
Abstract
Background:
Climate change poses a substantial threat to human health, and operating rooms (ORs) have an outsized environmental impact. The Program for Research in Sustainable Medicine (PRiSM) designed a protocol for minor foot and ankle surgery intended to reduce waste, streamline instrument trays, and minimize laundry. We conducted a randomized controlled trial to compare the carbon footprint of procedures performed using the PRiSM protocol vs a traditional protocol.
Methods:
Forty adult patients undergoing foreign body removal, hammertoe correction, toe amputation, hardware removal, mass excision, or gastrocnemius recession were randomized to the PRiSM or our “Traditional” protocol. The PRiSM protocol used a smaller instrument tray, fewer drapes and towels, and minimal positioning blankets. No changes were made to surgical site preparation or operative techniques. Environmental impact was estimated using the carbon footprint, measured in kilograms of carbon dioxide equivalents (CO2e). Emissions associated with OR waste, instrument processing, and laundry were calculated.
Results:
On average, PRiSM cases had a smaller carbon footprint than Traditional cases (17.3 kg CO2e [SD = 3.2] vs 20.6 kg CO2e [SD = 2.0], P < .001). Waste-associated emissions from PRiSM cases were reduced (16.0 kg CO2e [SD = 2.7] vs 18.4 kg CO2e [SD = 1.8], P = .002), as were modeled instrument processing–related emissions (0.34 vs 0.91 kg CO2e). One superficial surgical site infection occurred in each group.
Conclusion:
We found a small but statistically significant reduction in the environmental impact of minor foot and ankle surgery when using the PRiSM vs Traditional protocol. The environmental impact of these cases was dominated by plastic waste–related emissions. Orthopaedic surgeons should think critically about what components of their surgical setup are truly necessary for patient care, as minor changes in product utilization can have significant impacts on waste and greenhouse gas emissions.
Level of Evidence:
Level I, randomized controlled trial.
Introduction
Global warming and increasingly unpredictable climate patterns have a detrimental impact on human health, and there is widespread recognition that climate change poses a significant global health threat. 5 Human activities, such as those within the orthopaedic operating room (OR), contribute to climate change by generating greenhouse gases (GHGs) that trap infrared radiation from the earth’s surface. ORs have been found to use up to 6 times as much energy as clinical wards and produce 50% to 70% of the waste generated by hospitals.9,12,25 Orthopaedic surgeons can take a leading role in enhancing environmental sustainability within the OR and contribute to efforts to curb climate change.
Although there is little written on the environmental impact of orthopaedic surgery,11,13,14,31 previous studies have identified target areas with the highest potential for reducing the carbon footprint of the OR.7,23,25 These include reducing OR waste, minimizing energy consumption (eg, via optimizing heating, ventilation, and air conditioning systems and setbacks for OR lights), more conscientious purchasing (eg, fewer single-use devices), optimizing sterilization and reprocessing of surgical instruments, and discontinuing use of certain anesthetic gases. Although some target areas require systems-level adaptations, others are within the confines of what is immediately controllable by the surgical team. Therefore, the Program for Research in Sustainable Medicine i (PRiSM) developed a protocol for minor foot and ankle surgery that incorporates such changes and aims to safely reduce the carbon footprint of common procedures. This protocol involves using a minimalist approach for patient draping and positioning and a smaller instrument tray to reduce the carbon emissions from waste, laundry, and instrument processing.
The objective of this prospective, randomized controlled study was to compare the PRiSM protocol to the traditional protocol for minor orthopaedic foot and ankle surgery. Specifically, we sought to determine if these protocols differ significantly with respect to their carbon footprint and safety. We hypothesized that the PRiSM protocol would result in a significantly smaller carbon footprint with no difference in the rate of surgical site infections (SSIs) when compared to the traditional approach. With hundreds of minor foot and ankle surgeries performed each year at our institution, should the PRiSM protocol significantly reduce carbon emissions, its universal adoption could result in a meaningful reduction in the environmental impact of our specialty.
