
Abstract
Background:
Academic medicine emphasizes the need to recruit a diverse workforce in graduate medical education. Orthopaedic surgery residency has demonstrated efforts to model program compositions with evolving US demographics. However, it remains unclear whether orthopaedic fellowships, particularly foot and ankle, also reflect these efforts.
Methods:
Using the publicly available Accreditation Council for Graduate Medical Education (ACGME) Data Resource Book, a census of the gender and racial/ethnic identities of orthopaedic foot and ankle fellows, as well as active orthopaedic surgery residents, were compiled from 2007 to 2022. Linear trend analysis was conducted to evaluate the trends of orthopaedic residents and foot and ankle fellows, with a Pearson correlation for comparison.
Results:
Prior analysis demonstrated no significant change in sex and ethnic diversity of fellows from 2006 to 2015. The majority of foot and ankle fellows were White (31%-69%) and male (63%-88%). Linear analysis demonstrated growing diversity in female and non-White active orthopaedic surgery residents. Similarly, there was an increasing number of female foot and ankle fellows (0%-38%) reflective of the trend in orthopaedic residency (12%-20%); however, there was no significant change among racial/ethnic identities. Pearson correlation analysis between the trend of orthopaedic residency residents and foot and ankle fellows suggests moderate correlation among female, Asian, and “Unknown” racial/ethnic categories.
Conclusion:
The proportion of foot and ankle female fellows in ACGME-accredited fellowships has matched or exceeded the percentage of female orthopaedic residents. Despite increased diversity of orthopaedic surgery residents over the past 2 decades, ACGME-accredited foot and ankle fellowships do not yet reflect similar trends among racial/ethnic minorities.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
In the United States, there has been a significant growth in non-White minority groups over the last few decades. They have been found to comprise nearly 40% of the US population. 24 Despite this increase in diversity, the percentage of medical school enrollees from racial and ethnic backgrounds underrepresented in medicine (URiM) continues to remain well below their percentage makeup in the US Census.15,16 These disparities are even more prominent in the field of orthopaedic surgery, which is considered among the least racial, ethnic, and gender diverse surgical specialties.6,7,10,17,19 Despite initiatives such as Nth Dimensions, the Perry Initiative, the Ruth Jackson Orthopaedic Society, and the J. Robert Gladden Orthopaedic Society, recruitment efforts to promote minority and female representation have not significantly improved diversity in orthopaedic residency programs. 18 Further efforts to improve on this discordance is paramount given the impact race and sex have on quality of life and surgical outcomes.9,26
Although prior studies have examined demographic characteristics among medical schools and orthopaedic residency programs, literature identifying such trends in orthopaedic fellowship programs is sparse. This is especially pronounced within foot and ankle fellowships, with most studies highlighting the scarcity of women and minorities among foot and ankle leadership.4,8,27 Unequal representation among faculty is the greatest perceived barrier to orthopaedic residency program diversity, 14 and with an increasing number of foot and ankle fellowship applications, 20 understanding the composition of current residents is critical to determine if the homogeneity within the field is being perpetuated, and to take steps to improve diversity. Poon et al 18 previously examined the ACGME database to assess gender and racial parities in various orthopaedic subspecialities. The results of this study found ACGME-accredited foot and ankle fellowship selection was fourth among female applicants and did not find any significant changes in the diversity profile of foot and ankle fellows from 2006 to 2015. The purpose of this study was to identify demographic trends among orthopaedic ACGME-accredited foot and ankle fellows and analyze whether they align with those of orthopaedic residents from 2007 to 2022.
Methods
Using the publicly available ACGME Data Resource Book, we compiled the demographic data of US orthopaedic ACGME-accredited foot and ankle fellows from 2007 to 2022. 1 Approximately 85% of fellows are graduates of US orthopaedic programs. The gender of fellows, reported as male, female, and not reported, is available from 2007 to 2022. The racial/ethnic identity of fellows, reported as White, Asian, Hispanic, Black or African American, Native American, Native Hawaiian, Other, or Unknown, is available from 2011 to 2022. We calculated the annual percentage of fellows within each category. Using the same gender and racial/ethnic categories, we tabulated the percentage equivalent of active US orthopaedic residents within each identity across the respective study periods.
