
Abstract
This is a visual representation of the abstract.
Keywords
Introduction
Acute lateral ankle sprains are the most common sports injury. 8 Many of the injured patients recover with conservative treatment; however, up to 40% of them progress to chronic lateral ankle instability requiring surgical stabilization. 1
Surgical treatment for chronic ankle instability is controversial regarding approach (open vs arthroscopic), technique (repair vs reconstruction), indications, and timing, yet the Broström-Gould procedure remains the gold standard and first-line surgical treatment.1,8 New trends advocate arthroscopic repair of the anterior talofibular ligament (ATFL) when the ligament remnants are competent, showing satisfactory outcomes, and anatomic reconstruction with tendon autograft when ligament remnants are insufficient or in a combined calcaneofibular ligament (CFL) injury.1,2,8
Recently, ATFL remnant quality has been the subject of study when defining the best approach, 2 but the ideal graft and preparation technique is yet unknown. 5 Lopes et al 7 combined arthroscopic ATFL and CFL reconstruction technique implements a 10-cm gracilis autograft, harvested using a tendon stripper through a short oblique incision, in which both ends are threaded with FiberLoop No. 2 (Arthrex, Naples, FL) and placing one of them through a 4.75- × 15-mm Bio-Tenodesis Screw system (Arthrex) for fixation to the talus. This study aims to describe a modified gracilis autograft preparation for the arthroscopic ATFL and CFL reconstruction as described by Lopes et al. 7
Material and Methods
Indication
The ideal candidates for this technique are active patients with combined ATFL and CFL tears confirmed on MRI and presenting as chronic lateral ankle instability and failure of a conservative treatment trial for a minimum of 6 months. Patients with isolated ATFL injury with a suspected poor remnant quality may also be eligible based on the recurrence of ankle sprains.
Operative Technique
Setup
The patient is placed supine with a pillow under the ipsilateral buttock to position the lower limb in internal rotation and allow access to the anterior and lateral ankle (Figure 1). The contralateral lower limb is abducted or lowered for accessible and comfortable arthroscopic instrument use. A lateral support is positioned at the level of the lateral thigh to hold the knee flexion for gracilis tendon harvesting.

Patient setup for the arthroscopic ATFL and CFL reconstruction.
Gracilis tendon graft harvesting and preparation
After sterile draping, a 2- to 5-cm vertical incision centered on the distal hamstring insertion is performed for gracilis harvesting, preserving its distal attachment (Figure 2). Contrary to the original technique, only the proximal end of the gracilis tendon is sutured with Vycril 2 (Ethicon, Cincinnati, OH) in a whipstitch pattern before sharply detaching its distal end for a fast and easy graft preparation. Similar allograft preparation can be achieved if preferred.

Gracilis autograft harvesting approach.
Arthroscopic portals, footprint preparation, and tunnel drilling
Arthroscopic portals, footprint preparation, and tunnel drilling follow the original technique. 7
Graft passage and tensioning
The distal end (thickest) of the gracilis tendon is secured to a 4.75-mm SwiveLock (Arthrex) Bio-Tenodesis Screw by substituting the default sutures for a FiberLink (Arthrex) (Figure 3) and fixed into the talar tunnel (Figure 4). The FiberLink (Arthrex) is then cut at its emergence from the talar tunnel, and the graft fixation is tested by pulling it. An UltraButton (Smith & Nephew) adjustable suture-button system is placed around the graft, and the distal end of the graft is routed between the peroneal tendons and the lateral calcaneus cortex, exiting through the retromalleolar calcaneal incision and then through the calcaneal tunnel with the aid of guiding sutures (Figure 5). Likewise, the UltraButton (Smith & Nephew) adjustable suture-button system is pulled into the fibular tunnel with a guiding suture.
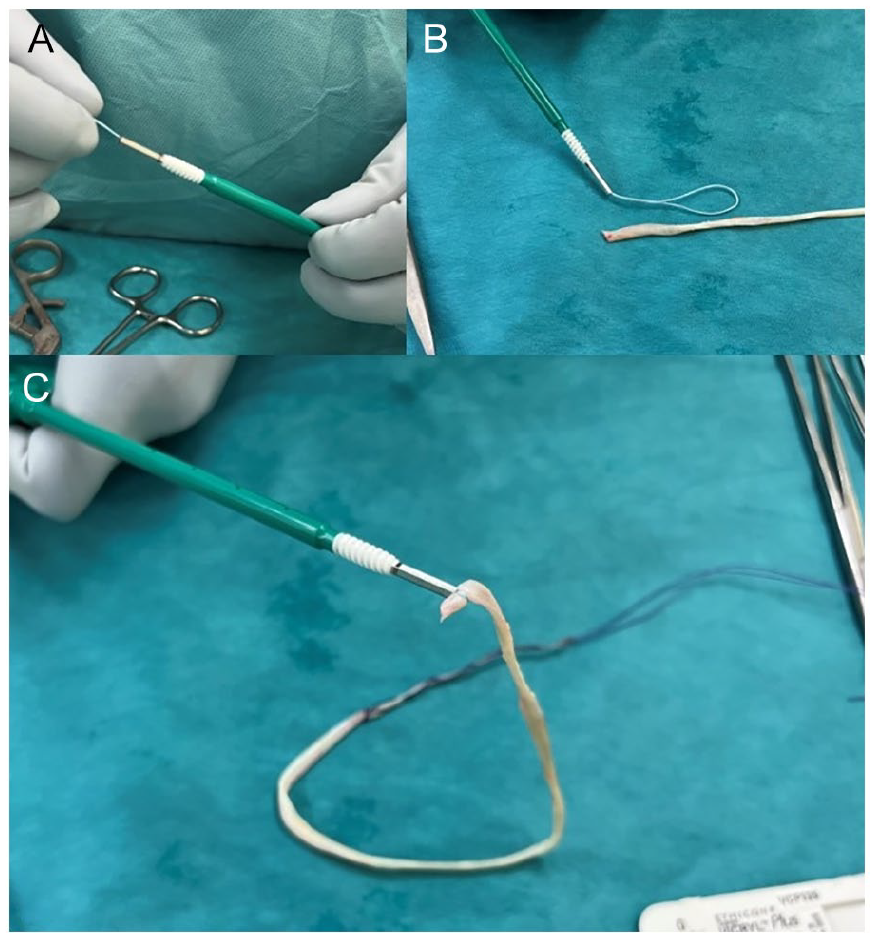
(A) Progressing the suture loop inside the Bio-Tenodesis Screw System; (B) suture loop ready in the distal Bio-Tenodesis Screw System; and (C) the distal end (thickest) of the gracilis tendon is secured to the Bio-Tenodesis Screw System with the suture loop.

