
Abstract
Background:
Nonabsorbable sutures are still the main choice for acute Achilles tendon rupture (AATR) repair due to strength provided. However, the rerupture rates, infection risks, foreign body reaction, and postsurgical recovery differences between absorbable and nonabsorbable suture materials in AATR repair have not been carefully reviewed.
Methods:
A systematic review was done on PubMed, EBSCO, Cochrane Central Register of Controlled Trials, and Embase to find research studies in relation to complications associated with AATR repair using the PRISMA guidelines. The risk of bias from each study included will be assessed using the Cochrane Risk of Bias Tool for randomized study (RoB 2) and Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) for nonrandomized study.
Results:
Five studies with a total of 255 patients, 105 in the absorbable suture group and 150 in the nonabsorbable suture group, were included for analysis. Risk of rerupture, infection, and foreign body reaction shown no significant difference between groups, and the mean difference of recovery scores were similar.
Conclusion:
Existing literature shows that absorbable sutures appear to be associated with similar outcomes to nonabsorbable sutures regarding rates of rerupture, infection, foreign body reaction, and outcomes grading following surgical repair of acute Achilles tendon repair.
Keywords
Introduction
Acute Achilles tendon rupture (AATR) is a common injury that has a substantial impact on a person’s ability to undertake functional activities, particularly in physically active adults. 2 Achilles tendon rupture leads to long-term morbidity, mainly 10% to 30% calf weakness. 2 The primary goals of the management of AATR are to achieve permanent tendon healing at the correct length and to ensure a rapid return to normal function. 16 To date, no clear consensus has been established surrounding the best treatment for AATR. Two main treatments of AATR are surgical vs nonoperative treatment with vigorous debate still ongoing.3,15
Choice of suture material for surgical repair of AATR include several options. Surgeons preference are generally prioritized rather than evidence-based choice of suture. 8 Surgeons are generally more in favor of using nonabsorbable, multifilament sutures, believing that the suture material stays within the repaired tendon and provides adequate fixation power through critical healing period. 1 However, all suture materials can induce an inflammatory reaction with extrinsic scar tissue formation, cause chronic inflammation, and even maintain infection, affecting postoperative outcomes. 1 Absorbable suture material can have initial tendon holding capacity and strength and potentially produce similar postoperative functional outcomes compared to nonabsorbable suture material, 5 and it carries the potential advantage of ultimately being resorbed from the site. 13 The purpose of this study was to perform a systematic review and meta-analysis comparing usage of absorbable and nonabsorbable suture in Achilles tendon repair.
Methods
Eligibility Criteria
The inclusion criteria for this systematic review were (1) clinical trial or cohort study design, (2) reported comparation of absorbable and nonabsorbable sutures in the treatment of AATRs, (3) full-text studies, and (4) available in English. The exclusion criteria were (1) animal studies, (2) cadaveric studies, (3) in vitro studies, and (4) reviews.
Search Strategy, Information Source, and Selection Process
This systematic review is conducted by 2 authors (I.O., A.F.C.) on PubMed, EBSCO, Cochrane Central Register of Controlled Trials, and Embase in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. 11 The search terms were as follows: (Achilles tendon OR tendoachilles OR tendo Achilles OR tendoachillis OR tendo Achillis OR calcaneal tendon OR tendocalcaneus OR tendo calcaneus) AND (treatment OR intervention OR management OR repair) AND (suture OR sutures OR absorbable OR non-absorbable). The titles, abstracts, and full text identified by the search terms were screened according to specific eligibility criteria.
Quality Assessment
The risk of bias from each study included will be assessed using the Cochrane Risk of Bias Tool 6 for randomized study (RoB 2) and Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) 10 for nonrandomized study by 2 authors (I.O., A.F.C.) independently and disagreement were resolved by discussion. Level of evidence was assessed using Levels of Evidence for Primary Research Question by Wright. 17
Data extraction
All baseline demographics data were extracted from included studies, consisting of author names, year of publication, country in which the study was performed, study design, and number of included patients. Collected data are then categorized into open repair with absorbable sutures group and nonabsorbable sutures group. The outcomes collected were scoring and complications related to meta-focus, analysis, including recovery score assessment, infection, foreign body reaction rates, ankle joint limitation, and VAS score to assess pain and are displayed in tables. Infection, foreign body reaction rates, and ankle joint limitation will be assessed categorically whereas the recovery score numerically.