Linear trend analysis with a Mann Kendall test was performed for each respective gender and racial/ethnic identity to determine any statistically significant change in percentage over the study period. The Mann Kendall test statistic assesses for monotonic trends in a time series by comparing the number of concordant and discordant pairs of data points. A lagged version of the data set was produced by percentage of residents and fellows from prior years. Statistical significance was determined at P < .05. The “Not Reported” and “Unknown” gender categories were excluded from analysis because no values were reported during the study period. The “Native American” and “Native Hawaiian” racial/ethnic categories were excluded from analysis in the fellow group because no values were reported during the study period. There was an inadequate sample of fellows (n = 3) in the “Other” racial/ethnic identity and was thus excluded from analysis.
A Pearson correlation coefficient was used to compare the trends between orthopaedic surgery residents and fellows regarding a specific gender or racial/ethnic category label. Categories excluded from linear analysis of trends were excluded from this analysis. All statistical analyses were conducted on R Studio (ver. 2023.06.01 + 524).
Results
Demographics of Active Orthopaedic Surgery Residents
From 2007 to 2022, male and female residents composed 80% to 83% and 12% to 20% of the sample, respectively (Figure 1). The number of male residents demonstrated a small decline compared with an uptick in female residents. Mann Kendall testing demonstrated that both groups had a statistically significant change in percentage over the study period (P < .001, Table 1). From 2011 to 2022, the majority of residents identified as White (57%-73%, Figure 2). Residents who identified as Asian (9%-14%), Hispanic (3%-8%), Black or African American (3%-5%), Native American (0%), and Native Hawaiian/Pacific Islander (0%) did not constitute a percentage of residents over the entire study period (Figure 2). The percentage of residents who identified as Other (2%-4%) and those who were Unknown (1%-25%) also remained low (Figure 2). Over the study period, there was a notable decrease in the percentage of White residents. Conversely, the percentage of Asian and Hispanic residents revealed an upward trend. Linear trend analysis demonstrated that White (P = .019), Asian (P = .042), and Hispanic (P < .001) residents had significant change in percentage (Table 2).

Percentage of active orthopaedic residents according to gender from 2007 to 2022.
Mann Kendall Test for Statistically Significant Change in Percentage of Resident and Fellow Gender From 2007 to 2022.

P < .05 can be interpreted as a significant monotonic trend in the time series of the category during this period.

Percentage of foot and ankle fellows according to gender from 2007 to 2022.
Mann Kendall Test for Statistically Significant Change in Percentage of Racial/Ethnic Profile of Orthopaedic Surgery Residents From 2011 to 2022.

P < .05 can be interpreted as a significant monotonic trend in the time series of the category during this period.
Demographics of Orthopaedic ACGME Foot and Ankle Fellows
A total of 251 ACGME foot and ankle orthopaedic fellows were studied. From 2007 to 2022, male fellows constituted 63% to 88% of the sample (Figure 3). Mann Kendall testing demonstrated there was no significant change in the percentage of this cohort during this study period (P = .92, Table 1). Over the study period, female fellows composed 0% to 38% of the cohort with a notable increase of 31% over 2014-2019 (Figure 3). Mann Kendall testing demonstrated this was a significant upward trend (P = .047, Table 1). Similar to residents, the majority of ACGME foot and ankle fellows identified as White (31%-69%). A notable portion of fellow racial/ethnic identities was Unknown (13%-47%). A small percentage of fellows identified as Asian (6%-31%), Hispanic (0%-12%), and Black/African American (0%-6%). It is worth noting that Hispanic and Black/African American fellows were only present for 2 years across the study period while comprising 0% in the remaining years (Figure 4). No fellows identified as Native American or Native Hawaiian/Pacific Islander across the study period. Linear trend analysis shows that there were no significant changes in percentages in any racial/ethnic category (Table 3).