Methods
Study Design
Institutional review board approval was obtained prior to beginning this prospective, randomized controlled study.
All surgeries took place at a single ambulatory surgery center associated with a large academic hospital in a metropolitan region of the United States. Procedures were performed by 3 fellowship-trained orthopaedic foot and ankle surgeons. The primary outcome of this study was total procedure carbon footprint as measured by waste-related, instrument processing–related, and laundry-related GHGs. The secondary outcome was rate of SSI.
Study Population
All adult, English-speaking patients undergoing an isolated gastrocnemius recession, foot or ankle foreign body removal, mass excision, toe amputation, Morton neuroma decompression or excision, hammertoe correction, or hardware removal were eligible. Forty patients were included from March 2023 to August 2023, with 20 patients randomized to the “PRiSM” group and 20 patients randomized to the “Traditional” group.
Sample Size
Prior literature on the carbon footprint of foot and ankle surgery for computing an a priori sample size calculation was unavailable. However, a recent retrospective study in the hand literature comparing the carbon footprint of endoscopic vs open carpel tunnel surgery used a sample size of 28. 31 Because our study includes multiple procedures, we anticipated more variability and thus concluded that a sample size of 40 would provide sufficient power to detect a significant difference in the carbon footprint between protocols. We further conducted a post hoc power analysis to retrospectively calculate the power of our study to detect a difference in carbon emissions between these protocols given our sample size. The results of this analysis revealed an effect size of 1.2 (large effect) and a power of 0.98. The G*Power 3.1.9.7 program was used for this calculation. 8
An a priori sample size calculation regarding our secondary outcome, SSI rate, was performed using α = 0.05 and 80% power to detect a doubling of the expected 4% SSI rate reported in the literature for foot and ankle surgery. 4 This resulted in a sample size of 1106. Because the surgical site preparation remained the same for both protocols, the decision was made to base our sample size solely on our primary outcome.
