
Abstract
Background:
Ankle fractures are a frequent injury in the adult population and a quarter of all ankle fractures are classified as unstable, requiring surgical intervention. Plate-and-screw construct is the traditionally used fixation method for fibula fractures. The use of an intramedullary nail is an alternative fixation method, with current literature supporting very low complication rates and hardware removal surgeries. The purpose of this study was to evaluate the outcomes, including complication rates and implant removal rates, using a fibula nail with both proximal and distal fixation capabilities by an experienced surgeon.
Methods:
We retrospectively reviewed 203 consecutive fibula nail cases from a single surgeon using a mini-open technique for anatomic reduction. Demographic, operative, clinical, and radiographic outcome data were analyzed, specifically examining complication rates and need for implant removal.
Results:
The average follow-up was 18.8 months (6-54 months). All fractures healed. We identified 2 cases of superficial wound infection, 1 superficial peroneal nerve irritation, and 1 case of implant removal. In the first 110 cases, 2 fractures were converted to a plate intraoperatively prior to a technique modification which has prevented this occurrence. No deep infection, delayed union, or nonunion occurred.
Conclusion:
Our data support that fibula nails with proximal and distal locking capabilities offer an alternative to plating with the potential for lower complication rates and lower need for implant removal.
Level of evidence:
Level IV, case series.
Keywords
Introduction
Plate-and-screw fixation for fibular fractures constitutes an acceptable and effective construct, Vanderkarr et al 17 reported that between January 2016 and October 2021, ankle fractures affected 0.14% of the population, with 23.4% of these fractures requiring surgical intervention. Approximately 7% of the patients who underwent surgical management of an ankle fracture during this time sustained an infection and 5.6% required reoperation with related morbidity and cost.13,17
Traditionally, operative treatment of unstable ankle fractures has been open reduction and internal fixation (ORIF).1,2,6,7 ORIF is performed to reduce the fracture anatomically under direct visualization, and plate fixation is the favored method to treat fibula fractures.1,3,6 However, plate fixation may require extensile incisions through the skin and overlying soft tissue, elevation and stripping of adjacent musculature, periosteum, and blood supply.1,3,16 Extensile incisions potentially require delayed surgical intervention because of soft tissue swelling, which increases the risk of wound healing complications. 7 Larger incisions may also increase postoperative pain and therefore need for more narcotics, increased postoperative swelling, and larger cosmetic scarring. 8 Additionally, the presence of a plate on the surface of the subcutaneous distal fibula may cause irritation and require removal, with an average removal rate reported at approximately 34.7% (12%-95.5%). 15
In general, less invasive surgery with more stable constructs may lead to decreased complications and less reoperations. Fibula nailing allows a minimally invasive surgical approach that can be used for unstable ankle fractures.1,3,6,16 Intramedullary nails can potentially allow closed fracture reduction and/or preferably a mini-open incision to ensure anatomic reduction. The less invasive approach results in less soft tissue disruption, thus potentially reducing soft tissue complications and infections.1,3,15 The incisions necessary for the fibula nail technique are, on average, 80% smaller than those required for plate techniques. 16 This technique leads to minimal complication rates and reduced need for second surgeries because of its minimally invasive nature.3-6,15
Existing literature supports positive outcomes and lower complication rates with the nail technique. 11 These advantages were previously reported in our original series of 110 consecutive fibula nails. This study provides extended follow-up data on the initial 110 cases, now including an expanded cohort of 90 patients, further affirming the safety and effectiveness of this technique as an alternative to traditional plate-and-screw fixation.
The aim of this study was to describe perioperative complications in ankle fracture patients consecutively treated via fibula nail fixation by a single experienced surgeon.
