
Abstract
Background:
The Broström procedure with suture tape augmentation has become commonplace for surgical treatment of chronic lateral ankle instability. However, there is no consensus among surgeons whether internal bracing of the ATFL alone or a combined ATFL and calcaneofibular ligament (CFL) internal brace produces superior clinical outcomes. This retrospective study aims to investigate whether isolated internal bracing of the ATFL has comparable outcomes to combined ATFL and CFL brace.
Methods:
There were 85 patients from a single tertiary medical center’s electronic medical record identified who underwent an ATFL or ATFL and CFL reconstruction between January 2017 and December 2020. Postoperative outcomes including patient satisfaction, ankle instability, ankle pain, and the need for revision surgery at 1-year follow-up were evaluated.
Results:
Forty-eight patients underwent isolated ATFL reconstruction, and 37 underwent combined ATFL and CFL reconstruction. The choice was made between the 2 options based on surgeon preference. At 1-year follow-up, postoperative outcomes were statistically indistinguishable between the 2 treatment groups.
Conclusion:
The modified Broström reconstruction with ATFL and CFL reconstruction with an internal brace did not produce superior functional outcomes measured at 1 year compared to isolated ATFL reconstruction. Further investigation of long-term functional outcomes is needed to evaluate the long-term efficacy of combined or single-ligament reconstruction.
Keywords
Introduction
Lateral ankle sprains are one of the most common injuries in all levels of sporting activity.7,9 Initial treatment consists of physical rehabilitation; however, up to 20% of individuals may develop chronic ankle instability. 20 Untreated ankle instability may lead to intra-articular pathology such as osteochondral lesions of the talus, loose bodies, impingement, painful ossicles, chrondromalacia, and osteophytes. 10 The Broström procedure was the first anatomic surgical treatment described for lateral ankle instability and consisted of an isolated reconstruction of the anterior talofibular ligament (ATFL).2,3 This technique yielded favorable initial outcomes; however, long-term evaluation of biomechanical and clinical outcomes revealed complications including attenuation of the lateral ligaments, 11 ligament laxity, 12 and long-term ankle instability. 13 Subsequent modifications to the Broström procedure have focused on improving lateral ligament strength, ankle biomechanics, and long-term stability.
The addition of an internal brace to anatomic reconstruction provides a checkrein on the ligament reconstruction, allowing early mobilization and protection of the reconstruction. Suture tape augmentation has gained interest among orthopaedic surgeons because of reports of increased ligament strength and favorable short-term outcomes.4,5,7,8,14,18,19,24 -26 Currently there is no literature directly comparing the use of suture tape augmentation of the ATFL and calcaneofibular ligament (CFL) to augmentation of the ATFL alone. This retrospective study aims to investigate if isolated ATFL reconstruction with suture tape augmentation produces comparable outcomes to reconstruction of both the ATFL and CFL using suture tape.
Methods
Study Design
After institutional review board (IRB) approval, a retrospective chart review was conducted at a single center. All patients who underwent lateral ankle ligament reconstruction with a Broström procedure between January 2017 and December 2020 were evaluated. Patients were included in this study if they had chronic lateral ankle instability and failed conservative treatment and underwent a modified Broström reconstruction of the ATFL with or without the CFL. Diagnosis of lateral ankle instability was established by one of 3 foot and ankle specialists practicing at the study site using a combination of history, physical examination, and advanced imaging. All patients were between the ages of 18 and 80 years at the time of surgery. Patients were not excluded if they underwent a concurrent secondary procedure that included arthroscopy of the ankle or partial excision of the talus, tibia, or fibula. Patients were excluded if (1) the Broström procedure was a revision surgery; (2) they underwent a concurrent secondary procedure other than those previously listed; or (3) follow-up data were unobtainable.
After data collection, all patients who underwent a Broström procedure were subcategorized into those who had suture tape augmentation of the ATFL alone, and those who had augmentation of both the ATFL and CFL. Augmentation of ATFL alone vs both ATFL and CFL was based on surgeon preference. One surgeon performed augmentation of the ATFL alone and 2 surgeons performed augmentation of both the ATFL and CFL.
Broström Reconstruction With Suture Tape Augmentation
Surgery is typically performed on an outpatient basis. Regional anesthesia is provided in the preoperative suite. The patient is positioned supine on a standard operating table. A bump is placed under the hip on the operative side to adequately internally rotate the operative extremity in order to expose the lateral ankle. A tourniquet is applied. If any arthroscopy is indicated, the arthroscopic step of the procedure is completed first. An incision is made over the anterior third of the fibula and extended distally 5 cm in a curvilinear fashion toward the ligamentous structures. Dissection of the subcutaneous tissue exposes the capsular structures that are released in a subperiosteal fashion. The peroneal tendons are exposed and evaluated for any concurrent tendinopathy.
