
Abstract
Background:
The best treatment strategy for fractures to the posterior malleolus (PM) is still intensively debated. The aim of this systematic review was to compare the patient-rated outcome following open reduction and internal fixation (ORIF) for fractures of the PM to either closed reduction using AP screws (CRIF) or no treatment in bi- or trimalleolar ankle fractures.
Methods:
Systematic literature research (MEDLINE (PubMed), CINAHL, Scopus, Central and EMBASE) according to the PICOS and PRISMA guidelines. Eligible were studies comparing the outcome following ORIF to any other treatment strategy for fractures to the posterior malleolus in isolated bi- or trimalleolar ankle fractures.
Results:
Twelve studies were eligible for a qualitative analysis and 6 for a quantitative analysis. Overall, a considerable heterogeneity among the studies was observed. The most commonly used outcome score was the American Orthopaedic Foot & Ankle Society ankle-hindfoot score (AOFAS). The final follow-up ranged from 12 to 160 months. Four studies compared ORIF to CRIF of the PM. The quantitative analysis revealed significantly better AOFAS scores for ORIF (90.9 vs 83.4 points; P < .001; I2 = 0%). Three studies compared ORIF to untreated PM fragment. The quantitative analysis again revealed superior AOFAS scores for ORIF (92.0 vs 82.5 points; P < .001; I2 = 99%). A similar trend was observed for the Ankle Fracture Scoring System and American Academy of Orthopaedic Surgeons Foot and Ankle Questionnaire scores as well as the quality of reduction.
Conclusion:
Despite a considerable heterogeneity, the data available point to a superior outcome following ORIF for fractures to the PM when compared to CRIF or no treatment.
Introduction
Ankle fractures are common injuries. It is well accepted that the patient-rated outcome correlates with the severity of the fracture.9,15 With the increasing application of computed tomographic (CT) scans, it has been recognized that up to 44% of all ankle fractures involve the posterior malleolus (PM).6,30 The best treatment strategy for fractures to the PM is debated, especially when the fragment size is small. Traditionally, fragments involving more than 25% to 33% of the articular surface in the sagittal plane were considered indications for surgical treatment.25,39 PM fragments <25% to 33% of the articular surface were commonly not addressed. Among all fragment sizes, the treatment indication is considered as highest effect on the stability of the ankle—respectively the tibiofibular joint—which is a widely used argument for open reduction and internal fixation of the PM fragments via the posterolateral approach.
This approach has been challenged by the landmark paper of Gardner et al. 13 Nowadays, fractures to the PM are considered as bony avulsions of the posterior inferior tibial-fibular ligament (PiTFL). Therefore, ORIF of the PM does not only reconstruct the bony anatomy of the tibiotalar and tibiofibular joints but also reduces the fibula in the tibial groove and restores the ligamentous stability of the PITFL.4,12,28 Consequently, an increasing number of authors today recommend ORIF of the PM fragment.5,22,23,44
ORIF of the PM fragment attempts to tease the realignment of the plafond and stabilization of the tibiotalar joint. Furthermore, realignment of the syndesmosis and the distal tibiofibular joint via the PITFL can be attempted.
Despite the above-mentioned advantages of ORIF of the PM fragment, the actual benefit for the patient remains debated. Previous studies have reported inconclusive results,4,10,17,24,41,42 but no study has conducted a systematic, cumulative analysis of the studies available. Therefore, the aim of this systematic review was to compare the patient-rated outcome of ORIF of the PM fragment to either closed reduction and internal fixation (CRIF) AP screws or untreated PM fragments in bi- or trimalleolar ankle fractures involving the posterior malleolus.
Methods
This systematic was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 26 and was a priori registered to PROSPERO.
Search strategy
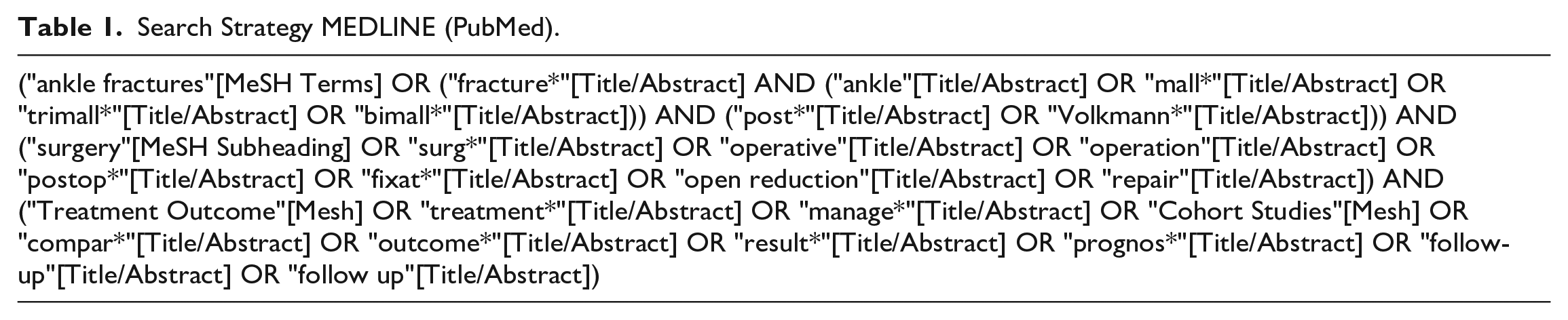
MEDLINE (PubMed), CINAHL, Scopus, Central, and EMBASE were searched for original studies published from inception to the June 30, 2021. A gray literature search for conference proceedings in both Scopus and EMBASE was performed, and all references of the studies included were hand-searched to identify studies that might have been missed by the systematic search. The search strategy was established for MEDLINE (PubMed) and adapted for the other search engines accordingly (Table 1, Supplemental Table 1).