Statistical Analysis
Statistical analyses were performed using RevMan version 5.4 (Cochrane Collaboration). Risk differences and 95% CIs were calculated for dichotomous outcomes and mean differences and 95% CIs were calculated for continuous outcomes. Heterogeneity was evaluated by the chi-square test, which described the percentage of total variation across studies that was due to heterogeneity rather than chance. The random effects model or subgroup analysis would be chosen to perform the meta-analysis if the data were heterogeneous; otherwise, the fixed effects model would be selected. The I2 values were calculated as an objective basis of heterogeneity judgment. The P value from the chi-square test was required to be <.05 and I2 >50%.
Results
Literature Search
A total of 1190 citations from PubMed, 856 from EBSCO, 16 from Cochrane, and 25 from Embase were acquired through the literature search (Table 1). We excluded 296 duplicate citations by using Mendeley duplicate remover. After screening, 1785 citations were excluded. One animal study was excluded. In the end, 5 studies were included in this meta-analysis. Three studies were randomized clinical studies, whereas the other 2 were nonrandomized studies. The PRISMA flowchart of this meta-analysis is displayed in Figure 1. Quality assessment of randomized studies using RoB 2 (Figure 2) and nonrandomized studies using ROBINS-I (Figure 3) concludes low risk of bias in all studies included. A common bias found across articles was the blinding of intervention from the intervener (surgeons), which was impossible. Details of patient’s characteristics and demographics are presented in Table 2.
Keywords Used in Literature Search.


PRISMA flowchart of this meta-analysis.
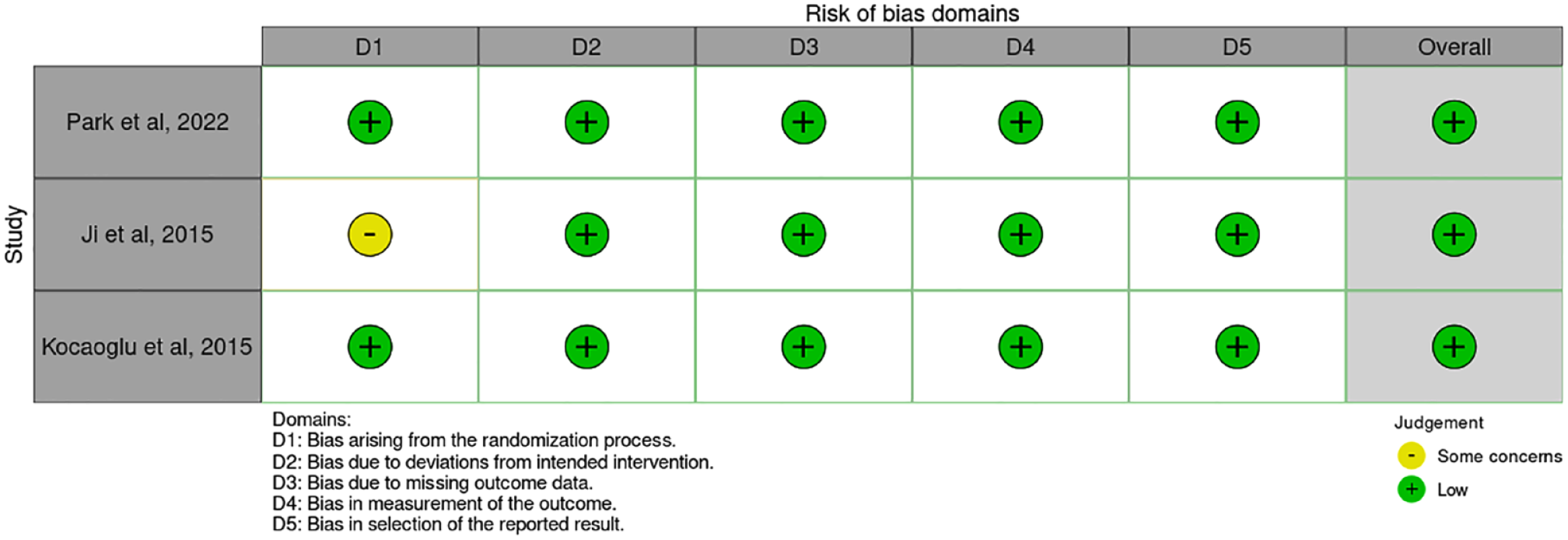
Risk of bias summary using RoB 2.