The extra-articular footprint of the ATFL is identified on the talus. The location for the anchor is typically just medial to the remnant of the ATFL insertion on the talus. The location of the CFL anchor is also identified by the CFL remnant on the lateral wall of the calcaneus. This footprint is prepared for FiberTape (Arthrex, Naples, FL) fixation with a suture anchor. The FiberTape is woven through the lateral capsuloligamentous structures. A tunnel is made at the fibula in preparation to dock the internal brace (Figure 1A).

Modified Brostrom ATFL reconstruction with suture tape augmentation. (A) The location for the ATFL and CFL suture anchors are identified and drilled. The suture tape is woven through the lateral capsuloligamentous structures. (B) Location for the fibular tunnel used to dock the internal brace. (C). The internal brace is secured in the fibular tunnel previously made and tensioned with the foot in neutral dorsiflexion and eversion. ATFL, anterior talofibular ligament; CFL, calcaneofibular ligament.
Attention is then directed to the lateral ligament reconstruction. The origin of the ATFL and CFL is identified on the fibula, and 2 suture anchors are placed. The position of the suture anchor is identified just distal to the insertion of the AITFL, approximately 1.5 cm from the tip of the lateral malleolus. The anchor is drilled in an anterior to posterior direction. The CFL anchor is placed approximately 0.5 cm from the fibular tip. Particular care is taken during CFL anchor placement to avoid entrapment of the peroneal tendons. The FiberTape is then woven through the proximal capsuloligamentous structures. With the ankle held in neutral dorsiflexion and slight eversion, the capsular structures are secured with surgical knots. The internal brace is then docked to the fibular tunnel previously made, being tensioned with the foot in neutral dorsiflexion and eversion (Figure 1C). Care is made to not overtension the reconstruction. The construct is then evaluated for stability to varus, valgus stress, and anterior drawer test.
Postoperatively, the patient is placed in a Jones dressing, made nonweightbearing for 2-3 weeks until the surgical wound is healed. The patient is then allowed to weightbear as tolerated in a controlled ankle motion brace and participate in a standardized physical therapy regimen until 2 months when return to sport is permitted.
Outcome Measures
All clinical information was retrospectively obtained from the surgical center’s electronic medical record. Data collected included patient demographics, surgical history, symptom duration prior to surgery, surgical complications, and concurrent secondary procedures. Outcome data were collected at 1-year follow-up in clinic by the same attending surgeon that performed the ligament reconstruction surgery. Part of the surgeon’s assessment included explicit documentation of patient satisfaction postprocedure, ankle pain with physical activity or at rest, and ankle instability either reported by the patient or noted on physical examination. These data were collected by a member of the research team from the surgeon’s electronic health record note into a datasheet. The need for a revision surgery was separately collected from the patient’s electronic health record. Outcome variables were dichotomized as either being present or absent.
Statistical Analysis
Statistical analyses were performed using Excel (Microsoft Corporation, Redmond, WA). Patient samples were evaluated for demographic and postoperative metrics using descriptive analysis. Statistical analyses of univariate continuous outcomes were performed using Student t test, whereas categorical variables were tested using χ2 tests. A P value of <.05 was deemed significant.
The effect size for our categorical outcome variables was calculated using the phi coefficient and interpreted as a small, medium, and large effect sizes corresponding to values of 0.10, 0.30, and 0.50, respectively. Odds ratios with 95% CIs were reported for categorical outcome variables as well. A post hoc power analysis was performed using G*Power (UCLA; Los Angeles, CA).
Results
We identified 389 patients who underwent lateral ankle ligament reconstruction via a Broström procedure between January 2017 and December 2020 and 85 met inclusion criteria. Forty-eight patients (56.5%) underwent isolated ATFL reconstruction and 37 (43.5%) underwent combined ATFL and CFL reconstruction. The mean age among the 2 cohorts was 32.0 (±14.2) years and included 29 males and 56 females. Demographic characteristics including mean age, sex, body mass index, symptom duration prior to surgery, laterality, and comorbidities were not significantly different as summarized in Tables 1 and 2.
Demographics of the Patient Population.

Abbreviations: ATFL, anterior talofibular ligament; BMI, body mass index.
Values are total number or mean ± SD.
Comorbidities in the Patient Population.

Abbreviation: ATFL, anterior talofibular ligament.