Search Strategy MEDLINE (PubMed).
Eligibility Criteria
The eligibility criteria were designed according to the PICOS criteria 33 and are illustrated in Table 2.
Eligibility Criteria per the PICOS Criteria.
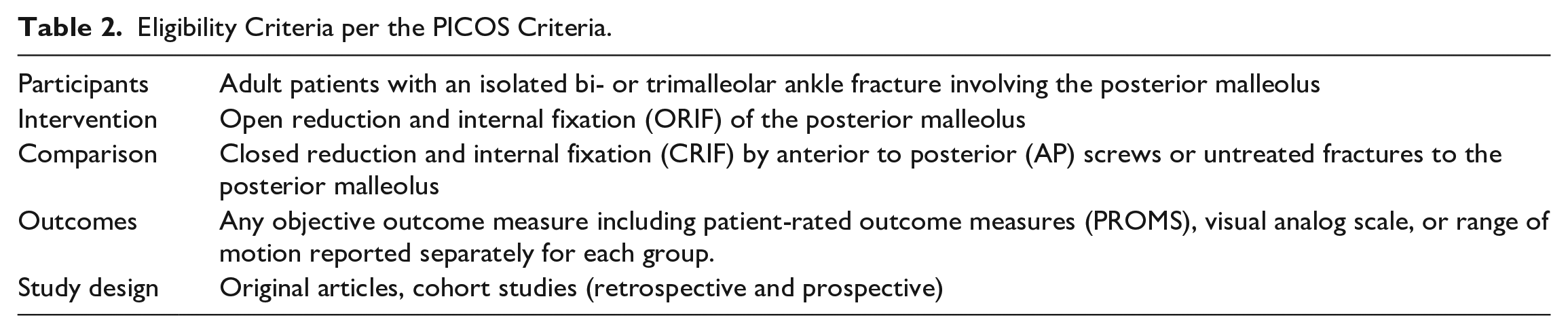
Exclusion criteria were isolated fractures to the PM, fractures other than to the ankle, pilon fracture, missing objective outcome data, and biomechanical or computational studies. Publications were excluded if non-English, non-French, non-German, non-Spanish, or non-Portuguese.
Data Extraction
Each database was searched separately; the data sets were exported to Endnote (version 20.1; Fa. Clarivate) and duplicates were removed. The final data set was exported to Covidence (Melbourne, Australia). Two reviewers independently first screened the title and/or abstracts and then the full texts. Conflicts were resolved by discussion with a third reviewer.
Standardized data extraction sheets were created and completed for each included paper separately. The following data from each included paper were collected: study design, sample size, demographics, fracture details, treatment details, imaging details, quality of reduction, follow-up time, radiographic analysis, and any objective outcome measures as defined above. Objective outcome measures were defined as primary outcome parameters. Further feasible parameters were collected as secondary outcome parameters and included to analysis.
Risk of Bias Assessment
The level of evidence and risk of bias assessment were again performed by 2 reviewers independently. Disagreements were resolved by discussion with a third reviewer. The level of evidence was assessed by the level of evidence rating system introduced by Wright et al. 45 The risk of bias assessment was performed using the Methodological Index for Non-Randomized Studies (MINORS). The MINORS Tool is regularly used for randomized and nonrandomized studies and scores between 0 and 24 points.36,45
Data Synthesis and Analysis
The retrieved data sheets were analyzed for comparable data and finally merged to a final database. In case 3 or more studies revealed a sufficient comparability (inclusion criteria, fracture details, treatment details, outcome parameters, follow-up), a meta-analysis was conducted. In case of insufficient comparability but comparable treatment groups and outcome parameters, a quantitative analysis was performed to illustrate the current outcome trend 43 using the Cochrane RevMan 5.4.1 (random effects method [inverse variance]; effect measure: mean difference). 32 Shi et al 35 data had to be converted to SD; this was done as described by Wan et al. 43 Finally, data were presented with mean values ± SD. The I2 test was used to assess the heterogeneity within the model. The following classification was used to describe the statistical heterogeneity: 11 0% to 40% = not important heterogeneity; 30% to 60% = moderate heterogeneity; 50% to 90% = substantial heterogeneity; 75% to 100% = considerable heterogeneity. Furthermore, if possible, the quality of reduction, the frequency of additional transsyndesmotic fixation, and the degree of osteoarthritis per the different PM fragment treatment strategies were analyzed.
Finally, if feasible in the quantitative or qualitative analysis, the calculated mean differences that are of clinical importance will be presented as the minimal clinically important difference (MCID) for the PROMs in ankle fractures.