Risk of bias summary using ROBINS-I.
Characteristics of the Included Studies. a

Abbreviations: NM, not mentioned; N, nonsport injury; RCT, randomize controlled trial; S, sport injury.
Group A = open repair with absorbable suture; group B = open repair with nonabsorbable suture.
Rate of Rerupture
No heterogeneity was found in studies regarding the rate of rerupture (P = 0.96; I2 = 0%), therefore fixed effects model was used. Those in the absorbable suture group did not experience any significant difference on rerupture rate than patients in the nonabsorbable group (risk difference: 0.01, 95% CI −0.04 to 0.06; P = .60) (Figure 4). The percentage of rerupture in the absorbable suture group was 2.33% (2 of 86), and in the nonabsorbable group, 0.76% (1 of 132).

Forest plot showing rerupture rate after repair with absorbable vs nonabsorbable sutures.
Rate of Infection
Fixed effect model was used as no heterogeneity was found in studies of infection rate (P = .86; I2 = 0%). Patients in the absorbable suture group had no significantly different event of infection than patients in the nonabsorbable group (risk difference 0.01, 95% CI −0.06 to 0.08; P = .81) (Figure 5). Infection in the absorbable suture group reached 7.62% (8 of 105) and 8.67% in nonabsorbable group (13 of 150).
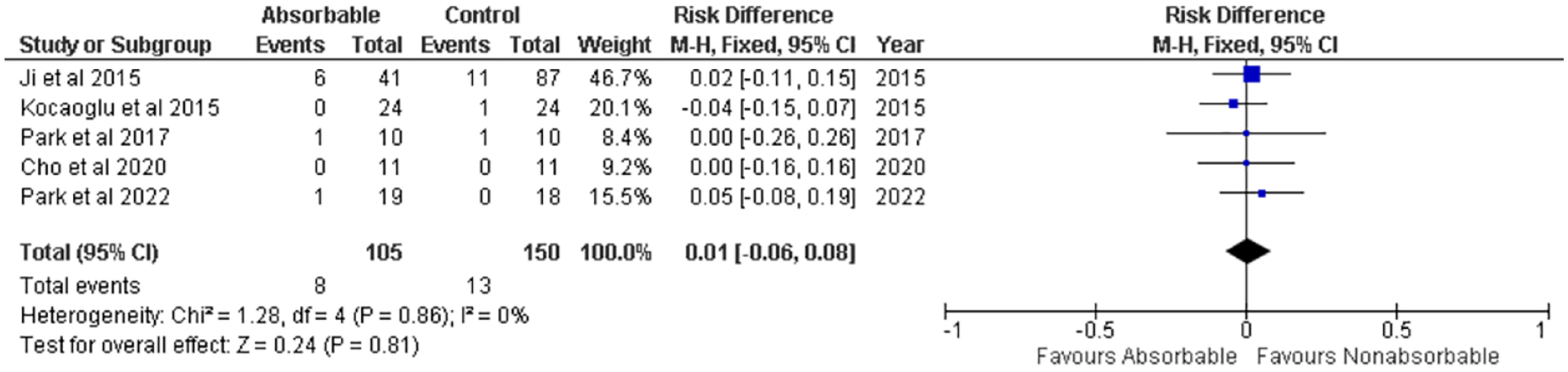
Forest plot showing infection rate after repair with absorbable vs nonabsorbable sutures.
