
Abstract
Background:
There is no current consensus on whether to use an open or minimally invasive (MIS) approach for Achilles tendon repair after acute rupture. We hypothesized that patients in both open and MIS groups would have improved patient-reported outcome scores using the PROMIS system postoperatively, but that there would be minimal differences in these scores and complication rates between operative techniques.
Methods:
A total of 185 patients who underwent surgery for an acute, unilateral Achilles tendon rupture between January 2016 and June 2019, with minimum 1-year follow-up were included in the cohort studied. The minimally invasive group was defined by use of a commercially available minimally invasive device through a smaller surgical incision (n=118). The open repair group did not use the device, and suture repair was performed through larger surgical incisions (n=67). Postoperative protocols were similar between groups. Preoperative and postoperative PROMIS scores were collected prospectively through our institution’s registry. Demographics and complications were recorded.
Results:
PROMIS scores overall improved in both study groups after operative repair. No significant differences in postoperative PROMIS scores were observed between the open and MIS repair groups. There were also no significant differences in complication rates between groups. Overall, 19.5% of patients in the MIS group had at least 1 postoperative complication (8.5% deep vein thrombosis [DVT], 3.3% rerupture, 1.7% sural nerve injury, 2.5% infection), compared to 16.4% in the open group (9.0% DVT, 1.5% rerupture, 1.5% sural nerve injury, 0% infection).
Conclusion:
Patients undergoing either minimally invasive or open Achilles tendon repair after acute rupture have similar PROMIS outcomes and complication types and incidences.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
There is no current consensus on whether to use an open or minimally invasive (MIS) approach for Achilles tendon repair after acute rupture. Acute Achilles tendon ruptures can be managed with either operative or nonoperative treatment. Results of acute Achilles ruptures treated nonoperatively have achieved good results in patients with proper indications that follow an appropriate functional rehabilitation protocol.18,23,39-41 When compared to patients who were treated operatively, nonoperative management has been shown to have similar outcomes and complication rates.18,23,39-41 A randomized controlled trial showed that there were no clinically important differences between operatively and nonoperatively treated Achilles tendon ruptures in terms of strength, range of motion, calf circumference, or outcome score. 40 However, there are concerns that nonoperative treatment may lead to rerupture, loss of push-off strength and explosiveness, and a reduced level of postinjury activity.23,39
Minimally invasive and open Achilles repair techniques are commonly used and have been studied to evaluate their efficacy in terms of outcomes and complication rates.4,8,9,11,12,14,22,24,28,34 The most commonly used open Achilles repair techniques include the Krackow and Bunnell suture techniques.22,36 Many minimally invasive techniques have been developed to treat acute Achilles tendon rupture, including the Ma & Griffiths repair, the Webb and Bannister repair, the Achillon device, the Tenolig device, and the PARS repair among other modified percutaneous repair techniques.8,10,14,38 Some studies have shown that minimally invasive techniques have fewer overall complications and lead to a lower risk of infection and wound complications.9,11,24,28,34
Outcome scores have been used to evaluate patient recovery and technique efficacy in MIS and open Achilles tendon repairs. Past studies have used different types of scores to evaluate outcomes after Achilles tendon repair, such as the AOFAS score, 1 Achilles tendon Total Rupture Score (ATRS),4,7 Leppilahti score, 40 and the McComis score. 4 However, none of these scores are computer adaptive and are not validated with the exception of the ATRS score.4,31,32 Though the Patient-Reported Outcomes Measurement Information System (PROMIS) has been validated and assessed for the estimated minimum clinically important difference (MCID) in open Achilles tendon repair, 15 it has not been previously used to compare long-term outcomes of minimally invasive and open Achilles tendon repair techniques. PROMIS-based computer adaptive scores have been advocated for use to improve precision and reduce patient burden when compared to previously used clinical outcome measures.6,16 The PROMIS Physical Function Computerized Adaptive Test (PF CAT) has been recommended for use by the AOFAS. 19 Although many studies have previously examined complication rates and outcomes after acute Achilles tendon repair, 14 no study has compared complication rates in conjunction with PROMIS score outcomes between minimally invasive and open techniques. Given the inconsistencies in the literature and lack of reliable patient-reported outcomes, we set out to compare complication rates between MIS and open techniques while using a long-term validated patient-reported outcome score (ie, PROMIS).
We hypothesized that patients undergoing either MIS or open Achilles tendon repair would have improved postoperative PROMIS scores, but that there would be minimal differences in PROMIS scores and complication rates between the operative techniques.
