
Abstract

Introduction
Allograft and autograft interposition wedges have been used for the treatment of metatarsophalangeal joint nonunions, failed joint arthroplasties, ailed hallux valgus correction, and infections.3,4 These procedures are complicated by nonunion rates of up to 21%, and the requirement for bony surfaces with appropriate bone stock to create a good fit on both the proximal phalanx and metatarsal head with the allograft/autograft wedge.2,6,7
When there is a lack of distal bone stock and/or the bone contours may not allow for adequate shaping for a good fitting graft, it may lead to higher rates of nonunion. 5 The surgeon is then left with the need to consider increased shortening of the first ray, which can lead to worse outcomes.3,7 The Masquelet technique has been widely used for large bone defects, especially when the area needs structural support and biomembrane formation to improve the natural process of healing. 8 In this surgical technique, we combined both a Masquelet technique followed by impaction bone grafting with proximal tibial bone graft and allograft bone with 90/90 mini-fragment plating when faced with significant bone loss to avoid the need for further shortening.1,8 The utilization of 90/90 plating creates a rigid construct compared to uniplanar plating and has shown excellent results when used in first metatarsal phalangeal joint arthrodesis when bone loss is present. 1 This allows for not only adequate grafting but also robust fixation when minimal distal bone stock is present.
Methods
Patients were treated from May 2020 to May 2021. Surgical indications are in Table 1. All patients were evaluated preoperatively with radiography, MRI, and CT imaging.
Patient Case-Specific Surgical Indications.

Case Example
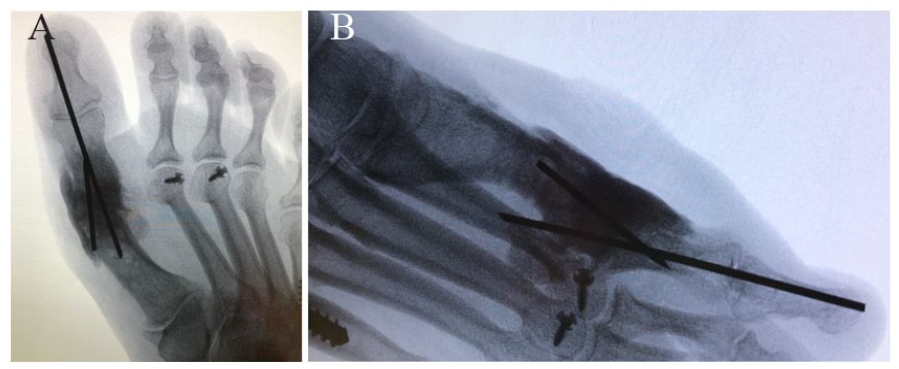
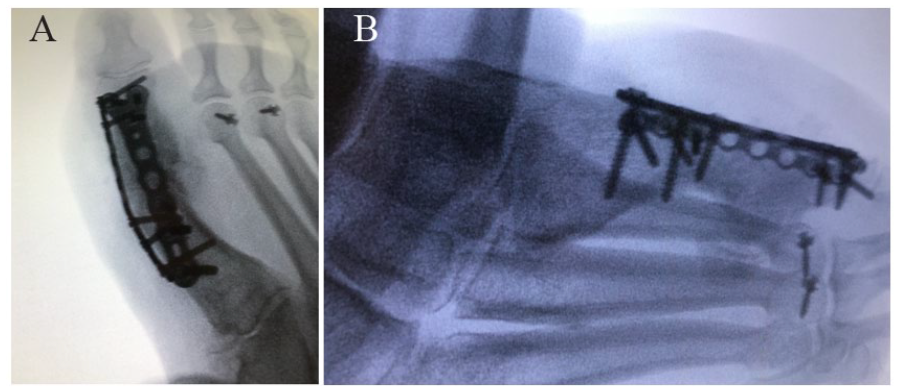
A 47-year-old female with failed hallux valgus correction underwent a hallux MTP fusion. This resulted in a nonunion and she was revised with an allograft bone block distraction arthrodesis. This resulted in a nonunion and hardware failure (Figure 1). She underwent a Masquelet technique with impaction bone grafting with 90/90 plating. Final weightbearing post operative radiographs are presented in Figure 2.