Results
The study selection process is outlined in Figure 1. The herein applied search strategy resulted in 7942 studies after removal of duplicates. A total of 370 studies were full text screened. Mertens et al 24 and Marques Ribeiro et al 22 were contacted and provided more detailed data or data analysis, which were used in the following. Mean values of Saygılı et al 34 were calculated manually as they provided data for each patient separately. Xu et el 46 were contacted but no information about the operative technique could be received. Twelve studies were eligible and were included for qualitative synthesis (Tables 3 and 4). Seven studies contained data on the PM fragments >25% and 4 studies on PM fragments <25% (Table 4, Supplemental Figure 1). Although the way the PMF size was assessed differed considerably, only one study by De Vries et al reported on significant group differences, whereas O’Connor et al did not report a significant difference of the PMF size within the different groups (P = .9). All other studies (if judged based on the percentage values presented), apparently included similar sized PMFs in their treatment groups (Table 4). Finally, 6 studies were included in a quantitative analysis.
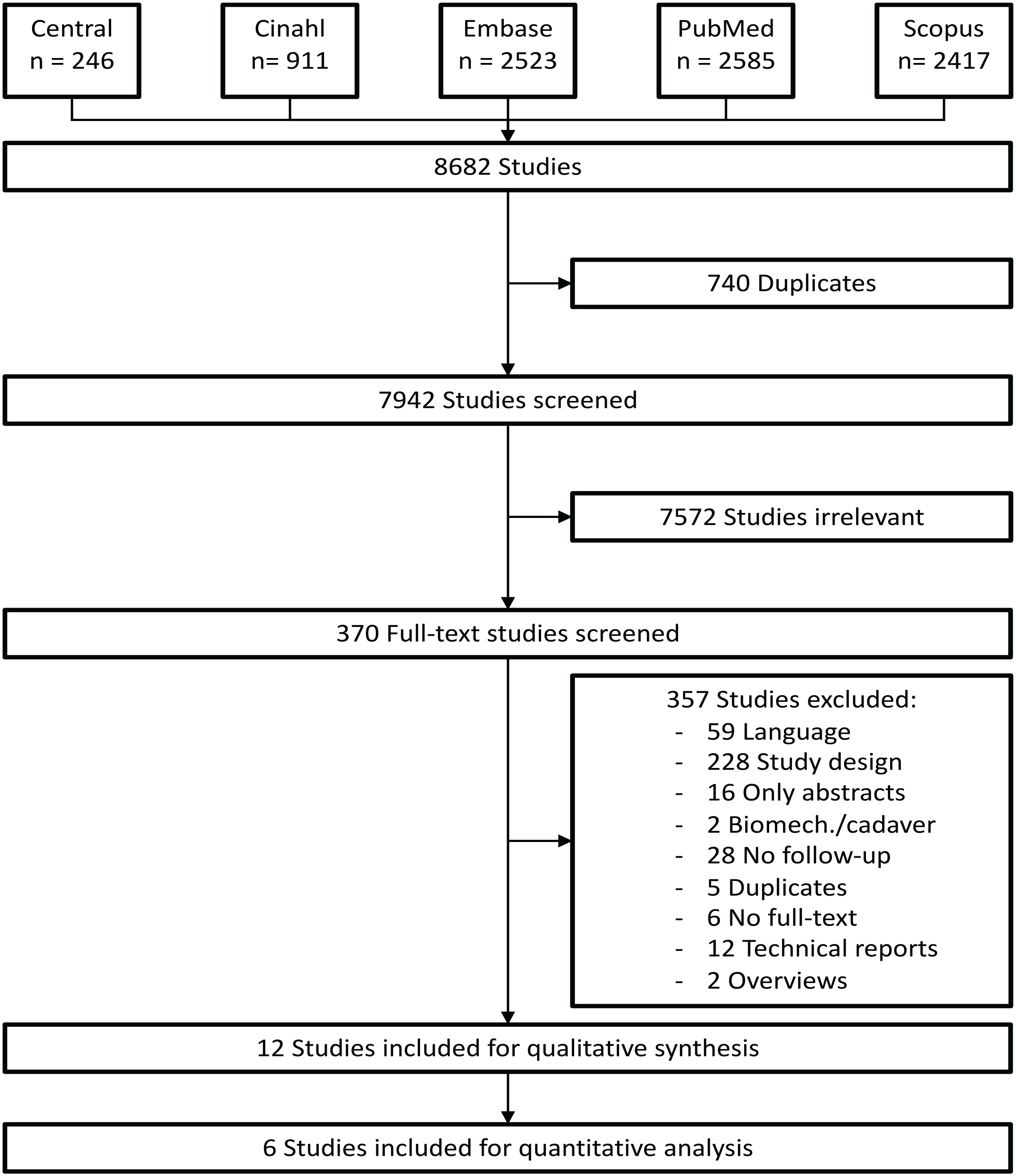
Flow chart following the PRISMA guidelines. 5 different scientific data bases were searched and 8682 studies found. Finally, 12 studies were included for qualitative synthesis and 6 studies for quantitative analysis.
