
Abstract
Background:
Primary Achilles tendon repair (ATR) can be performed in ambulatory surgery centers (ASCs) or hospitals. We compared costs and complication rates of ATR performed in these settings.
Methods:
We retrospectively queried the electronic medical record of our academic health system and identified 97 adults who underwent primary ATR from 2015 to 2021. Variables were compared between patients treated at ASCs vs those treated in hospitals. We compared continuous variables with Wilcoxon rank-sum tests and categorical variables with χ2 tests. We used an α of 0.05. Multivariable logistic regression was performed to determine associations between surgical setting and costs. Linear regression was performed between each charge subtype and total cost to identify which charge subtypes were most associated with total cost.
Results:
Patients who underwent ATR in hospitals had a higher rate of unanticipated postoperative hospital admission (13%) than those treated in ASCs (0%) (P = .01). We found no differences with regard to postoperative complications, emergency department visits, readmission, rerupture, reoperation/revision, or death. Patients treated in hospitals had a higher mean (±SD) implant cost ($664 ± $810) than those treated in ASCs ($175 ± $585) (P < .01). We found no differences between settings with regard to total cost, supply costs, operating room charges, or anesthesia charges. Higher implant cost was associated with hospital setting (odds ratio = 16 [95% CI: 1.7-157]) and body mass index > 25 (odds ratio = 1.2 [95% CI: 1.0-1.5]). Operating room costs were strongly correlated with total costs (R2 = .94).
Conclusion:
The overall cost and complication rate of ATRs were not significantly different between ASCs and hospitals. ATRs performed in hospitals had higher implant costs and higher rates of postoperative admission than those performed in ASCs.
Level of Evidence:
Level III, retrospective comparative study.
Introduction
Achilles tendon rupture is one of the most common tendon injuries, with reported worldwide incidence of 2 to 55 per 100 000 person-years.13,16,17,28,30 The incidence of Achilles tendon rupture is increasing, particularly among middle-aged adults,10,15 which some attribute to an increase in participation in recreational sports in this population. 16 Operative Achilles tendon repair (ATR) costs approximately 3 times as much as nonoperative treatment. 29 Primary ATR is most commonly performed as an outpatient procedure, either in ambulatory surgery centers (ASCs) or hospitals.
As we move toward a value-based health care system, it is important for surgeons to understand the drivers of surgical costs and how to minimize these costs. Few surgeons understand the cost implications of the setting in which their care is provided; therefore, they cannot make fully informed decisions regarding costs of care.11,25 Surgical setting has been found to be a significant contributor to cost of care.3,18
There is little research comparing the costs of ATR performed in ASCs vs hospitals. Previous studies examining the cost of treatment of Achilles tendon rupture have focused on operative vs nonoperative care.23,29,32 The only study we are aware of that examined operative management of Achilles tendon rupture focused on the costs of open vs percutaneous repair. 6 There has been little research into surgical setting as a cost driver in ATR; the study that did address this question examined only cases performed in ASCs and looked at whether the ASC was low or high volume, as well as whether it was privately owned or hospital-owned. 18 Studies in the orthopaedic foot and ankle literature have investigated surgical setting as a contributor to costs in the operative management of ankle fractures, finding that outpatient surgery is associated with lower costs and fewer postoperative complications compared with inpatient surgery.3,20,27
Our objective was to compare the costs and complications of primary ATR performed in ASCs vs the hospital. We hypothesized that ATR performed in ASCs would be less costly and would not be associated with a higher rate of complications compared with ATR performed in the hospital.
Methods
Institutional review board approval was obtained for this study.
Data Source and Study Population
We searched the electronic medical record of our large, urban, US academic medical system for patients who underwent primary ATR (Current Procedural Terminology code 27650) between January 2015 and September 2021. We included patients aged 18 years or older who underwent primary ATR by any method. We excluded patients who underwent revision ATR, those who required flexor hallucis longus tendon transfer, as well as those for whom cost data were incomplete.
Variables of Interest
Patient characteristics
We extracted data on the following patient characteristics: age, sex, race/ethnicity (white/Caucasian, Black/African American, Asian/Pacific Islander, Hispanic, Native American/Alaska native, other race/ethnicity), body mass index (BMI) value, American Society of Anesthesiologists (ASA) physical classification (1-4), smoking status (never, former, current), cardiopulmonary comorbidities (history of coronary artery disease, myocardial infarction [MI], asthma, chronic obstructive pulmonary disease), and diabetes status. We also assessed data on whether the injury was acute or chronic.