Arthroscopic view of the talar fixation of the gracilis autograft using the SwiveLock (Arthrex) Bio-Tenodesis Screw.

The proximal end of the gracilis autograft after exiting medially through the calcaneal tunnel. Note that only that end was whipstitched during graft preparation.
Under arthroscopic visualization from the anteromedial portal and plantigrade position, 1 cm of the graft is gradually progressed into the fibular tunnel. The graft is fixed in the calcaneal tunnel with a 6 × 20-mm interference screw while maintaining the foot plantigrade position, and additional tension tuning can be achieved by tightening the UltraButton (Smith & Nephew) adjustable suture-button system.
Postoperative Treatment
Patients are allowed to bear total weight as tolerated with a walker-type boot for 15 days. Rehabilitation for ankle strengthening, pain-guided active range of motion exercises, and proprioception training start from day 8. Patients start jogging, running, and vertical jumping in the sixth week, progressing to uneven and unstable surfaces accordingly. Return to sports is allowed at 6 months.
Discussion
Different ATFL and CFL graft alternatives have been implemented in the ATFL and CFL reconstruction with satisfactory outcomes. Wang and Xu, 9 in a retrospective case series of 25 patients undergoing a fluoroscopy-guided minimally invasive reconstruction with semitendinosus autograft, reported excellent satisfaction in 80% of patients and significant AOFAS score improvement (from 71.1 to 95.1) at a mean 32.3-month follow-up. Jung et al, 4 in a prospective study including 66 patients undergoing open reconstruction using semitendinosus allograft, reported a significant mean VAS pain score reduction (from 5.5 to 1.3) and AOFAS and Karlsson-Petersen score improvement (from 71.0 to 90.9, and 55.1 to 90.3, respectively) at a mean 22.1 months, and finding no clinical differences between pretensioning the graft or not. Similarly, Lopes et al, 6 in a prospective study including 171 patients undergoing arthroscopic reconstruction with gracilis autograft, reported high patient satisfaction and significant AOFAS and Karlsson score improvement (from 61.7 to 87.6 and 54.7 to 85.2, respectively) at a mean 9.6-month follow-up.
Anatomical studies have suggested that the semitendinosus tendon graft is closer to the ATFL diameter than the gracilis, 5 yet no graft option has been proven clinically superior. Moreover, several graft configurations, such as the Y configuration by Guillo et al 1 and the triangular-shaped (ALC-triangle) by Higashiyama et al, 3 have been described as suitable alternatives for ATFL and CFL reconstruction.4,7,9
The presented technique allows an easy and fast graft preparation by suturing the proximal end of the gracilis and leaving its thicker end for ATFL reconstruction with a Bio-Tenodesis Screw. This avoids the need to suture both graft ends, measure the graft, and/or make technically demanding graft configurations, potentially saving valuable time. The authors have performed this technique on 12 professional athletes participating in pivoting sports (10 males and 2 females), achieving excellent scores in “activities of daily living” and “sports” subscales in the Foot and Ankle Ability Measure (FAAM) at the 3-month follow-up and return to sports before the recommended time at a mean of 4 months after surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241242780 – Supplemental material for Modified Gracilis Autograft Preparation for Arthroscopic Anterior Talofibular and Calcaneofibular Ligament Anatomic Reconstruction: Technical Tip
Supplemental material, sj-pdf-1-fao-10.1177_24730114241242780 for Modified Gracilis Autograft Preparation for Arthroscopic Anterior Talofibular and Calcaneofibular Ligament Anatomic Reconstruction: Technical Tip by Bruno C. R. Olory, Theodorakys Marín Fermín, Pieter D’Hooghe, Emmanouil Papakostas, Khalid Al-Khelaifi and Bashir A. Zikria in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
No ethics approval was required for the presented study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent for publication was obtained from the patient/parent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.