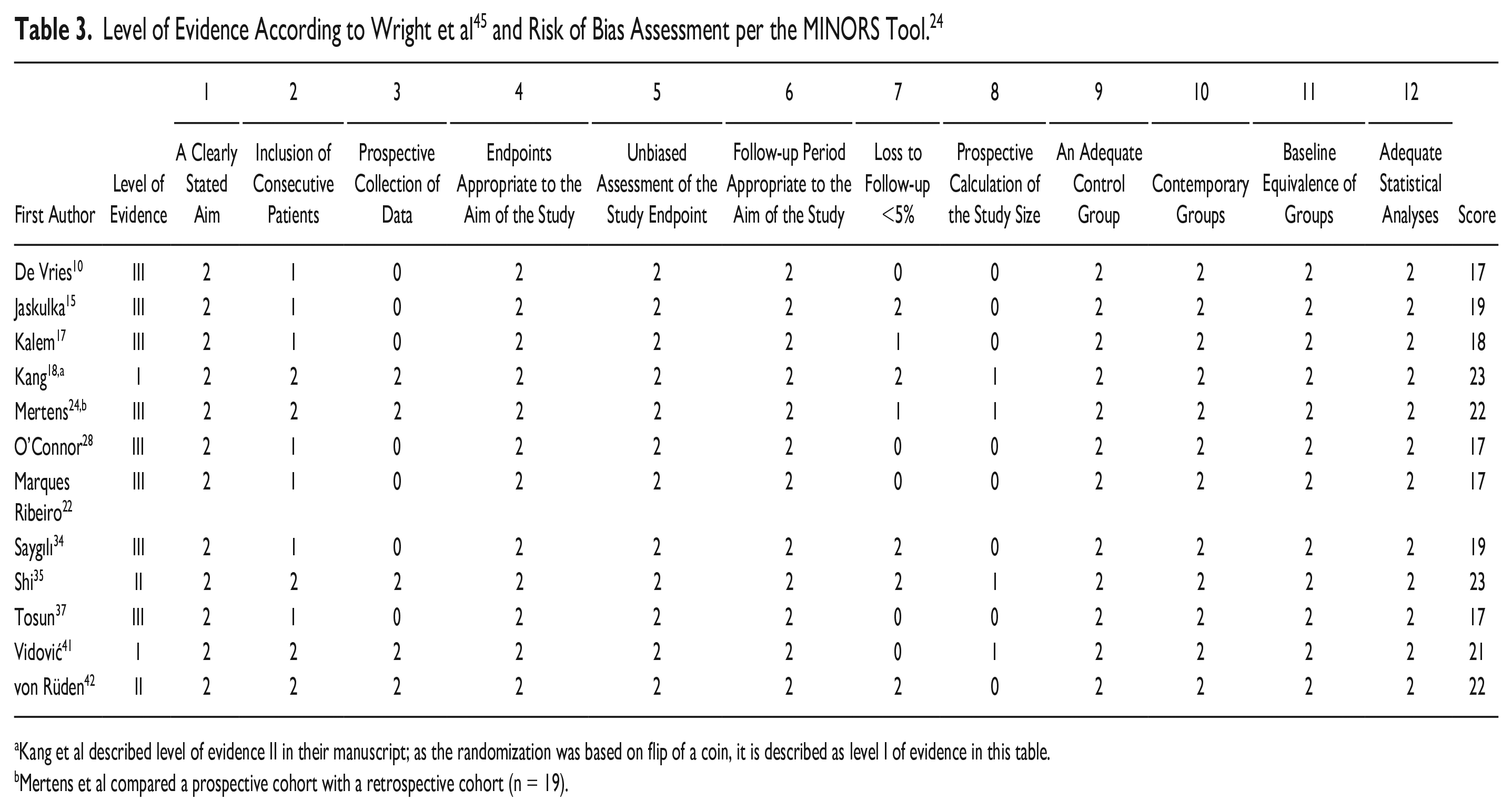
Kang et al described level of evidence II in their manuscript; as the randomization was based on flip of a coin, it is described as level I of evidence in this table.
Mertens et al compared a prospective cohort with a retrospective cohort (n = 19).
Overview of the 12 Studies Included.