Surgical variables
Surgical variables of interest were date of surgery, surgeon, surgeon’s subspecialty training (foot and ankle, sports, or trauma), surgical setting (ASC or hospital), surgical technique (open or percutaneous [whether the Achilles tendon sheath was opened during the procedure]), suture technique if open (Krakow or core weave), and postoperative hospital admission. Factors contributing to selection of surgical setting included surgeon preference and patient comorbidity profile.
Complications
We assessed cardiopulmonary complications (MI, cardiac arrest, pneumonia, prolonged intubation [inability to extubate at the end of the procedure]); thromboembolic complications (deep vein thrombosis, pulmonary embolism, cerebrovascular accident); wound complications (superficial surgical site infection, deep surgical site infection, wound dehiscence, wound drainage); nerve complications (sensory deficit, motor deficit, neuropathic pain) and reoperation/revision, rerupture, emergency department (ED) visit, hospital readmission, or death within 30 days after the procedure.
Costs
We assessed the following costs (in US dollars): direct surgery cost, direct implant cost, and total direct cost. Cost data were extracted directly from the electronic medical record.
Statistical Analysis
Patient characteristics, surgical factors, and postoperative complications were compared between patients treated in ASCs and those treated in the hospital. Continuous variables were assessed for normal distribution via the Shapiro-Wilk test. All continuous variables were determined to be nonnormally distributed, and we used Wilcoxon rank-sum tests to compare them. Continuous variables are reported as means ± SDs and were compared using χ2 tests. The α-value was set at .05.
For any cost subtype that differed significantly between surgical settings on bivariate analysis, we performed multivariable logistic regression to identify whether surgical setting was associated with differences in cost. Ultimately, the multivariable model included age, sex, BMI value, active tobacco use, surgeon subspecialty, and surgical setting. To identify which charge subtype was most associated with total cost, we performed simple linear regression between each charge subtype and total cost. Analyses were performed in Stata, version 17, software (StataCorp LLC, College Station, TX).