Materials and Methods
Under institutional review board approval (IRB no. 1480559-4), 215 patients were screened for eligibility into the retrospective study between 2018 and 2021. Of the 215 patients, 12 patients were excluded for the following reasons: loss to follow-up postoperatively, open fracture, <18 years of age, and/or the injury included a concurrent lower extremity fracture. In total, 203 fractures treated with a fibula nail were included in our retrospective analysis. Fractures were classified in accordance with the Weber classification. 12 All patients were surgically treated with the Arthrex FibuLock fibula nail (Arthrex, Naples, FL).
Data Collection
Data were collected from medical charts and imaging to determine demographic information, imaging, and perioperative variables such as incision size, follow-up course, and complications including wound problems, infections, implant irritation, and removal.
Preoperatively, anteroposterior, lateral, and mortise weightbearing radiographs were obtained in all patients. Stress radiographs and/or computed tomography (CT) scans were also frequently based on the fracture type or further need to assess for instability of the ankle fracture. The following parameters were examined to help assess unstable ankle fractures: medial clear space widening, lateral subluxation of the talus, diastasis of the syndesmosis, presence of additional fractures, dislocation, obvious increased tibial or fibular widening, and stress view diastasis. The CT scan was also used to identify the fracture pattern to aid in preoperative planning. Stable ankle fractures were treated nonoperatively and are not included in the following cohort of patients.
All fibula fracture patterns were deemed to be appropriately treated with a fibula nail as it is the preferred treatment method for the senior author’s ankle fracture surgical management protocol. The senior author performs arthroscopy with a NanoScope (Arthrex) for all ankle fractures, allowing him to identify, document, and potentially treat intraarticular pathology, which has been reported in excess of 80% in the literature.9,14 A 2- to 3-cm mini-open incision is used to obtain anatomy correction prior to nail insertion. Syndesmotic alignment and stability are assessed on preoperative radiographs, CT scan, and intraoperatively using nano-arthroscopy and direct visualization and manipulation. We do not rely on fluoroscopic imaging alone to determine syndesmotic alignment or stability.
Anterior inferior tibiofibular ligament injury was observed 100% of his unstable ankle fracture arthroscopies, and therefore by definition, some degree of syndesmotic injury in unstable ankle fractures; therefore, unless convinced that there is absolutely no instability, the procedure always involves stabilizing the syndesmosis. The reduction quality was assessed intraoperatively by the senior author using direct visualization of the reduction through the mini-incision as well as fluoroscopy. Reduction quality parameters used to assess the reduction were fibular length (dime sign and talocrural angle), direct visualization of near anatomic reduction, lateral view fibular position in relation to the tibial plafond, the tibial/fibular clear space, medial clear space (MCS) on manual stress test, and use of the Cotton test with Freer. Weightbearing radiographs were performed at 6-week, 10-week, 16-week, 5- or 6-month, and 1-year follow-up visits.
Statistical Analysis
All collected data were analyzed by a commercially available statistical software package (SPSS version 12.0.1 Apache Software Foundation) using descriptive statistics. Continuous data were summarized as mean ± SD and range. Categorical data were reported as numbers of subjects and percentages.