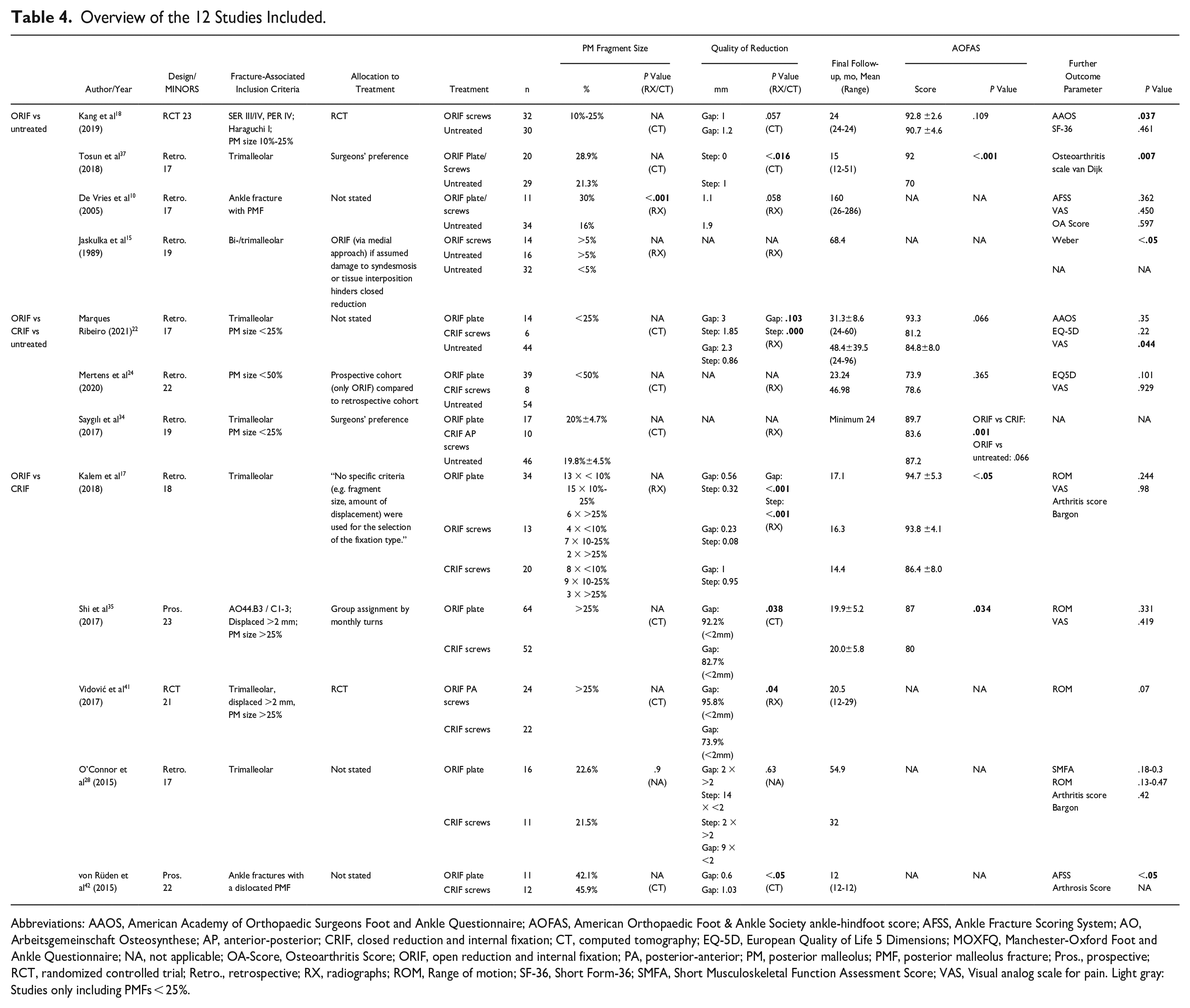
Abbreviations: AAOS, American Academy of Orthopaedic Surgeons Foot and Ankle Questionnaire; AOFAS, American Orthopaedic Foot & Ankle Society ankle-hindfoot score; AFSS, Ankle Fracture Scoring System; AO, Arbeitsgemeinschaft Osteosynthese; AP, anterior-posterior; CRIF, closed reduction and internal fixation; CT, computed tomography; EQ-5D, European Quality of Life 5 Dimensions; MOXFQ, Manchester-Oxford Foot and Ankle Questionnaire; NA, not applicable; OA-Score, Osteoarthritis Score; ORIF, open reduction and internal fixation; PA, posterior-anterior; PM, posterior malleolus; PMF, posterior malleolus fracture; Pros., prospective; RCT, randomized controlled trial; Retro., retrospective; RX, radiographs; ROM, Range of motion; SF-36, Short Form-36; SMFA, Short Musculoskeletal Function Assessment Score; VAS, Visual analog scale for pain. Light gray: Studies only including PMFs < 25%.
Two studies were rated as level I according to Wright et al 45 , 2 studies level II and 8 studies level III. The mean MINORS score 36 of all studies included was 19.6 points (range: 17-23) (Table 3). Seven studies compared ORIF to CRIF17,22,34,35,41,42,46 and 6 studies ORIF to untreated PM fragments10,15,18,22,34,37 and 2 studies compared ORIF to CRIF to untreated PM fragment.22,34 The ORIF groups varied per the surgical approach and the choice of implants. Two studies pooled screws and plates for their ORIF group.10,37 Mertens et al 24 was the only study to present pooled data for CRIF and untreated PM fragments. Overall, the studies included revealed a considerable heterogeneity, regarding the fractures included; the size of the PM fragment (based on the description by Langenhuijsen et al); the surgical treatment strategies for the posterior, lateral, and medial malleolus; the follow-up durations; and the type of outcomes assessed. Because of this heterogeneity, a meta-analysis appeared not appropriate. Still, if any parameter would be assessed in a comparable manner and would be reported by 3 or more studies, the authors aimed to perform a quantitative analysis in order to objectify the results despite the considerable heterogeneity. Still, the PM fracture sizes described were heterogenous among this systematic review and were described in their feasible subgroups in Table 4.