Ninety-seven patients were included in our analysis. Demographic and preoperative patient characteristics are described in Table 1. Patients who underwent ATR in the hospital were more likely to be active tobacco users (P < .01). Ninety-nine percent of ATRs were performed for acute injuries.
Demographic and Preoperative Characteristics of 97 Patients Who Underwent Primary Achilles Tendon Repair in ASCs vs Hospitals from 2015 to 2021.
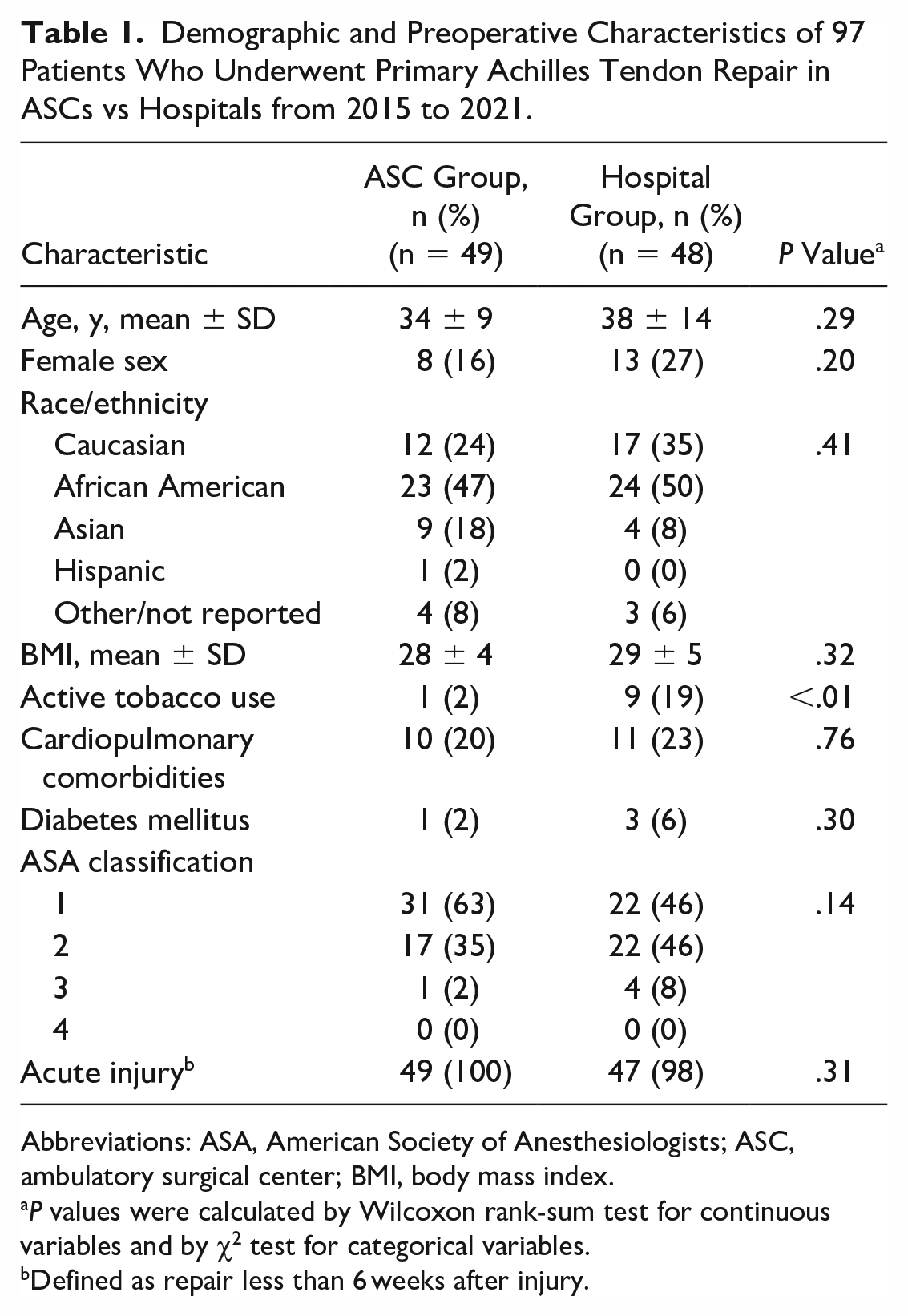
Abbreviations: ASA, American Society of Anesthesiologists; ASC, ambulatory surgical center; BMI, body mass index.
P values were calculated by Wilcoxon rank-sum test for continuous variables and by χ2 test for categorical variables.
Defined as repair less than 6 weeks after injury.
In ASCs, ATRs were more often performed by sports medicine subspecialists, and in hospitals, ATRs were more often performed by foot and ankle or trauma subspecialists (all, P < .001). In ASCs, ATRs more often used an open technique (P < .001), with the Krakow and core weave techniques being most common. Surgical characteristics for the cohort are presented in Table 2.
Surgical Variables and Postoperative Complications of 97 Patients Who Underwent Primary Achilles Tendon Repair in ASCs vs Hospitals from 2015 to 2021.

Abbreviations: ASC, ambulatory surgical center; ED, emergency department.
P values calculated by χ2 test.
Results
Complications
Postoperative complications are presented in Table 2. We found no differences between the cohorts with regard to cardiopulmonary, thromboembolic, wound, or nerve complications, and no differences in postoperative ED visits, readmission, rerupture, reoperation/revision, or death. Patients treated in the hospital were more likely to have an unanticipated postoperative hospital admission than those treated in ASCs (P = .01).
Costs
ATR cases performed in the hospital had a higher mean implant cost than those performed in ASCs (P < .01) (Table 3). We found no differences between the ASC and hospital groups with regard to total cost; however, we found greater variability in total cost within the ASC group (Figure 1). We found no differences between the ASC and hospital groups with regard to supply costs, operating room charges, or anesthesia charges (Table 3). Multivariable logistic regression (Table 4) showed that hospital setting (odds ratio [OR] = 16 [95% CI: 1.7-157]) and BMI value (OR = 1.2 [95% CI: 1.0-1.5]) were associated with higher implant cost. Operating room costs were strongly correlated with total costs (R2 = .94, Figure 2).