Percentage of active orthopaedic surgery residents according to race/ethnicity from 2011 to 2022.

Percentage of foot and ankle fellows according to race/ethnicity from 2011 to 2022.
Mann Kendall Test for Statistically Significant Change in Percentage of Racial/Ethnic Profile of Foot and Ankle Fellows From 2011-2022.
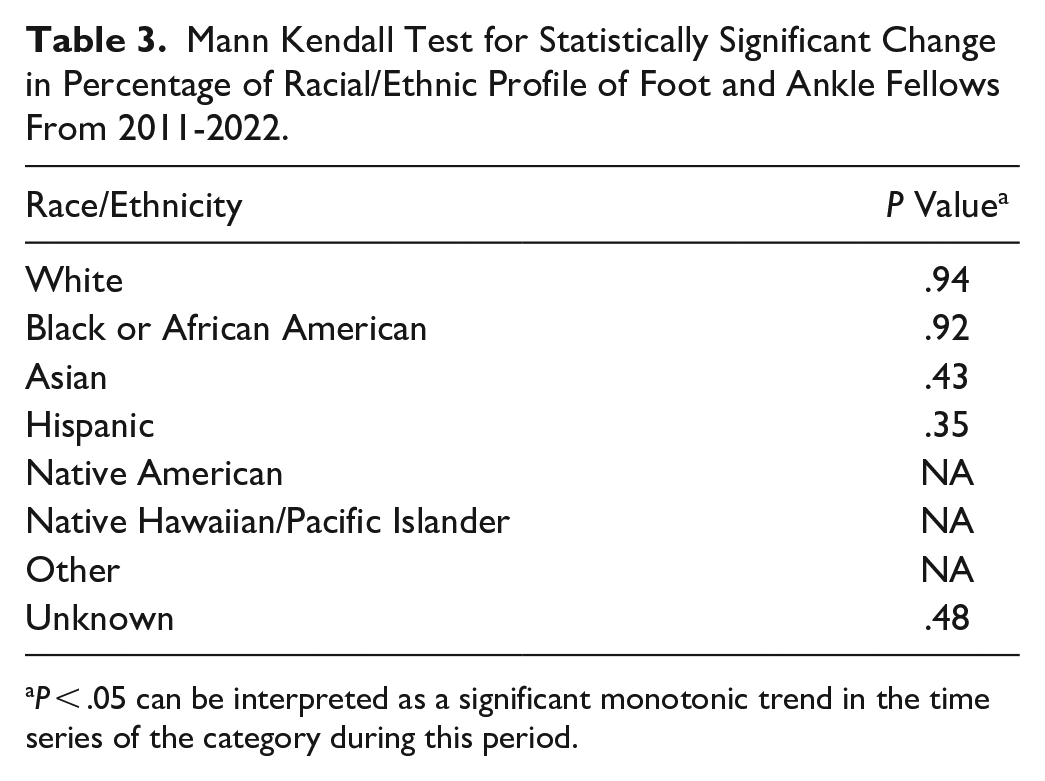
P < .05 can be interpreted as a significant monotonic trend in the time series of the category during this period.
Comparison of Demographic Trends Between Orthopaedic Surgery Residents and ACGME Foot and Ankle Fellows
A Pearson correlation coefficient between the trends of female residents and female foot and ankle fellows demonstrated moderate correlation (r = 0.59). A comparison of the trends in Asian residents and fellows also demonstrated moderate correlation (r = 0.42). Pearson correlation analysis for individuals identifying as Male (r = 0.19), White (r = 0.02), Black or African American (r = 0.06), and Hispanic (r = 0.31) showed weak correlation between the trends in orthopaedic residents and fellows (Table 4).
Correlation Between Trend of Orthopaedic Surgery Residents and Foot and Ankle Fellows by Gender or Racial/Ethnic Identity.