Primary Outcome Parameters
Objective outcome measure
The objective outcome parameters assessed are presented in Table 4. Similar outcome parameters, assessed in at least 3 studies, were the American Orthopaedic Foot & Ankle Society ankle-hindfoot score (AOFAS) 19 in 7 studies,17,18,22,24,34,35,37 the degree of osteoarthritis in 6 studies,10,17,28,37,42,46 the visual analog scale for pain (VAS) in 4 studies,10,17,24,35 and the range of motion (ROM) in 4 studies.17,28,35,41 All but 1 study 18 assessed the objective outcome at final follow-up, which varied between 12 42 and 160 months. 10 The AOFAS score was the only objective outcome measure assessed identically in all studies. Consequently, the AOFAS was the only parameter suitable for a cumulative analysis.
AOFAS score
Those studies reporting the AOFAS score were grouped per the comparator, that is, ORIF vs CRIF AP screws and ORIF vs untreated PM fragment. In case studies including both comparators, that is, ORIF vs AP screws vs untreated, these were included separately in both analysis. Mertens et al 24 did not differentiate between CRIF and untreated patients and could therefore not be grouped per the comparator. Consequently, the study was excluded from the quantitative analysis.
ORIF vs CRIF
Four studies, compromising of 5 groups, compared ORIF vs CRIF AP screws (0 randomized controlled trials, 1 prospective study, 3 retrospective studies).17,22,34,35 Per the individual studies, 3 studies (4 groups) reported significantly better AOFAS scores for the ORIF group17,34,35 and 1 retrospective study found no significant differences 22 (Figure 2): No study reported significantly better AOFAS scores for the CRIF AP screw group. Taken together in the quantitative analysis (Figure 2), 142 patients treated by ORIF and 108 treated by CRIF were included. Because of varying data, no weighted mean follow-up could be calculated. The follow-up periods varied between 14.4 17 and 31.3 months. 22 The quantitative analysis revealed significantly (P < .001) better AOFAS scores following ORIF (weighted mean: 90.9 points) compared to CRIF (weighted mean: 83.4 points) with a mean difference for the AOFAS score of 7.5 points. The model resulted in a low level of heterogeneity (I2 = 0%; P = .57).

Forest plot comparing AOFAS of ORIF vs. CRIF treated PM fragments. AOFAS was significantly better in the ORIF treated groups (P < .001).
ORIF vs untreated PM
Three studies compared ORIF to no treatment for the PM fragment (1 randomized controlled trial, 0 prospective, and 2 retrospective studies).18,34,37 One retrospective study by Tosun et al 37 reported significantly better AOFAS scores for the ORIF group and the prospective study by Kang et al,18,34 and one retrospective study found no significant differences (Figure 3). No study reported significantly better AOFAS scores for the untreated PM group. In the quantitative analysis (Figure 3) the results of 69 patients treated by ORIF were compared to 105 patients with untreated PM fragment. The follow-up varied between 15 37 and a minimum of 24 months. 34 Again, ORIF (weighted mean: 92.0 points) resulted in better AOFAS scores compared to untreated PM fragments (weighted mean: 82.5 points) with a mean difference of 9.5 points. The test for overall effect retrieved a P value of .21. The analysis revealed a high level of heterogeneity (I2 = 99%; P < .00001).
For the ORIF vs CRIF comparison, the mean weighted SDs were 6.1/7.1 points and for the ORIF vs untreated PM fragments 3.1/5.0 points.

Forest plot comparing AOFAS of ORIF vs. untreated PM fragments. ORIF showed significantly better PROMs regarding AOFAS compared to the untreated group (P < .001).
Other PROMs
Two studies reported outcome based on the Ankle Fracture Scoring System (AFSS).10,42 De Vries et al 10 found no significant differences (P = .362) comparing ORIF to no treatment of the PM fragment. von Rüden et al 42 reported significantly better AFSS scores for ORIF compared to CRIF with AP screws (P < .05). Two studies assessed the American Academy of Orthopaedic Surgeons Foot and Ankle Questionnaire.18,22 One of these reported significantly better results (P = .037) for ORIF compared to the untreated PM group, 18 and the second study found no significant differences (P = .35) comparing ORIF to CRIF. 22 Two studies assessed the health-related quality of life using the EQ-5D reporting. Mertens et al 24 reported no significant differences between the ORIF and plate cohort compared to the CRIF/untreated group as well as Marques Ribeiro et al 22 comparing ORIF plate and CRIF screws.
Secondary outcome parameters
Quality of reduction
Data on the quality of reduction was reported in 9 studies. But there was a considerable heterogeneity on what parameters were used (ie, reduction gap [mm]10,17,18,22,28,35,41,42 or articular step-off [mm]17,22,28,37), and how the quality of reduction was assessed (ie, plain radiographs10,17,22,24,34,37,41 or CT18,35,42). Jaskulka et al 15 and O’Connor et al 28 did not specify the type of imaging use. Therefore, no quantitative analysis could be conducted. Overall, 5 of 9 studies17,22,35,41,42 reported a significantly better quality of reduction when the PM fragment was treated by ORIF compared to CRIF. One study 37 showed improved quality of reduction after ORIF of the PM fragment compared to untreated PM fragment. Three studies10,18,28 found no significant difference: 2 studies compared ORIF with untreated PM fragment, one study compared ORIF vs CRIF.