Procedure Costs for 97 Patients Who Underwent Primary Achilles Tendon Repair from 2015 to 2021, by Surgical Setting. a
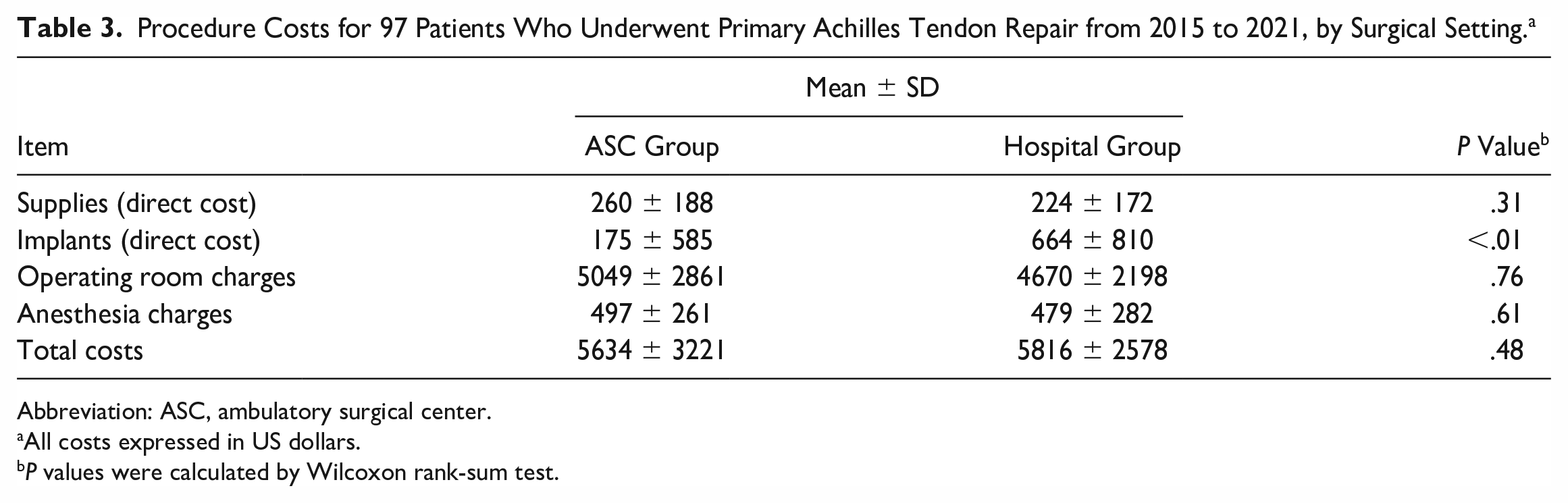
Abbreviation: ASC, ambulatory surgical center.
All costs expressed in US dollars.
P values were calculated by Wilcoxon rank-sum test.

Total cost (in US dollars) between Achilles tendon repairs performed at an ambulatory surgery center (ASC) vs those performed in the hospital. Total costs between surgeries performed at an ASC were not significantly different than those performed at a hospital.
Adjusted Odds a for Implant Direct Cost in 97 Patients Who Underwent Primary Achilles Tendon Repair from 2015 to 2021.

Abbreviation: OR, odds ratio.
Area under receiver operating curve for model: 0.88.

Operating room charges vs total cost of each Achilles tendon repair, per patient. Operating room charges had the highest correlation with total cost of the procedure. The R2 of the linear regression model was 0.94.
Discussion
The goal of this study was to compare costs and complications of ATRs performed in ASCs vs the hospital. We found no difference in total cost of ATR between settings. Thus, our hypothesis regarding cost was not supported. This still represents an important finding; insurance carriers are attempting to move these procedures to ASCs under the premise of cost containment. These data suggest that it is not necessarily more cost efficient for the insurer.
We found that ATRs performed in hospitals had higher implant costs and were more likely to result in postoperative hospital admission in this population. We found no differences in rates of other complications between the groups, which supports the hypothesis that performance of ATR in ASCs is not associated with a higher rate of complications. Furthermore, we found that operating rooms costs were most strongly correlated with total costs of ATR.