Randomization
Patients were randomly divided into 2 equal-sized groups using the simple-randomization opaque sealed-envelope technique.6,10 On obtaining verbal consent for study participation, a research assistant opened an envelope containing the group allocation and then notified the surgical team of group assignment. Patients were randomized to either the PRiSM group or the Traditional group.
Intervention
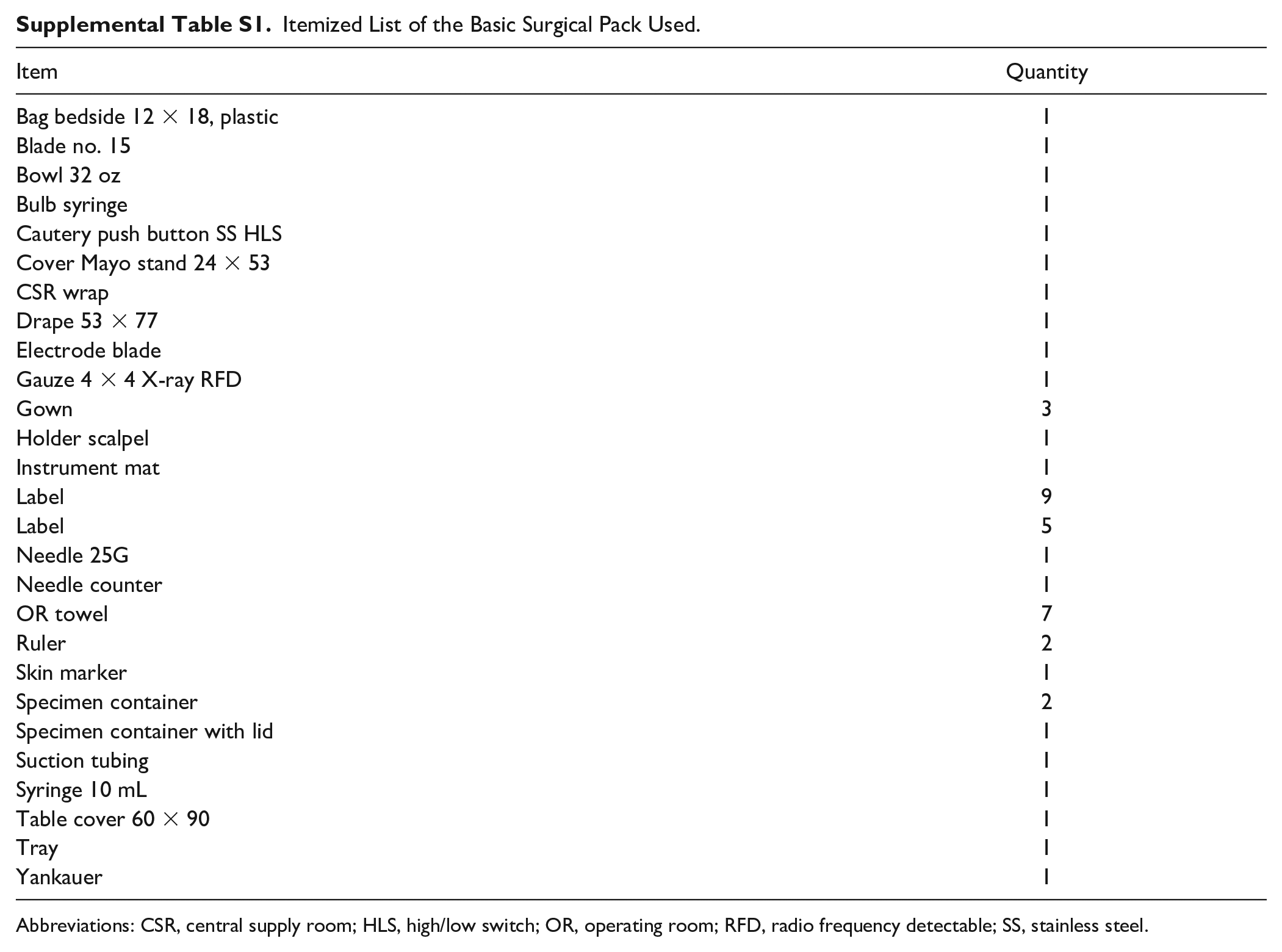
Patients randomized to the Traditional protocol had procedures performed using the commonly employed surgical setup at the surgery center. This includes using a “Hand and Foot Set” (Figure 1A), a basic OR pack (Supplemental Table S1), and an additional ¾ sheet, extremity drape, and pack of blue OR towels (Figure 1B). Patients were positioned with blankets, and the operative limb was placed on Bone Foam. Surgical trainees (residents and fellows) were present and scrubbed for both protocols. Standard gowns and gloves were used. The mini c-arm, if necessary for the procedure, was draped with a mini c-arm drape.

(A) The “Hand and Foot Set” utilized for the Traditional group. (B) The surgical pack, draping (including the extra ¾ drape), and towels used for the Traditional protocol.
Patients randomized to the PRiSM protocol used a streamlined tray (“Excision Kit”; Figure 2A), a basic OR pack, an extremity drape, and a conscious effort to use fewer positioning blankets (Figure 2B). The operative limb was placed on Bone Foam. Surgical gowns, gloves, and the mini c-arm drape were used as needed, identical to the Traditional protocol.

(A) The “Excision Kit” utilized for the PRiSM group. (B) The surgical pack and extremity drape utilized for the PRiSM protocol. PRiSM, Program for Research in Sustainable Medicine.
Outcome Measures
The carbon footprint for each case was determined by summing the estimated kilograms of CO2 equivalents generated by waste, instrument sterilization, and laundry. Only standard trash was included in our calculations as no red bag waste was generated. The standard trash and laundry were weighed using a hand-held suspension scale at the end of every case. Instrument sterilization emissions were estimated using information made available by facilities management at our surgery center.