Rate of Foreign Body Reaction
Rates of foreign body reaction in the included studies showed no heterogeneity (P = .62; I2 = 0%); that being the case, fixed effects model was used. Events assessed in Ji et al 6 were adhesion rates resulting from inflammation and the coagulation process. Results showed that patients in the nonabsorbable sutures group had no significantly different foreign body reaction than patients in the absorbable suture group (risk difference −0.02, 95% CI −0.11 to 0.07; P = .69) (Figure 6). Foreign body reaction rate in the absorbable suture group was 8.13% (7 of 86), and in the nonabsorbable group, 12.12% (16 of 132).

Forest plot showing foreign body reaction rate after repair with absorbable vs nonabsorbable sutures.
Difference in Mean Recovery Score
Heterogeneity was seen in studies concerning scoring of recovery in the studies (P = .002, I2 = 82%). The studies mainly use American Orthopaedic Foot & Ankle Society ankle-hindfoot score to evaluate recovery in each patient. Unlike the other included studies, Park et al 14 used Achilles tendon Total Rupture Score (ATRS) and Park et al 13 assessed patients using scoring from Foot and Ankle Outcome Score (FAOS), all recording recovery score of patients after surgery, with scores ranging from 0 to 100 (Figure 7). The mean difference in recovery outcome scores displayed too much heterogeneity to allow pooling of the data.

Forest plot showing recovery score after repair with absorbable vs nonabsorbable sutures.
Discussion
This study was intended to identify potential superiority between absorbable and nonabsorbable sutures used for Achilles tendon repair after rupture. We found that patients in the absorbable suture group experienced no significantly different rerupture rate than patients in the nonabsorbable group. A study of Park et al 14 is that isokinetic plantar flexion strength between the absorbable and the nonabsorbable suture groups showed no significant difference. Despite mechanical studies’ findings that absorbable sutures have a lower load-to-failure property than nonabsorbable sutures over time, the clinical outcomes evaluated in our study for absorbable and nonabsorbable sutures were comparable.
Infection rates in both absorbable and nonabsorbable sutures group were similar. Incidence rate of infection after surgical repair of AATR was reported to be 2% to 3%.7,12 Infections regarding surgery site was known to have several risk factors, including corticosteroid use, smoking, diabetes, and delay in treatment. 12 A study by Jildeh et al 7 showed that those with longer tourniquet times, higher estimated blood loss, and a history of smoking had a higher infection risk.
Our results found no significant differences in the rate of foreign body reaction to absorbable suture group than the nonabsorbable group. Absorbable stitches usually disappear within an average of 3 months. Some reports found foreign body granulomatous reaction associated with nonabsorbable suture material used in AATR repair. 13 Absorbable sutures may allow AATR repair because of its low rate of reaction, especially after absorption. 4 This process is usually delayed in onset and would appear in a few months after the surgery. 9
This study has several limitations. First of all, this study includes nonrandomized studies, which may affect the results. Heterogeneity across study designs and variables also limits performing meta-analysis in difference in recovery. This includes exact suture type and size, repair method, postoperative protocol, intervals, and length of follow-up. Risk ratio of outcomes can be influenced by other nonmodifiable factors including preoperative Achilles tendon status and patient baseline characteristics and comorbidities. Several outcomes are also not fully reported in the selected papers as only some outcomes were recorded, which may be due to the limited number of participants.
Conclusions
The use of absorbable and nonabsorbable sutures seems to have no significant difference in impact regarding rerupture, infection, foreign body reaction rate, and outcome scoring post AATR surgery repair. Further larger prospective studies regarding the outcome of absorbable sutures on AATR are warranted.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231201842 – Supplemental material for Absorbable vs Nonabsorbable Sutures for Achilles Tendon Repair: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114231201842 for Absorbable vs Nonabsorbable Sutures for Achilles Tendon Repair: A Systematic Review and Meta-analysis by Ihsan Oesman and Anissa Feby Canintika in Foot & Ankle Orthopaedics
Footnotes
Appendix
Ethical Approval
Ethical approval was not sought for the present study as this is a systematic review and meta-analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.