Results
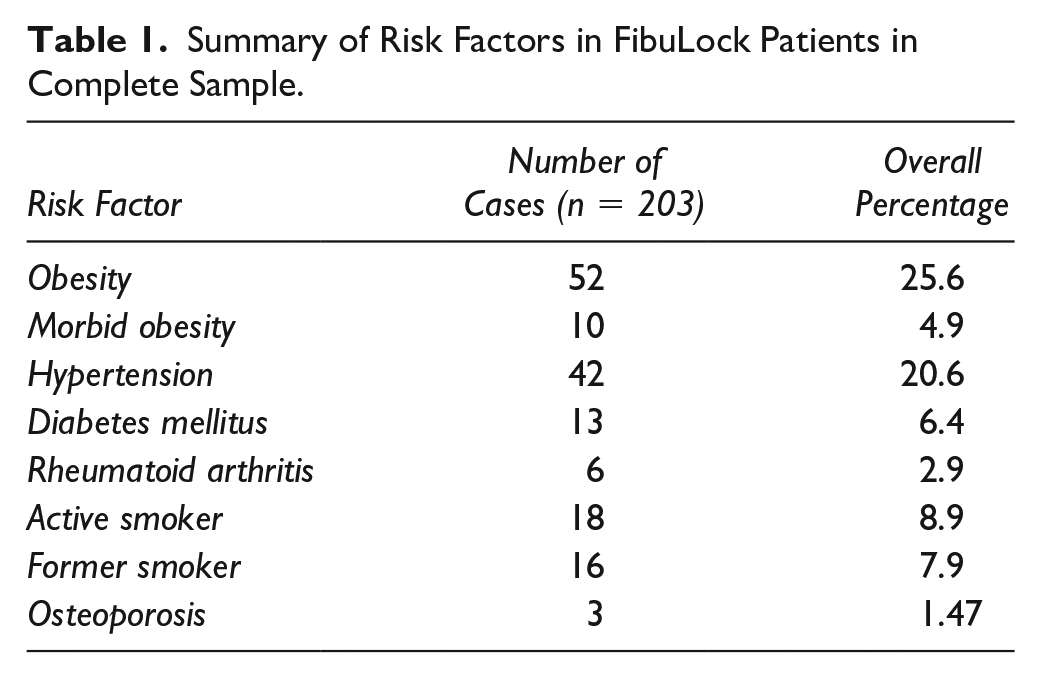
Between 2018 and 2020, a total of 216 patients were screened for eligibility into the retrospective study. Of the 216 patients, 12 patients were excluded for the following reasons: lost to follow-up postoperatively, surgery did not use the intramedullary nail, the fracture was open or comminuted, <18 years of age, and/or a concurrent pilon fracture. In total, 203 fractures were treated with a fibula nail and were included in our retrospective analysis. The average age of the cohort was 47.3 years (range, 29-82) and the average body mass index was 28 (range, 22-34). The gender distribution of the sample included 133 (65.5%) females and 71 (34.9%) males. Medical comorbidities are listed in Table 1. The average follow-up was 18.5 months.
Summary of Risk Factors in FibuLock Patients in Complete Sample.
Weightbearing radiographs were preoperatively obtained in all patients able to tolerate the examination unless prior imaging revealed obvious instability requiring surgery. Eighty-two patients (40.4%) underwent a stress radiograph, and 189 patients (93.1%) received a CT scan. Fifty-six patients (28.6%) had a fibula fracture only, 27 (13.3%) had a bimalleolar fracture, 65 (32%) trimalleolar, and 53 (26.1%) fibula and posterior malleolar fractures. The patterns and complexities of fractures varied among the 203 patients and are displayed in Table 2.
Summary of Fracture Type in Patient Population.

The average number of days from date of injury to surgery was 8.0 (SD ± 5.6). The reduction mode also varied among patients and was dependent on the complexity of the fracture pattern. A total of 191 fractures were reduced through a mini-open incision; 10 were reduced closed. Depending on the location of the fracture and the equipment required, additional incisions were made in order to place a screw in lieu of flexible fixation. The additional incisions when placing a screw was less than 2 mm. The mini-open incision had an average size of 3.5 cm, 75.2% had an incision of less than 3 cm (Figure 1). Other procedures performed during the surgical time, including syndesmotic repair, deltoid ligament repair, and arthroscopy, are shown in Table 3.

Lateral approach of the ankle. Incision size for open reduction of fibula fracture.
Summary of Concurrent Procedures.

All fractures were reduced anatomically intraoperatively. The majority of the fractures (95%) did not experience diastasis at the fracture site. In 5% of the fractures, we observed subtle fracture gapping generally less than 1 mm following reduction clamp removal. We propose that this is due to a mismatch in nail and fibula morphology. These fractures did not show any difference in the postoperative course compared to fractures that did not gap aside from those patients developing callus on postoperative radiographs.