To estimate GHG emissions of the standard waste generated in the OR, we used production emissions factors for average plastics. The vast majority of standard waste was composed of disposable textiles, blue wrap, latex, and plastic tubing and basins, which represent a combination of low-density polyethylene, high-density polyethylene, polypropylene, and polyethylene terephthalate.15,21 Because a small proportion of waste was not composed of these materials, we used the mixed plastics emissions factor with a 10% modifier (3.179 kg CO2e per kg of waste) as per the methodology used by MacNeill et al. 15 The modified average plastics emissions factor was multiplied by the standard trash weight to estimate the waste-related emissions of each case.
To estimate GHG emissions associated with instrument processing, we used information provided by the central processing and facilities management team. At our institution, the Excision Kit (PRiSM protocol) has 38 instruments, whereas the Hand and Foot Set (Traditional protocol) has 106. Instruments are first run through a washer; a typical wash cycle runs for 1 hour and uses 6.5 kWh of energy. Instruments then undergo steam sterilization, which uses 12.4 kWh of energy and for a cycle lasting 1 hour 7 minutes. At our facility, 24 Excision Kits (PRiSM tray) and 9 Hand and Foot Sets (Traditional tray) can be washed per cycle. We assumed that wash and sterilization cycles were run at capacity. The US Environmental Protection Agency (EPA) conversion factor of 0.433 kg CO2e per 1 kWh of electricity was used to estimate energy-associated emissions. 28
To estimate GHG emissions associated with laundry generated, we based our calculations on those used by Vozzola et al, 30 who reported that typical energy consumption at an industrial laundry facility was 6750 MJ per 1000 kg of laundered textiles, with 85% of energy used from natural gas and 15% from electricity. The US EPA conversion factors of 0.433 kg CO2e per kWh and 5.3 kg CO2e per therm of natural gas were used to estimate laundry-related emissions for each case.
Patient Outcomes
Three months after the conclusion of the study, patient charts were reviewed for incidence of SSI.
Statistical Analysis
Statistical analyses were executed using SPSS version 27. Frequencies and means were calculated for all categorical and continuous variables, respectively. Two-sided independent sample Student t tests or Mann Whitney U tests were used to compare continuous variables across the PRiSM and Traditional groups. Two-sided Pearson chi-square or Fisher exact tests were used to compare categorical variables between groups. Significance was set at α = 0.05.
Results
Baseline Characteristics
Baseline characteristics of patients and procedures were comparable in each group and are shown in Table 1.
Patient and Procedure Characteristics.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; PRiSM, Program for Research in Sustainable Medicine.
Primary Outcome: Carbon Footprint
The total estimated carbon footprint of PRiSM cases was 65.3 kg CO2e less than that of Traditional cases. Waste-related emissions were responsible for the greatest proportion of the carbon footprint for both groups (Figure 3).

Total kilograms of CO2e generated by the PRiSM group and the Traditional group. PRiSM, Program for Research in Sustainable Medicine.
On average, PRiSM cases had a smaller carbon footprint than Traditional cases (17.3 kg CO2e [SD = 3.2] vs 20.6 kg CO2e [SD = 2.0], P < .001) (Figure 4). The PRiSM protocol reduced the carbon footprint for the included cases by an estimated 3.3 kg CO2e or 16% compared to the Traditional protocol.