Materials and Methods
Three hundred twenty-six consecutive patients with operatively treated acute Achilles tendon ruptures between January 2016 and June 2019 were reviewed from a single center of 9 foot and ankle fellowship–trained orthopaedic surgeons. Medical records including clinical and operative notes were reviewed for each patient. All patients were diagnosed with acute Achilles tendon rupture based on history and physical examination and underwent operative management after discussing the risks of operative and nonoperative management. Each attending surgeon exclusively used either the open or minimally invasive procedure based on personal preference and training. Two surgeons in our cohort use the open Achilles tendon repair technique, and 7 surgeons in our cohort use the minimally invasive Achilles tendon repair technique. Patients with Achilles tendinopathy, insertional ruptures, sleeve avulsions, and chronic tears were excluded. Patients aged <18 years and those without postoperative PROMIS scores were also excluded. Of the 326 patients with operatively treated acute Achilles tendon ruptures, 8 patients were excluded because they did not have an open or minimally invasive repair, and 133 patients were excluded from the study because they were missing minimum 1-year postoperative outcome scores and were unable to be contacted, leaving 185 patients (56.8%) that met the inclusion criteria and had a minimum of 1-year postoperative outcome scores.
When comparing patients excluded for both the open and MIS procedure type, there were no differences in sex (P = .59), body mass index (BMI; P = .19), age (P = .92), or complications (P > .05). When comparing open repair patients who were excluded to open repair patients who were included, there were no differences in sex (P = .32), BMI (P = .78), age (P = .34), or complications (P > .05). When comparing MIS patients who were excluded to MIS repair patients who were included, there were no differences in sex (P = .23), BMI (P = .67), age (P = .66), or complications (P > .05).
PROMIS scores in Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression were collected from an institutional review board (IRB)–approved registry after obtaining approval from the registry’s steering committee at the investigators’ institution. PROMIS scores are computer-adaptive tests ranging in scoring from 20 to 80, with higher scores indicating a greater amount of the category being tested. As a standard of care, PROMIS scores are collected from patients using an online database (REDCap) preoperatively, and at 1 and 2 years postoperatively, scores were also collected by follow-up phone call or e-mail beyond the 1- and 2-year time points.
We recorded patient demographics, mechanism of rupture, percentage of injuries due to sports, and time from injury to surgery (days). We also recorded complications that were present in the medical record, which included rerupture, sural nerve injury, infection, deep vein thrombosis (DVT), suture knot irritation, chronic pain, wound complications, other nerve issues, development of tendinosis, and adhesive scar tissue. Procedure duration, use of tourniquet, and primary anesthesia were collected from the medical and operative records. Overall complication rate was calculated for patients with at least 1 complication to account for patients who had multiple complications.
Surgical Technique
There were 2 operative techniques that were used in this study, which involved either MIS (n = 118) or open repair (n=67). The MIS technique was defined as acute Achilles repair with the use of a commercially available minimally invasive device. This method typically utilized a smaller incision, routinely less than 4 cm, to visualize the ruptured tendon edges with sutures passed percutaneously to complete the repair. The open technique was defined as acute Achilles repair without the use of a commercially available minimally invasive device. This technique involved a larger surgical incision, routinely 5 cm or more, that allowed full visualization of the ruptured tendon, and suture repair was then performed using Krackow and Bunnell–type stitches. All cases were performed in the prone position under either regional anesthesia, neuraxial nerve block, or general or peripheral nerve block with the use of a pneumatic thigh tourniquet.
Unless there was a direct contraindication, chemical DVT prophylaxis was selected and administered postoperatively based on the surgeon’s assessment of individualized patient risk factors. All patients followed a similar postoperative protocol, including being in a plantarflexion nonweightbearing splint for weeks 1-2, followed by weightbearing as tolerated in a boot with a heel lift for weeks 3-6, then weightbearing as tolerated in a boot without a heel lift for weeks 7-12 and a return to sport at 6-9 months postoperatively.
Statistical Analysis
We conducted a power analysis that showed with group sample sizes of 56 and 60, we achieved 80% power to detect a minimal clinically important difference (MCID) of –4.2 between the null and alternative hypotheses. The Wilcoxon signed-rank test was used to compare the distribution of continuous variables in 2-group comparisons. The Fisher exact test was used to compare the discrete variables in 2-group comparisons. All P values were 2-sided, and statistical significance was evaluated at the .05 alpha level. Analysis was conducted in SAS, version 9.4.
Results
There were no significant differences between groups in average preoperative PROMIS t scores for Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression (Table 1).
Relationship Between Preoperative PROMIS Scores Between the MIS and Open Repair.