Transsyndesmotic fixation
Four studies reported on the frequency of transsyndesmotic fixation per the different PM fracture treatment strategies. One study compared ORIF to untreated PM fractures, with significantly fewer transsyndesmotic fixations in the ORIF group (5% vs 52%; P = .002). 37 Two studies compared ORIF to CRIF reporting no considerable differences per the frequency of additional transsyndesmotic fixation.17,28 Saygılı et al 34 found additional syndesmotic stabilization in 18% for ORIF, 30% for CRIF, and 67% for untreated PM fragments.
Osteoarthritis
Five studies10,17,28,37,42 reported on the degree of osteoarthritis, but used varying classification systems. The follow-up ranged between 12 42 and 160 months. 10 Only 4 studies performed a statistical analysis.10,17,28,37 Two studies used the scoring system of Bargon 2 and found no significant differences between ORIF and CRIF.17,28 One study applied the osteoarthritis scale by van Dijk 38 and found significantly better results for ORIF compared to untreated PM fragments (P = .007). 37 De Vries et al 10 found no significant differences between ORIF and untreated PM fractures (P = .597) using the Osteoarthritis Score.
Discussion
Twelve studies were included in the qualitative analysis and 6 studies in the quantitative analysis. The quantitative analysis revealed significantly better AOFAS scores for patients treated by ORIF compared to CRIF (Figure 2). Better results with no statistical significance were observed comparing ORIF to untreated PM fractures (Figure 3). A similar trend was observed for the qualitative analysis of the AFSS and the American Academy of Orthopaedic Surgeons Foot and Ankle Questionnaire. Per the secondary outcome parameters, ORIF resulted in a significantly better quality of reduction. In contrast, only 1 study, by van Dijk et al, 38 showed significantly lower scales of posttraumatic arthritis. Frequency of additional transsyndesmotic fixation following ORIF or other treatment options of the PM fragment was heterogenous among all groups.
The AOFAS was the most used score and therefore the predominant outcome parameter. Despite its frequent use in foot and ankle research, the AOFAS has been questioned for its validity, responsiveness, and applicability.7,14,21,29 Per the AOFAS Score, ORIF of the PM (vs CRIF/untreated) resulted in overall excellent (90.9 points/92.0 points; 90-100 points), CRIF and untreated PM fragments in good (83.4/82.5 points; 75-89 points) results. 1 Whether the herein calculated mean differences of 7.5/9.5 points (ORIF vs CRIF/untreated PM fragments) are of clinical importance is debatable as the minimal clinically important difference (MCID) for the AOFAS score in ankle fracture patients is unknown.20,31 The AOFAS MCID for hallux valgus has been reported to be 8.9 (SD 1.2) points. 8 Other studies have suggested that the MCID resembles 50% of the observed SD.16,27 For the ORIF vs CRIF comparison, the mean weighted SDs were 6.1/7.1 points and for the ORIF vs untreated PM fragments 3.1/5.0 points. MCIDs resembled <50% in this review regarding the treatment comparison based on the PROMs on AOFAS. Consequently, it seems reasonable that ORIF of the PM results in clinically significantly better AOFAS scores than CRIF or untreated PM fragments. Still, this was not a statistical finding but a clinical one.
Furthermore, comparison between varying operative techniques to studies where a further cohort included nonoperated PM fragments should be mentioned as clinical findings suggesting improved AOFAS scores after ORIF were described within this systematic review. Saygılı et al were the only authors reporting AOFAS score for an ORIF cohort, a CRIF cohort, and an untreated PM fragment cohort within the quantitative synthesis (Figures 2 and 3). All other authors showed data of 2 cohorts.
One of the major factors for impaired functional outcome following surgical treatment of ankle fractures is posttraumatic arthritis. 40 Risk factors for posttraumatic arthritis include the fracture severity3,4 as well as the degree of bony and syndesmotic reduction. 4
Despite the higher quality of bony and possibly syndesmotic reduction, the benefit of ORIF on the development of posttraumatic arthritis remains unknown. Only 4 studies assessed the degree of posttraumatic arthritis in more detail, with inconclusive results.10,17,28,42 Still, the degree of posttraumatic arthritis was only assessed on plain radiographs with a short-term follow-up (mean follow-up <24 months in 3 of 5 studies). It can be hypothesized that the follow-up period was too short to find radiographic apparent osteoarthritic changes.