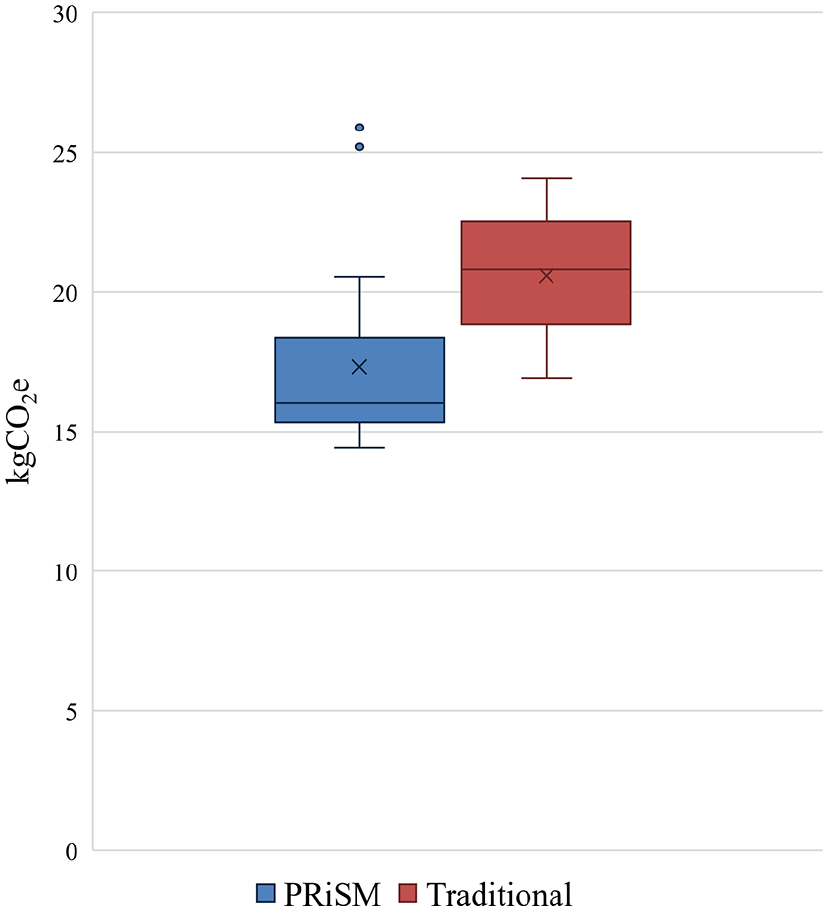
Distribution of CO2e generated by PRiSM and Traditional cases. The whiskers represent the threshold for outliers and are calculated as the boundary of the interquartile range ± 1.5 times the interquartile range. The circles indicate outliers. The “x” represents the mean, and the horizontal line represents the median. PRiSM, Program for Research in Sustainable Medicine.
The average estimated waste-associated greenhouse gas emissions from PRiSM cases were significantly less than for Traditional cases (16.0 kg CO2e [SD = 2.7] vs 18.4 kg CO2e [SD = 1.8], P = .002) (Table 2). No PRiSM cases required conversion to the Hand and Foot Set. The modeled instrument processing–related emissions were 0.34 kg CO2e for PRiSM cases using the Excision Kit and 0.91 kg CO2e for Traditional cases using the Hand and Foot Set, representing a 63% emissions reduction associated with the PRiSM protocol. Average estimated laundry-related emissions for PRiSM cases and Traditional cases (1 kg CO2e [SD = 0.89] vs 1.3 kg CO2e [SD = 0.97]) were statistically indistinguishable (P = .4).
Carbon Footprint (kg CO2e) of Minor Foot and Ankle Procedures Performed Using the PRiSM Protocol vs Traditional Protocol. a

Abbreviation: PRiSM, Program for Research in Sustainable Medicine.
Data are shown as mean (SD).
Secondary Outcome: SSIs
Two SSIs occurred: one in a patient randomized to the Traditional protocol and the other in a patient randomized to the PRiSM protocol. Infections were superficial and resolved within a few days with a course of oral antibiotics.
Discussion
By championing change in the OR, orthopaedic surgeons can help mitigate the negative environmental effects of surgery. 16 With hundreds of foot and ankle surgeries performed each year at our institution, even minor reductions in the carbon footprint of these procedures can have an impact. In this randomized controlled trial, we found a 16% reduction in the environmental impact of foot and ankle surgery when utilizing the PRiSM protocol vs the Traditional protocol at our ambulatory surgery center. We found that the environmental impact of these cases was dominated by waste-related emissions, indicating that even small reductions in the use of predominantly plastic disposables can have an important impact on mitigating the carbon footprint of the OR.