Abbreviations: MIS, minimally invasive; PROMIS, Patient-Reported Outcomes Measurement Information System.
There were no significant differences between groups in average postoperative PROMIS t scores for Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression (Table 2).
Relationship Between Postoperative PROMIS Scores Between the MIS and Open Repair.

Abbreviations: MIS, minimally invasive; PROMIS, Patient-Reported Outcomes Measurement Information System.
There was no difference between average follow-up for postoperative PROMIS scores with 1.6 years for the MIS group and 1.5 years for the open group (P = .64). There was no difference in average time from injury to surgery, with 7.4 days for the MIS group and 7.9 days for the open group (P = .69). There was no difference in percentage injury due to sport, with 85.6% of the MIS group and 91.0% of the open group injured due to sport (P = .24). There was no difference in average patient age on procedure date; the average age in the MIS group was 37.6 years and 39.1 years in the open group (P = .55). There was no difference in average BMI between groups, as the average BMI was 26.7 in the MIS group and 25.7 in the open group (P = .23). There was no difference between procedure groups based on gender: 82.2% of the MIS group and 77.60% of the open group were male; 17.8% of the MIS group and 22.40% of the open group were female (P = .45).
There were no significant differences between groups with respect to the most common sport-related mechanisms of rupture: basketball, tennis, and soccer (P = .67) (Table 3).
Summary of Mechanism of Acute Achilles Tendon Rupture in the MIS and Open Repair Groups.

Abbreviation: MIS, minimally invasive.
Procedure duration was significantly shorter in the MIS group, with an average duration of 43.2 minutes compared to 47.1 minutes in the open group (P = .0058).
Complication rates were not significantly different between the MIS and open groups: for patients with at least 1 postoperative complication, we had an overall complication rate of 19.5% in the MIS repair and 16.4% in the open repair (P = .69).
Major complications requiring a return to the operating room included reruptures and deep infections. There were 4 reruptures (3.3%) in the MIS group and 1 rerupture (1.5%) in the open group (P > .99). There were 3 deep infections (2.50%) in the MIS group and no infections (0%) in the open group (P = .56) (Table 4). Other minor complications that resolved without a return to the operating room were not significantly different between repair groups (P > .05) (Table 4).
Summary of Complications Between Repair Groups.
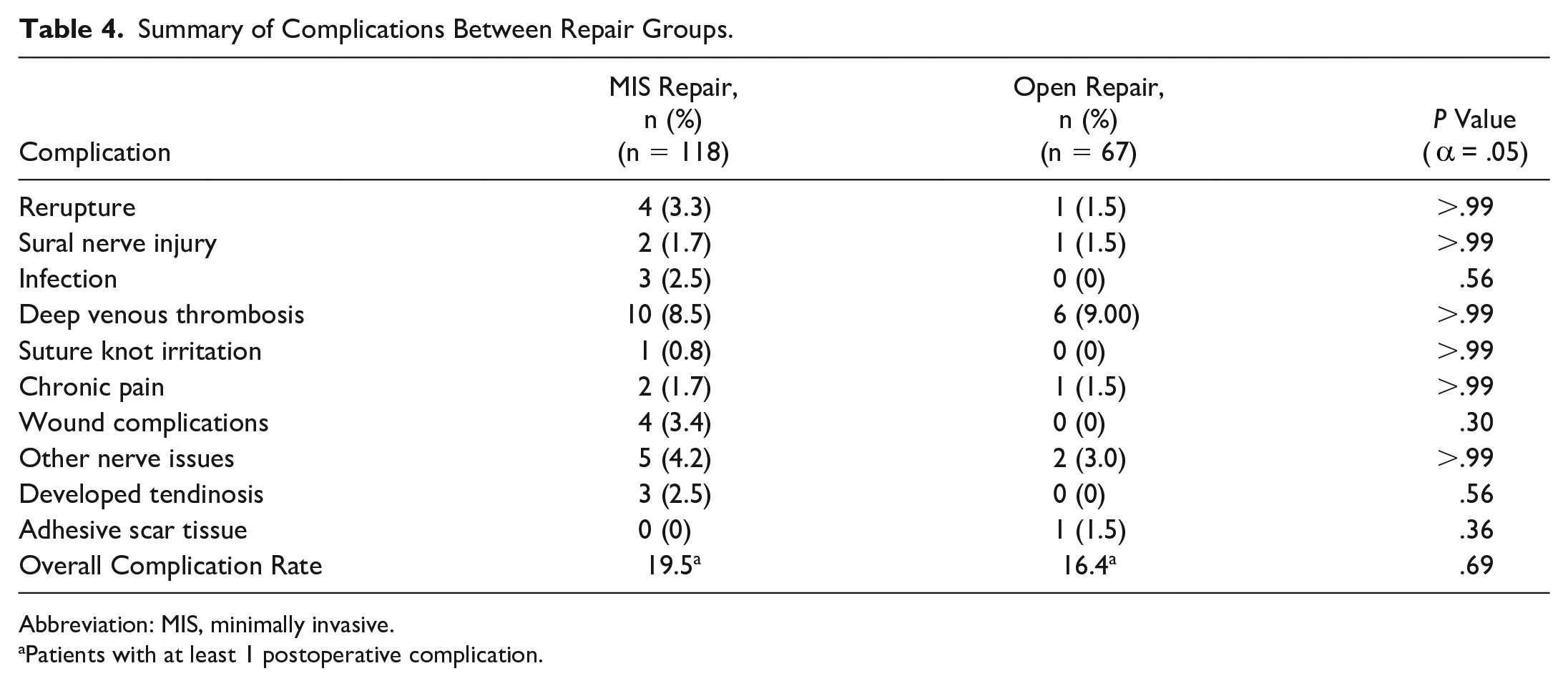
Abbreviation: MIS, minimally invasive.