Whereas the fracture severity is a nonmodifiable risk factor, both the degree of bony and syndesmotic reduction are possibly modifiable by the treatment strategy of the PM fragment. Although not specifically designed to answer these questions, 9 studies included in the herein presented systematic review also reported on the quality of bony reduction per the different PM fragment treatment strategies. Even though limited because of a considerable heterogeneity, ORIF apparently resulted in a superior quality of reduction compared to CRIF17,22,35,41,42 and untreated PM fragment. 37
Whether ORIF does also result more frequently in an anatomical reduction of the syndesmosis could not be assessed in this review, as only 3 studies assessed the quality of reduction on postoperative CT images18,35,42 and it remained unknown, whether this was done on uni- or bilateral images. Still, only 2 of these studies conducted a further statistical analysis. O’Connor et al 28 and Tosun et al 37 showed significantly lower rate of transsyndesmotic fixation in the ORIF group. A significant reduction of additional transsyndesmotic fixation following ORIF of the PM fragment, compared to CRIF or untreated PM fragments, has been reported in other studies as well. 4 Baumbach et al stated that ORIF restores syndesmotic stability more often than untreated PM fragment or CRIF as the syndesmotic injury with the effect to stabilize the PITFL. Still, it is not clear whether the prone position might have had an effect as it was not described by the included studies. Actually, the destabilization ankle fractures is bone- and ligament-related. As on the one hand, fractures are fixed, ligament injuries must be addressed to stabilize the ankle and its joints—tibiotalar, tibiofibular, and fibulotalar—a complex dependence on each other that underlines the importance of evidence-based knowledge how to treat ankle fractures at its best.
Limitations
Nevertheless, this systematic review has its limitations, most pronounced in the heterogeneity within the included studies. Each of these studies was dependent of different decision making regarding how to treat PM fragments in ankle fractures. Of those studies not (pseudo-)randomized, 3 did not state on the actual decision-making process. Four studies stated that the decision was made “per the surgeon’s preference.” Only 1 study, by Jaskulka et al, 15 facilitating a medial approach to the PMF, based its decision on ORIF vs untreated based on the initial presentation of the fracture.
Future studies should use CT images to assess the size of the PM fragment as well as the quality of reduction, clearly differentiating between the different fracture types, that is, bi- or trimalleolar fractures, and apply well-validated outcome scores at defined follow-up periods with a sufficiently long final follow-up. PM fragment sizes were heterogenous in this systematic review independently described on which radiologic image tools were used. These heterogeneities prohibited not only a meta-analysis but also a sufficient analysis of other co-founders, such as fracture severity or the degree of syndesmotic reduction. Because ankle fractures are such frequent injuries, it is essential to develop evidence-based guidelines for their treatment. To develop these guidelines, we as transsyndesmotic surgeons, must agree on standards regarding the conduction of future studies. This is essential to increase the comparability and thereby the conclusiveness of the studies available.
Despite these limitations, this is the first systematic review to assess the patient-rated outcome of ORIF of the PM fragment. The systematic review was conducted according to the recommendations of PRISMA, including a well-structured search strategy, applied to 5 databases, and a gray literature search. Furthermore, only studies comparing ORIF to either CRIF or untreated PM fragments were included.
Findings
Despite a considerable heterogeneity between the studies eligible for this systematic review, the data available point to a superior patient-rated outcome following ORIF of the PM fragment, compared to CRIF or no treatment. Furthermore, ORIF of the PM fragment appears to result in a favorable quality of reduction with therefore improved sagittal plane stability and possibly lower rate of syndesmotic fixation. High-quality randomized controlled trials are needed to prove the herein observed trends and to define clear treatment recommendations.
Supplemental Material
sj-docx-3-fai-10.1177_10711007231165771 – Supplemental material for Open Reduction and Internal Fixation of the Posterior Malleolus Fragment in Ankle Fractures Improves the Patient-Rated Outcome: A Systematic Review
Supplemental material, sj-docx-3-fai-10.1177_10711007231165771 for Open Reduction and Internal Fixation of the Posterior Malleolus Fragment in Ankle Fractures Improves the Patient-Rated Outcome: A Systematic Review by Rainer Christoph Miksch, Viktoria Herterich, Alexej Barg, Wolfgang Böcker, Hans Polzer and Sebastian Felix Baumbach in Foot & Ankle International
Supplemental Material
sj-jpeg-2-fai-10.1177_10711007231165771 – Supplemental material for Open Reduction and Internal Fixation of the Posterior Malleolus Fragment in Ankle Fractures Improves the Patient-Rated Outcome: A Systematic Review
Supplemental material, sj-jpeg-2-fai-10.1177_10711007231165771 for Open Reduction and Internal Fixation of the Posterior Malleolus Fragment in Ankle Fractures Improves the Patient-Rated Outcome: A Systematic Review by Rainer Christoph Miksch, Viktoria Herterich, Alexej Barg, Wolfgang Böcker, Hans Polzer and Sebastian Felix Baumbach in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231165771 – Supplemental material for Open Reduction and Internal Fixation of the Posterior Malleolus Fragment in Ankle Fractures Improves the Patient-Rated Outcome: A Systematic Review
Supplemental material, sj-pdf-1-fai-10.1177_10711007231165771 for Open Reduction and Internal Fixation of the Posterior Malleolus Fragment in Ankle Fractures Improves the Patient-Rated Outcome: A Systematic Review by Rainer Christoph Miksch, Viktoria Herterich, Alexej Barg, Wolfgang Böcker, Hans Polzer and Sebastian Felix Baumbach in Foot & Ankle International
Footnotes
Ethical Approval
The study was approved by İzmir Katip Çelebi University, Turkey Medical Faculty Institutional Review Board Committee with decision number 0343 and was performed according to Helsinki ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.