On average, when using the Traditional protocol for foot and ankle surgery, one procedure generated 20.6 kg CO2e. These emissions are equivalent to those generated by driving 52.8 miles in an average gasoline-powered vehicle or the energy required to charge 2506 smartphones. Sequestering this amount of carbon from the atmosphere takes roughly 9 acres of forest one day. Importantly, the majority of surgical drapes, gowns, and disposable supplies are made from polypropylene and other plastics, for which the manufacturing has a substantial environmental impact. 21 Certain surgical pack suppliers offer environmentally preferred options, including natural OR towels that do not require dyes or bleaching, drapes and trays made from sustainably sourced wood pulp, and pigment-free plastic bowls and basins. 17 Currently, our basic pack only includes the sustainable bowl and tray options. Studies have also shown that reusable gowns and drapes are noninferior clinically and prevent SSIs as well as disposable alternatives.2,16,22 Prior life cycle impact assessments exploring reusable vs disposable instruments and textiles have suggested that minimizing waste and sterilization can significantly reduce the estimated detrimental effects on human health caused by the associated emissions.13,20,26,29,30
Importantly, the changes required by the PRiSM protocol were easy to implement. We specifically chose adaptations that could be immediately adopted by the surgical team and would not require any substantial deviation from the typical workflow. As a result, the PRiSM protocol was readily embraced by the OR staff. Although not explicitly studied, OR and central-processing staff also commented on the time-savings associated with simpler patient set-up and utilizing the smaller instrument set.
Although this study is the first of its kind in foot and ankle surgery, this topic has been explored by other groups and in other orthopaedic subspecialties.1,11,13,19,24,26,27,31 Kodumuri and colleagues in the United Kingdom studied the impact of a “Lean and Green model” for carpel tunnel decompression that also used smaller instrument trays, smaller drapes, and fewer disposables. 11 Over a 15-month period, they collected data on 103 cases performed using the Lean and Green model and found an 80% reduction (28.8 kg CO2e to 6.6 kg CO2e) in CO2e emissions and a clinical waste reduction of 65%. Of note, constraining the study to one procedure type allowed the authors to consistently implement more dramatic adaptations—for example, their protocol did not use any single-use plastic dishes, suction tubing, or plastic sheets. Taken together, our studies demonstrate that the standard approach to certain orthopaedic cases can be safely shifted toward a protocol that minimizes environmental impact.
We found that minimizing the number of instruments used in the PRiSM group resulted in a substantial (63%) decrease in sterilization-associated emissions. It was somewhat surprising that instrument sterilization was not the largest component of the carbon footprint. Prior studies performing life cycle analyses of single-use vs disposable devices for specific procedures have found instrument processing to be one of the largest contributors of GHG emissions.13,24,31 One possible explanation for this discrepancy is that our ambulatory surgery center uses a small steam generator compared to the more energy-intensive equipment commonly used by larger centers. Furthermore, we assumed maximum loading capacity, which is often not the reality and has been shown to greatly impact the carbon footprint of instrument sterilization. 19 It is also worth noting that for an average reusable instrument, it is more sustainable and cost effective to include the instrument in a tray rather than open an individually wrapped instrument.18,19
Although not our primary outcome for this study, cost is an important consideration for implementing environmental sustainability initiatives. The cost of a surgical drape generally ranges between $1.25 and $5.35; a recent study found that eliminating the extra down sheet, as we did for the PRiSM protocol, could save $17,446 annually if implemented across the department of orthopaedic surgery. 3 Laundry at our institution is paid for by the pound, and similar, if not greater, cost savings can be projected by minimizing laundry whenever appropriate. Furthermore, the aforementioned time saved on the part of OR and CPD staff constitutes another opportunity for cost savings. Sherman et al 24 found that reprocessing labor dominated per-use costs of a reusable laryngoscope when performing a life cycle costing assessment. Moreover, Kodumuri et al 11 found their Lean and Green model for carpel tunnel release reduced case time by 30 minutes, increasing OR productivity by 2 patients for a 210-minute operative session. These time savings were driven by decreased time spent draping and counting instruments before and after the procedure, similar to what we experienced with the PRiSM protocol. In short, these findings suggest that using a slimmed down surgical draping and positioning setup with fewer instruments can reduce cost and improve efficiency.