r <0.4 was characterized as weak correlation; 0.4 < r < 0.6 was characterized as moderate correlation; r > 0.6 was characterized as strong correlation.
Discussion
The present study aimed to characterize the trends in racial, ethnic, and gender profiles of orthopaedic ACGME foot and ankle fellows. Previous research by Poon et al 18 revealed a lack of significant change in the sex and ethnic diversity among foot and ankle fellows in ACGME-accredited institutions spanning from 2006 to 2015. Building on this foundational work, our study aims to ascertain whether advancements in the field have corresponded to an improvement in recent ACGME-accredited foot and ankle program demographics with a newly updated data set reflective of the past decade. Although Poon et al 18 explored the broader impact of orthopaedic residency demographics on fellowship composition, our study takes a more focused approach, conducting a detailed analysis of how residency demographics influence the specific trends observed within ACGME-accredited foot and ankle fellowships. Although there are measures in place to match the nation’s growing diverse population, academic medicine lags behind emerging US demographics. 3 Similarly, graduate medical programs strive to increase the diversity of classes, but these efforts fall short in orthopaedic residency and even more so in orthopaedic fellowships. It is increasingly common for orthopaedic residents to pursue a fellowship. However, diversity becomes increasingly sparse as a physician becomes more specialized, 18 and our study affirmed this finding at least among ACGME foot and ankle fellows over the past 2 decades.
Women are not as well represented in surgical subspecialties, particularly orthopaedic residency. 17 Orthopaedic surgery is often associated with demanding physical labor and a difficult lifestyle, which can be perceived as unsustainable by female applicants.13,28 However, there have been improvements in gender disparity within the field. We found that there has been an encouraging increase in the percentage of female orthopaedic surgery residents and a corresponding increase in female orthopaedic ACGME foot and ankle fellows over the past 2 decades. Previous studies have shown that factors increasing female representation in surgical subspecialty programs include leadership programs, same-sex mentors, and female applicant sponsorships. 12
Our study found that representation of URiM individuals has remained persistently low in orthopaedic surgery and fellowships in the past decade. 21 Some racial/ethnic identities such as Native Hawaiian/Pacific Islander have yet to constitute a substantial portion of the orthopaedic workforce. There have been studies suggesting barriers to orthopaedic residency stem from the selection process. 14 URiM individuals may have matching academic statistics and still find themselves on unequal ground. Efforts should be taken to encourage URiMs to apply into orthopaedics and surgical subspecialties, and to overcome any unconscious biases that may hinder diversification.
Previous studies have demonstrated the importance of diversity among physicians. A concordance between physician and patient racial and ethnic identity results in favorable health outcomes, as well as patient satisfaction and greater treatment adherence.23,25 To promote diversification within the field of orthopaedic surgery, initiatives such as the Nth Dimensions, The Perry Initiative, the Ruth Jackson Orthopaedic Society (RJOS), and The J. Robert Gladden Orthopaedic Society (JRGOS) were created for students early in their medical careers to increase exposure and recruitment of women and underrepresented minorities. Although Poon et al 18 found that such efforts have not reversed the homogeneity within the field, a recent study found that 80% of women who were awarded the RJOS scholarship ultimately pursued a career in orthopaedics, highlighting how scholarship opportunities can help overcome barriers into orthopaedic surgery. 2 Although organizations such as JRGOS and Nth Dimensions provide mentorship and scholarships to attend national meetings such as the American Academy of Orthopaedic Surgeons Annual Meeting,5,13 funding for additional scholarships to conferences at the regional or state levels would significantly broaden outreach and the number of available opportunities. Similar to initiatives that strive to integrate medical students from diverse backgrounds into orthopaedic surgery, fellowship programs can enhance their inclusivity by forging partnerships with multicultural societies like the J. Robert Gladden Orthopaedic Society. Such collaborations can foster resident exposure and mentorship in specialized areas of interest. These partnerships may entail implementing pipeline programs, sponsoring residents’ attendance at specialty-specific conferences, and proactively recruiting residents from diverse backgrounds. Moreover, we acknowledge the cascading impact of demographic diversity and firmly believe that broadening the diversity spectrum within orthopaedic surgery overall will inevitably enrich the composition of foot and ankle fellowship cohorts. Additionally, orthopaedic surgery residency websites 11 and program directors can improve on their commitment to diversity through program-specific initiatives and adopting a philosophy of complete transparency with regard to resident selection to promote program inclusivity.