We had the following intraoperative complications, a laceration of the superficial peroneal nerve, and 2 severely comminuted fractures converted to plate in our initial 110 cases. In the additional cohort of patients, no intraoperative complications were noted, and no cases were converted to plate following adoption of a plate-assisted nail technique. This technique involves a mini-fragment plate secured to obtain and hold comminuted, fragile, reductions, which then facilitates nail placement. The plate is secured with 6-mm unicortical locking screws and are frequently left in place.
Most patients were allowed to begin weightbearing at 2 weeks in a boot with protocol, allowing 10% increase in body weight every 3 days. Patients with the following were not permitted to begin weightbearing until 6 weeks: coexisting medial malleolar fracture, trimalleolar fracture, deltoid rupture, grossly unstable and dislocated syndesmotic injury, diabetics, and neuropathic patients. The average time to start partial weightbearing in a boot was 4.9 weeks (SD 2.1). The average time for patients to be fully weightbearing in the boot was 9.3 weeks (SD 2.6), and time to transition from weightbearing in a boot to use of an ankle brace was 9.7 weeks (SD 2.4).
Healing was assessed using postoperative radiographs and radiographic evidence of a healed fracture occurred at a mean of 6.3 weeks ± 1.1 (Figure 2). There were no postoperative infections, 2 cases of noninfected superficial epidermolysis over the fibula incision site, and no cases of delayed union or nonunion. One patient required the removal of a proud nail 6 months postoperatively. This was an iatrogenic surgeon error contributed by the atypical use of a mini c-arm rather than the standard large c-arm.

Radiographs of the right ankle. Upper row: preoperative radiographs of the right ankle. From left to right: anteroposterior, mortise, and lateral projections. Unstable ankle fracture. Lower row: 6-month postoperative radiographs of the right ankle. From left to right: anteroposterior, mortise, and lateral projections. Use of fibular nail fixation with proximal talon and 2 tightropes over the syndesmosis.
Discussion
In the series presented here, the fibula nail resulted in anatomic reduction and complete healing in all patients; we had no incidents of delayed or malunion, and postoperatively, no loss of reduction occurred in any patients. Two cases required conversion to an open plating procedure. One implant required removal secondary to iatrogenic surgical error leaving the nail proud. Our findings are consistent with Asloum and colleagues, 1 who compared plate and nail surgical interventions. Their fibula nailing group resulted in 100% union and only 7% postoperative complications, compared with their plate fixation group, which resulted in 94% union and 56% postoperative complications.
A systematic review of 1710 patients also compared rates of nonunion, implant removal, and other complications in intramedullary fixation vs plate fixation. Their findings showed a statistically significant difference favoring intramedullary fixation, with only 1.7% nonunion in intramedullary fixation, compared with 13.7% in plate fixation. 16
Plate fixation requires larger incisions with a reported mean of 8 cm. 8 In our technique, we performed open reduction with an average incision of 3.5 cm, and 75.2% of our patients had an incision of less than 3 cm. The use of an open technique is important as it allows for visual confirmation of anatomic reduction. We feel that minimizing the size of the incision to a mini-open one of 4 cm or less decreases postoperative pain and swelling, which may lead to faster restoration of comfort, motion, and strength while also decreasing the potential risk of wound complications and infections. 8 Furthermore, the reduction in the surgical footprint and decreased soft tissue stripping and periosteal disruption may lead to faster healing.
These advantages are exponentially more important in high-risk patients such as diabetics or current and prior tobacco consumers who may have increased risks of wound complications.3-6,17 This study supports current literature that suggests that the use of a fibula nail may be a better alternative than the traditional plate fixation currently used especially for select patients. 10 We chose to perform arthroscopy in 170 (84%) of our patients. Malleolar fractures commonly have concomitant chondral or osteochondral defects, many of which are missed on radiographs and CT scans.9,14 If missed, they may result in decreased clinical outcomes. Thus, the senior author prefers nano-arthroscopic evaluation of the joint at the time of fracture stabilization using 2 portals. In these cases, the nano-scope is preferred as it leaves a smaller surgical footprint than a regular scope and eliminates any time or equipment issues because of its plug-and-play capabilities.