In ASCs, ATR was more likely to be performed by sports medicine–trained surgeons and was more likely to use an open technique. In contrast, ATRs performed in hospitals were more likely to be performed by trauma or foot and ankle subspecialists and were more likely to use a percutaneous technique. To our knowledge, this is the first study to show such differences in ATR by orthopaedic subspecialty, though this pattern may not be widely generalizable. Previous research found no differences in surgical management of Achilles tendon rupture between sports medicine and foot and ankle surgeons. 26 These differences may be one explanation for the higher implant costs associated with hospital-based procedures because foot and ankle surgeons, who more frequently operated in the hospital setting, may be more comfortable with the percutaneous technique and use the accompanying implant systems, which are often more expensive. 12 Another potential explanation for this pattern is that hospitals are able to bill for more expensive implant systems, which drives the use of these implants out of the ASC and into the hospital setting. Higher BMI value was also associated with greater implant cost, though the reason for this finding is unclear. A potential explanation for this pattern is that surgeons may choose the percutaneous ATR systems, which are generally more expensive, in this population secondary to wound healing concerns because obesity is a risk factor for wound complications after ATR. 5 The use of a percutaneous technique involves a smaller surgical incision and less soft-tissue dissection, both of which help decrease incision-related complications. 12
Patients treated in the hospital were more likely to be admitted to the hospital after ATR. This finding is consistent with previous research on the subject, which found that ambulatory orthopaedic procedures performed in hospital-based facilities were associated with greater risk of unexpected disposition. 22 Unanticipated hospital admission may result from surgical, anesthesia, or medical complications, as well as social or organizational issues. Numerous studies have analyzed predictors of unanticipated admission after ambulatory surgery; older age, ASA class 3 or 4, duration of surgery, and patient comorbidities have consistently been shown to be risk factors for admission after outpatient surgery.7,21,31,33 Another potential explanation for this finding is related to proximity, because it is easier to facilitate hospital admission when a patient is already in the hospital.
Operating room costs were most strongly correlated with total cost of ATR in this study. This finding is consistent with other cost analyses in the orthopaedic literature. Operating room costs were consistently significant drivers of total cost in subspecialties as varied as sports medicine, arthroplasty, trauma, and spine.2,4,9,14,19 Implants and anesthesia costs were also frequently cited as the greatest contributors to cost.4,14,24 This finding is important because it demonstrates drivers of cost that can be further optimized in the orthopaedic surgery population. Given its correlation with surgical costs, operating room cost is becoming an increasingly important target for efficacy efforts.1,8 Surgeons can contribute to these efforts in various ways, including reduction of operative time, standardization of surgical instruments, and implementation of service-specific surgical teams. 8
The main strength of this study is that it enabled analysis of granular cost data, which is not typically possible when using a large national database. Additionally, we were able to choose clinically important data points, such as surgical technique and complications most likely to affect the study population. However, the study also has limitations. Our analysis relied on clinical data from one large academic medical center, and therefore may have limited generalizability. The sample size is also limited, and we excluded patients with incomplete clinical or cost data, which may reduce the generalizability of these results. Additionally, we were unable to parse out other costs, such as facility fees. Another potential confounding factor is that the foot and ankle surgeons in this study were more likely to operate in the hospital setting, as opposed to sports surgeons, who overwhelmingly operate in ASCs. This factor may contribute to the differences we found in surgical approaches and the associated cost differences. Finally, given the retrospective design of this study, we cannot determine causal relationships.
Conclusions
We found no difference in total cost of ATR performed in ASCs compared with hospitals. However, ATRs performed in hospitals had higher implant costs. Operating room costs were most strongly correlated with total procedure cost of ATR. Although we found a higher rate of postoperative admission among patients treated in the hospital, we found no other differences between the ASC- and hospital-based cohorts with regard to postoperative complications.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231205306 – Supplemental material for Surgical Setting in Achilles Tendon Repair: How Does It Relate to Costs and Complications?
Supplemental material, sj-pdf-1-fao-10.1177_24730114231205306 for Surgical Setting in Achilles Tendon Repair: How Does It Relate to Costs and Complications? by Rachel S. Bronheim, Henry T. Shu, Meghana Jami, Nigel N. Hsu and Amiethab A. Aiyer in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
For editorial assistance, we thank Rachel Walden, MS, in the Editorial Services group of The Johns Hopkins Department of Orthopaedic Surgery.
Ethical Approval
The study received institutional review board approval.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rachel S. Bronheim, MD, reports grants or contracts from any entity: National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) of the National Institutes of Health, T32 AR07708-08. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) of the National Institutes of Health under award number T32 AR07708-08 (RSB).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.