Overall, ACGME-accredited foot and ankle surgery fellowships remain underrepresented among females and racial/ethnic minorities despite a noteworthy increase among orthopaedic surgery residents. One possibility is that diversity among ACGME accredited foot and ankle fellowships may simply lag behind growing trends among residents given that orthopaedic surgery residency is a 5- or 6-year program. Another plausible explanation is that orthopaedic foot and ankle surgery is a relatively new specialty compared with some other orthopaedic subspecialties. The hope is that orthopaedic foot and ankle surgery interest will continue to grow as experienced senior faculty and energetic young faculty alike provide more education and exposure to residents during training.
Silvestre et al 22 determined that foot and ankle fellowships accounted for one of the smallest percentage of fellowships accredited by the ACGME. Certain health care systems mandate either having ACGME certifications or being eligible for them to gain attending privileges. Moreover, the significance of accredited fellowship training in orthopaedic surgery has gained attention because of perceived difficulties in current surgical training and the enhanced clinical results seen among surgeons with fellowship training. 22
Alternatively, not all orthopaedic residents pursue subspecialty fellowship training, and it is possible that orthopaedic surgery residents of diverse gender and racial/ethnic backgrounds may be more likely to enter practice directly after residency, whether to delay or skip fellowship training altogether. To combat this, professional societies like the American Orthopaedic Foot & Ankle Society (AOFAS) may leverage existing programs like the Women’s Leadership Initiative and Diversity, Equity, and Inclusion and create new initiatives focusing on racial/ethnic backgrounds to increase diversity within the field.
A strength of this study is the multiyear sample gathered from the ACGME database to portray the composition of current orthopaedic surgery residents. Conversely, a limitation of this study was analyzing data only from ACGME-accredited fellowships, which likely offer less than 20% of all fellowship positions. Presently, there is no aggregate data of non-ACGME fellowships. It is possible that variations in diversity could exist between ACGME and non-ACGME programs. ACGME-accredited programs often adhere to institutional guidelines that prioritize diversity and inclusion. In contrast, non-ACGME programs may not have the same level of accountability or commitment to diversity initiatives. The inclusion of non-ACGME data may differ from the observed trends. In order to address the limited sample size, we conducted analysis with changes in proportions rather than individual fellow counts. Thus, we believe the trends we ascertained in this study are reflective of the demographic changes in ACGME foot and ankle fellowships and may be generalizable. The American Orthopaedic Foot & Ankle Society identifies 49 fellowships that are accredited, thus resulting in a substantially smaller group size that may not accurately reflect small but potentially significant trends. Moreover, the ACGME Data Resource Book relies on self-reported data and can have inaccuracies. A comprehensive review of all foot and ankle fellowships could clarify the demographic profile of fellows, as well as help evaluate other orthopaedic fellowships.
Conclusion
In conclusion, there has been an increase in diversity among orthopaedic surgery residents but not yet as much among foot and ankle fellows over the past 2 decades. In recent years, female ACGME foot and ankle fellows constitute a percentage that reflects the composition found in the orthopaedic resident cohort.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241263056 – Supplemental material for A Comparison of Demographic Diversity Between Orthopaedic Surgery Residents and ACGME Foot and Ankle Fellows From 2007 to 2022
Supplemental material, sj-pdf-1-fao-10.1177_24730114241263056 for A Comparison of Demographic Diversity Between Orthopaedic Surgery Residents and ACGME Foot and Ankle Fellows From 2007 to 2022 by Aditya Joshi, Andrew Kim, Nigel Hsu, Amiethab Aiyer and John M. Thompson in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.