect Reconstruction After Wide Resection of Primary Malignant Bone Tumors of the Calcaneus: A Contemporary Review by Andreas Toepfer, Primoz Potocnik, Norbert Harrasser, Thomas Schubert, Zeeshan Khan and Jan Marino Farei-Campagna in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.