All 85 patients had outcome data available at their 1-year follow-up appointment. Forty patients (88.9%) in the ATFL group were satisfied with their surgical outcome compared with 33 patients (89.2%) in the combined ATFL and CFL group (P = .54). Fourteen patients (31%) reported ankle pain in the ATFL group compared with 7 (18.9%) in the combined ATFL and CFL group (P = .32). Only 2 patients (4.4%) in the ATFL group required a revision surgery and 3 (8.1%) required a revision in the ATFL and CFL groups (P = .65). However, 5 patients (11.1%) in the ATFL group experienced recurring ankle instability compared with 0 patients in the ATFL and CFL groups (P = .06) (Table 3).
Patients Receiving Isolated ATFL Reconstruction and Combined ATFL and CFL Reconstruction Stratified by Surgical Outcome.

Abbreviations: ATFL, anterior talofibular ligament; CFL, calcaneofibular ligament.
Discussion
The modified Broström procedure with suture augmentation is an increasingly popular technique for the surgical treatment of chronic lateral ankle instability. Although several studies suggest this technique is safe and effective, there is a paucity of data directly comparing outcomes of isolated ATFL suture augmentation to combined ATFL and CFL augmentation.6 -8,11,15,17,20,21,23,25 Our results suggest modified Broström reconstruction of the ATFL and CFL did not produce superior functional outcomes measured at 1 year compared with reconstruction of the ATFL alone. No significant difference was found between isolated ATFL and combined ATFL and CFL suture augmentation regarding patient satisfaction, recurring ankle pain, recurring ankle instability, and the need for a revision surgery at 1-year follow-up.
The P value for recurring ankle instability (0.06) trended toward significance, which may be clinically important. Eight patients in the isolated ATFL cohort and 4 patients in the combined ATFL and CFL cohort were not satisfied with their surgical outcome. There was no significant difference between the 2 cohorts concerning sex, age, BMI, comorbidities, and duration of symptoms prior to surgery on post hoc analysis.
According to a recent systematic review by Lewis and colleagues, there are 10 studies that report clinical or functional outcomes of the modified Broström reconstruction with suture augmentation of the ATFL alone or both ATFL and CFL. 18 Five of the 10 studies reported outcomes comparable to ours. The rate of recurrent ankle instability in patients who underwent isolated ATFL reconstruction ranged from 3.3% to 13.6% compared with 4.2% to 7.1% in combined ATFL and CFL reconstruction.4,5,24,26 In patients with isolated ATFL reconstruction, 11.6% required a revision surgery vs 4.2% in patients with combined ATFL and CFL reconstruction.4,8 Our reported incidences of recurrent ankle instability (11.0% ATFL vs 0.0% ATFL and CFL) and revision procedure (4.4% ATFL vs 8.1% ATFL and CFL) as well as those reported in the literature suggest isolated ATFL reconstruction with suture augmentation generally can achieve a substantial degree of ankle stability and satisfactory functional outcomes.
Several clinical studies have reported functional outcomes of modified Broström reconstruction of isolated ATFL and combined ATFL and CFL without suture augmentation. Reconstruction of the ATFL alone has shown good outcomes with return to sports rates between 93% and 100%1,15,17,22 vs 91% to 94%21,23 in combined ATFL and CFL reconstruction.
A cadaveric study by Lohrer and colleagues evaluated ankle biomechanics in cadavers who underwent either isolated ATFL or combined ATFL and CFL reconstruction with suture augmentation. There was no significant difference in anterior translocation during anterior talar drawer test. 19 Another cadaveric study evaluating ankle biomechanics compared ATFL with or without CFL reconstruction and demonstrated there was no significant difference in anterior displacement or varus tilt angle between the 2 treatment groups. 16 Again, this suggests isolated internal bracing of the ATFL may provide a similar degree of lateral ankle stability compared to a combined augmentation of both the ATFL and CFL. The similar clinical, functional, and biomechanical outcomes between isolated ATFL and combined ATFL and CFL reconstruction in the literature suggest concurrent internal bracing of the CFL with the modified Broström procedure using suture augmentation may not be necessary.
Omitting CFL reconstruction may benefit both surgeons and patients. The cost of a single Arthrex suture tape kit is $1500, and performing only isolated ATFL reconstruction may reduce implantation cost. Single ligament reconstruction also decreases surgical time16,19 and allows for a smaller surgical incision, which limits surgical exposure and retractor use, decreases risk of superficial nerve injury, shortens postoperative recovery time, and reduces immediate postoperative pain. 16
The present study has several limitations that include the retrospective nature of the study, data collection at a single center, and relatively short-term follow-up. Our patient population was evaluated and operated on by 3 different foot and ankle–trained orthopaedic surgeons. However, the diagnostic criteria of chronic lateral ankle instability, and patient rehabilitation program were the same for all patients. Patients who underwent concurrent procedures other than arthroscopy of the ankle or partial excision of the talus, tibia, or fibula were excluded, limiting the study’s generalizability and potentially excluding patients with poor prognostic factors. However, this may provide some clinical utility in selecting patients for modified Broström reconstruction of the lateral ankle ligaments.