This statement is consistent with our arthroscopic findings, where a considerable number of our patients had intraarticular pathology (Table 4). When arthroscopy was employed, commonly identified injuries included unstable chondral injuries requiring chondroplasty, removal of loose bodies, and most frequently a torn anterior inferior tibiofibular ligament requiring debridement along with removal from the anterolateral joint to prevent potential impingement.
Summary of Arthroscopic Procedures.

The existing literature has limited data on intramedullary fibula fixation and much of the earlier reported literature on other intramedullary fixation techniques revealed issues with loss of reduction because of closed reduction techniques and lack of proximal fixation. However, interestingly, fibula nailing still had equivocal results to plating techniques, many even showing improved results when nailing over plating.3,7,8,18 Rush rods, Ender nails, and Knowles pins are earlier intramedullary devices that were effective at aligning the fibula, but did not provide good rotational or axial stability. 4 We believe that a nail that provides both distal and proximal fixation is essential for rotational stability and length control. The proximal fixation feature allows for increased axial and rotational stability of the nail and reduction control. The evolving literature has supported these hypotheses, including our previously published series of 110 consecutive nails that showed 100% union with no loss of reduction postoperatively and a very low complication profile. 11
Although we acknowledge that rates of infection and nonunion with plate-and-screw fixation are relatively low, rates of implant irritation and removal are relatively higher.2,6,18 In a review of 404 surgically plated fibula fractures, 13.4% of patients had implant complications resulting in removal. 2 Another study comparing plate fixation and intramedullary nail fixation performed by the same surgeon had 31.6% of implant complications with plate fixation, 12.5% of these patients underwent a second surgery for removal, compared to 0% implant complications or removal seen in patients who received intramedullary nails. 18 In our results, only 1 case (0.5%) required implant removal for a proud nail, which is in line with the current literature findings. 18
Fibula nails are essentially no-profile devices with significantly lower rates of irritation and removal.4,6,15 Our results demonstrate a very low complication rate, with only 1 case requiring implant removal due to surgeon error. We believe that a fibular nail is a preferred method over plate-and-screw fixation because it provides advantages such as smaller incisions and decreased stripping of the periosteum and blood supply.1,3,16 We suggest that fibula nails with proximal and distal fixation capabilities are superior to prior versions of fibula nails lacking these capabilities.3,16
A limitation of this study was the fact that all patients were treated by a single surgeon, limiting the variances in skill and techniques that may occur with multiple surgeons but also, and importantly, possibly limiting the generalizability of the findings to other surgeons. Retrospective study designs are accompanied by natural study limitations such as not having selection criteria clearly delineated. Single procedure designs without a comparison to an alternative procedure performed by the same surgeon also limits the impact of the findings. Additionally, surgeons with more experience using this technique may have fewer complications due to experience, whereas a surgeon with less experience may see an increase in complications in the outcomes of this surgery.
Conclusion
The results of our study demonstrate that in our hands, a fibula nail was a very good choice for stabilization of fibula fractures, with a low infection and complication rate. The mini-open technique allowed anatomic reduction, high union rates, and compares favorably to published results for plate-and-screw fixation. We believe there will be a paradigm shift in fibular fixation care associated with improved outcomes, lower complication profiles, and think nailing will become a new “gold standard.”
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241230563 – Supplemental material for Use of Fibula Nails With Proximal and Distal Fixation
Supplemental material, sj-pdf-1-fao-10.1177_24730114241230563 for Use of Fibula Nails With Proximal and Distal Fixation by Solangel Rodriguez-Materon, Samantha Trynz, Dino Fanfan, Jorge Fleites, Jorge Gil and Christopher Hodgkins in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Baptist Health South Florida’s Institutional Review Board (IRB1480559).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christopher Hodgkins, MD, reports consulting fees and payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events from Arthrex. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.