Patients with at least 1 postoperative complication.
Discussion
Our study examined the differences in patient-reported outcome scores (PROMIS) and complications between open and minimally invasive Achilles tendon repair techniques after acute rupture. The important findings that emerged from this study were that there were no statistically significant differences in patient-reported outcome scores (PROMIS) or complications between the 2 repair techniques, and that patients in both the open and MIS repair groups had improved preoperative to postoperative patient-reported outcomes.
Other outcome scores have been commonly used to compare open and minimally invasive techniques. Multiple studies using outcome scores such as the AOFAS score, the ATRS score, the McComis score, and the Leppilahti score have found good clinical outcomes with no statistically significant differences between open and minimally invasive repair groups.1,4,40 Our study was the first to report PROMIS scores, providing meaningful clinical data about physical function and pain after repair of acute Achilles ruptures. PROMIS scores have been validated in foot and ankle 15 and are now commonly cited in publications. PROMIS scores have also been shown to successfully predict postoperative improvement. 13 There were no statistically significant differences in preoperative and postoperative PROMIS scores between the MIS and open repairs, suggesting that both procedure groups have similar long-term outcomes. Our average postoperative PROMIS scores improved from their preoperative values in both the MIS and the open repair groups. We observed changes in all domains except for Global Mental Health. Overall, we saw an increase in Physical Function postoperatively, with both repair groups having an average PROMIS t score over the population mean of 50. We saw decreases in Pain Interference and Pain Intensity, suggesting that patients had reduction in pain over the long term and had lower scores than the population mean of 50. Lastly, patients reported higher postoperative scores in the Global Physical Health domain and lower scores in the Depression domain.
There were no significant differences in complication rates between the MIS and open repair groups. Previous studies examining complication rates between these 2 techniques have found similar results. For patients with at least 1 complication, we had an overall complication rate of 19.5% in the MIS repair group and 16.4% (P = .69) in the open repair group. Our results indicate higher complication rates than previous studies, which could be due to several factors, including longer recorded follow-up with our patients and differences in defining and recording complications. Prior studies have found that the complication rates for the percutaneous repair and open repair were 5% and 10.6%, respectively. 14 A recent meta-analysis of 2060 patients found that the average incidence of overall major complications from all managements including nonoperative management, minimally invasive technique, and open technique was 9.13%; the mean incidence rate was 5% for rerupture, 1.5% for deep infection, and 2.67% for DVT. 41 Several meta-analyses and studies suggest that patients who underwent minimally invasive techniques compared to open techniques were more likely to report good or excellent results, 11 report triple the satisfaction, 28 have low rerupture rates, 37 good outcomes, and no significant differences in complication rates when compared to an open repair. 14
Historically, rerupture rates have been shown to be similar between open and MIS techniques.9,14,37 This is consistent with the results from our study, as we had 4 reruptures (3.3%) in the MIS group and 1 rerupture (1.5%) in the open group (P > .99). Previous studies have shown rerupture rates ranging from 0% to 3.7% in the percutaneous group and 0% to 2.8% in the open group, with overall rates of rerupture reported around 2.1%.9,14,37
Our study had 2 sural nerve injuries (1.70%) in the MIS group and 1 sural nerve injury (1.50%) in the open group (P > .99). These sural nerve injury rates are lower than studies that used earlier percutaneous techniques such as the Ma & Griffith repair with a 13% rate of sural nerve injury, but similar to more recent studies that show a sural nerve injury rate of 0% to 3.3% in the percutaneous repair and 3% in the open repair.7,8,12,14,20,25,26,37
We describe 4 incidences (3.40%) of wound complications in the MIS group and no wound complications (0.00%) in the Open group (P = .30). Though the difference between groups was not statistically significant, our results differ from other studies that reported variable rates of superficial wound complications ranging from 2.1% to 3.2% in the minimally invasive group and from 4.1% to 20% in the open group.14,28,34,37 This difference is interesting given that the minimally invasive group routinely used incisions less than 4 cm, but could also be due to the open group using an incision that is smaller than most previously reported open Achilles repair incisions.