Another limitation of our study is the sample size. We included 85 patients total between the 2 cohorts. The effect size for each outcome variable was calculated using the phi coefficient (Table 4). No value was greater than 0.3, indicating a small effect size for each outcome variable. A post hoc power analysis revealed our study would require at least a few hundred additional patients to achieve a power of 80% with alpha equaling 0.05 (Table 4). Despite the limitations of this study, it is the first to directly compare clinical outcomes of patients undergoing isolated or combined lateral ligament internal brace augmentation at a single center.
Effect Size and Post Hoc Power Analysis for Each Outcome Variable.
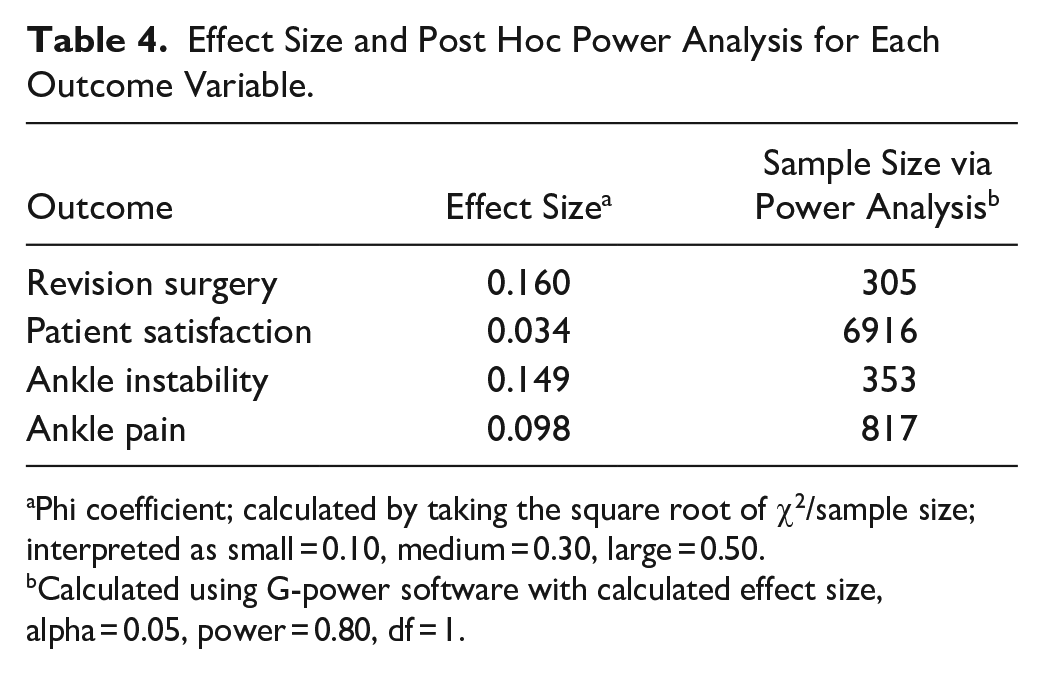
Phi coefficient; calculated by taking the square root of χ2/sample size; interpreted as small = 0.10, medium = 0.30, large = 0.50.
Calculated using G-power software with calculated effect size, alpha = 0.05, power = 0.80, df = 1.
Conclusion
The modified Broström reconstruction with suture tape augmentation of both the ATFL and CFL did not produce superior functional outcomes measured at 1-year follow-up compared to isolated ATFL internal brace augmentation. Several studies independently investigating isolated ATFL or combined ATFL and CFL internal bracing yielded similar clinical and functional results at short-term follow-up, suggesting concurrent reconstruction of the CFL may not be necessary. Further investigation in randomized controlled trials of long-term functional outcomes is needed to evaluate the long-term efficacy of combined vs single lateral ligament augmentation.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231185071 – Supplemental material for Isolated Anterior Talofibular Ligament (ATFL) vs Combined ATFL and Calcaneofibular Ligament Suture Tape Augmentation for the Treatment of Lateral Ankle Instability: Are Outcomes Equivalent?
Supplemental material, sj-pdf-1-fao-10.1177_24730114231185071 for Isolated Anterior Talofibular Ligament (ATFL) vs Combined ATFL and Calcaneofibular Ligament Suture Tape Augmentation for the Treatment of Lateral Ankle Instability: Are Outcomes Equivalent? by Zachary Troiani, Michael Harrington, Afshin Anoushiravani, Jetha Tallapaneni, Andrew Salgado and Andrew Rosenbaum in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the Albany Medical Center Committee on Research Involving Human Subjects IRB (6165).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew Rosenbaum, MD, reports other financial or nonfinancial interests: consultant for Arthrex. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.