The impact of recycling was not included in this study. At our facility, recycling bins are present in a room adjacent to the ORs. Some OR staff reported recycling extra plastic specimen containers, for example, but efforts at our center are inconsistent. Prior studies examining the impact of recycling in the hospital setting have encouraged the practice, but noted that recycling can be quite energy intensive when items must first be sterilized, transported, deconstructed, and ultimately remolded into something new. 24 This is an area of potential investigation and improvement.
This study has several limitations. First, direct measurement of the carbon footprint for a procedure is not yet possible. The methods used assumptions and thus produced estimates. Second, our study captured only a small portion of the actual procedure carbon footprint. For example, emissions sources, such as the heating, ventilation, and air conditioning system and OR lights, which are known to have a large carbon footprint that can vary depending on the energy source, were not included. Third, the surgical team was not masked to the group assignment, which could have introduced bias with regard to positioning (eg, blanket use) and equipment use. That said, a conscious effort was made to use the typical setup and positioning that has been used for years at this facility for the Traditional procedures. Fourth, our study was underpowered to detect a significant difference in rate of SSI between the 2 protocols. Finally, we acknowledge that not all surgeons use the same “Traditional” protocol as described here. However, we feel that this study is helpful in that it underscores how small, relatively simple, concerted efforts can together meaningfully reduce the environmental impact of orthopaedic surgery. We also believe that other surgeons can find many additional opportunities for waste reduction in the OR.
Conclusion
In summary, we found a small but statistically significant reduction in the environmental impact of foot and ankle surgery when using the PRiSM vs our Traditional ambulatory surgery center protocol. The environmental impact of these cases was dominated by waste-related emissions, indicating that even small reductions in the use of predominantly plastic disposables can have a meaningful impact on mitigating the carbon footprint of the OR. Although only a small subset of foot and ankle procedures were included, we believe that the PRiSM protocol can be safely implemented for many other procedures, including those outside the field of foot and ankle surgery. The changes outlined in the PRiSM protocol are easy to make and are often within the surgeon’s control. Orthopaedic surgeons should think critically about what components of their surgical setup are truly necessary for patient care, as even minor changes in instrument, product, and laundry utilization can reduce greenhouse gas emissions.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241238231 – Supplemental material for Carbon Footprint of Minor Foot and Ankle Surgery: A Randomized Controlled Trial
Supplemental material, sj-pdf-1-fao-10.1177_24730114241238231 for Carbon Footprint of Minor Foot and Ankle Surgery: A Randomized Controlled Trial by Emily B. Parker, Eric M. Bluman, Christopher P. Chiodo, Elizabeth A. Martin and Jeremy T. Smith in Foot & Ankle Orthopaedics
Footnotes
Appendix
Itemized List of the Basic Surgical Pack Used.
| Item | Quantity |
|---|---|
| Bag bedside 12 × 18, plastic | 1 |
| Blade no. 15 | 1 |
| Bowl 32 oz | 1 |
| Bulb syringe | 1 |
| Cautery push button SS HLS | 1 |
| Cover Mayo stand 24 × 53 | 1 |
| CSR wrap | 1 |
| Drape 53 × 77 | 1 |
| Electrode blade | 1 |
| Gauze 4 × 4 X-ray RFD | 1 |
| Gown | 3 |
| Holder scalpel | 1 |
| Instrument mat | 1 |
| Label | 9 |
| Label | 5 |
| Needle 25G | 1 |
| Needle counter | 1 |
| OR towel | 7 |
| Ruler | 2 |
| Skin marker | 1 |
| Specimen container | 2 |
| Specimen container with lid | 1 |
| Suction tubing | 1 |
| Syringe 10 mL | 1 |
| Table cover 60 × 90 | 1 |
| Tray | 1 |
| Yankauer | 1 |
Abbreviations: CSR, central supply room; HLS, high/low switch; OR, operating room; RFD, radio frequency detectable; SS, stainless steel.
Ethics Approval
Ethical approval for this study was obtained from the Mass General Brigham IRB (Protocol no. 2023P000576).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.