There were 3 deep infections (2.50%) in the MIS group and no deep infections (0%) in the open group (P = .56). This finding is notable given the incision size of the MIS group, which would provide for less exposed tendon. Our findings are consistent with other studies that have found an infection rate of 0.54% in open repairs, 5 overall infection rates of 1.5% for all managements, 41 and a meta-analysis for percutaneous repairs that found an infection rate of 2.1%. 37
Our study demonstrated 10 incidences (8.50%) of DVT in the MIS group and 6 incidences (9.00%) of DVT in the open group (P > .99), which falls within the reported range in the literature from below 1% up to 50%.2,3,27,29,30,33,37 Procedure duration was the only statistically significant difference found between the MIS and open groups, but only differed by 3.9 minutes on average, which may not factor in the decision to use either technique.
In addition to clinical differences, differences in cost-effectiveness exist between the minimally invasive and open Achilles tendon repair techniques owing to the use of a commercially available minimally invasive device in comparison to an open, suture-based repair. In the current era, surgeons should use cost-effective techniques to minimize the economic burden placed on the health care system. A recent study compared the cost-effectiveness between operative and nonoperative treatment in the setting of acute Achilles tendon rupture and found that nonoperative treatment provided greater benefits and lower costs than operative management. Additionally, another recent study compared the costs of Achilles repair with ring forceps, the Achillon device, and the PARS jig with suture kit, and determined that minimally invasive Achilles tendon repair procedures are more expensive than open Achilles tendon repair procedures. 35 The cost of minimally invasive Achilles tendon repair in our series is likely to be higher given the need to use a commercially available minimally invasive device with similar operative time between groups. 21
Strengths of the present study include our large cohort of patients with a long-term follow-up, with comparable sample size to other retrospective reviews. We also included 9 different foot and ankle fellowship–trained surgeons, which makes our study more generalizable. PROMIS scores have not been previously used in conjunction with complication rates when evaluating the outcomes of Achilles tendon repairs, but these patient-reported outcome scores can provide validated and accurate information to help guide surgical decision making. The use of PROMIS scores allows us to better understand patient outcomes with regard to long-term physical function and pain following operative intervention.
Limitations of our study include the exclusion of 133 patients owing to lack of PROMIS score follow-up at a minimum of 1 year postoperatively, which may affect our results given that we were unable to analyze their PROMIS scores. However, this loss of follow-up has been demonstrated in the literature when using foot and ankle patient outcome registries such as the Orthopaedic Foot and Ankle Outcomes Research (OFAR) network, which reported that at 6 months postoperatively only 56% of patients filled out their outcome scores; we also were able to demonstrate that the excluded patients were not significantly different from included patients on the basis of sex, age, and complication rates. 17 Another limitation is that we did not consider outcomes such as short-term postoperative pain levels, level of sport, or return to sport timeline. We did not use any functional tests such as strength testing or include a control group of nonoperatively treated patients. This study was a retrospective cohort study using a prospectively collected data through our registry and did not include randomization, therefore introducing selection bias.
Future areas of research should include evaluating the return to sport after Achilles tendon rupture and subsequent repair using various operative techniques. Evaluation of short-term postoperative pain levels may also be valuable in understanding differences between the short-term recoveries for both techniques. In addition, further research should be conducted to evaluate intraoperative tensioning and strength of the repair after recovery. Additional randomized controlled trials should also be performed with larger sample sizes to further evaluate MIS and open procedures.
Conclusion
This study demonstrated that there is no distinction between minimally invasive Achilles tendon repair and open Achilles tendon repair in patient-reported outcomes and complication rates.
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Hospital for Special Surgery Institutional Review Board, Study ID: 2013-038
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jonathan T. Deland, MD, reports personal fees from Arthrex. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.