Anteroposterior (A) and lateral (B) radiographic views of right foot showing broken hardware with fragmented allograft bone block in failed revision metatarsophalangeal fusion.

Final weightbearing (A) anteroposterior and (B) lateral radiographic views after revision first metatarsophalangeal joint fusion with staged Masquelet technique and impaction bone grafting with 90/90 plating.
Operative Technique
In the first stage of the procedure previous hardware and all nonviable tissue including dead bone or allograft bone are removed (Figure 3). Soft tissue and bone samples are sent to microbiology and pathology. Next, we reduce the hallux in the appropriate position in terms of dorsiflexion and coronal alignment and then place K-wire fixation (Figure 4). Next, an antibiotic cement spacer preloaded with 0.5 g of gentamicin (Rafobacin high-viscosity Bone Cement R; Zimmer Biomet) is hand-mixed with 1 g of vancomycin. The cement spacer is placed in the defect and placed over the bone to cover the edges dorsally and medially by at least 5 mm to help create a healthy membrane around the defect (Figure 5). At this time, final fluoroscopic images are taken to show appropriate position of the cement spacer and hallux (Figure 6). Postoperatively, the patient is placed in a splint for 2 weeks and then transitioned to a nonweightbearing controlled-ankle motion boot until definitive surgery.

(A) Anteroposterior and (B) lateral radiographic views showing large defect after bone debridement in the first stage of revision. (C) Intraoperative photograph showing removal of allograft wedge and dead bone with healthy remaining tissue.

K-wire fixation showing appropriate alignment of the hallux metatarsophalangeal joint.

Antibiotic cement spacer placement.
Final (A) anteroposterior and (B) lateral radiographic views showing appropriate placement on antibiotic spacer and Kirschner wires.
The second stage of the procedure could commence once cultures and pathology were negative for infection/osteomyelitis, or the infection was treated with intravenous antibiotics and patient deemed cured. The surgical incision from the previous procedure is utilized. A robust membrane is often formed by the Masquelet technique. The antibiotic spacer is identified and removed along with any K-wires. A rongeur and drill were used to expose healthy bleeding cancellous bone, both on the proximal phalanx and the remaining metatarsal head. At this time, the toe is then reduced in the appropriate alignment and held with a K-wire (Figure 7). Next, approximately 20 mL of proximal tibia bone graft is harvested and mixed with a combination of 10 mL of allograft bone (Bio4; Stryker, Kalamazoo, MI) and 3 mL of synthetic platelet-derived growth factor (Augment; Stryker). The selection of PDGF over other biologics is by the surgeon’s preference and is used given the multiple prior surgical failures to try and augment the healing potential. At this time, a dorsal locking plate (Variax 2; Stryker) is used to hold out the length of the first ray, and then impaction bone grafting is performed (Figure 8). Then a medial-based locking plate (Variax 2; Stryker) is placed to complete the 90/90 plating construct (Figure 9).

Fluoroscopic image showing removal of antibiotic spacer and reduction of hallux metatarsophalangeal joint with K-wire prior to bone grafting and plate fixation.

(A) Anteroposterior and (B) lateral radiographic views show reduction of hallux with K-wire and dorsal locking plate prior to impaction bone grafting. (C) Anteroposterior and (D) lateral radiographic views of the hallux after impaction bone grafting.
(A) Anteroposterior and (B) lateral radiographic views showing final intraoperative construct.
Postoperatively, the patient is placed in a splint nonweightbearing and then transitioned to a short leg nonweightbearing cast for 4 weeks. At 6 weeks, they were transitioned to a nonweightbearing controlled-ankle motion boot. Progressive weightbearing protocol was implemented at 10-12 weeks in a controlled-ankle motion boot, with transition to regular shoe at 12-14 weeks.
Discussion
Severe bone loss after failed hallux MTP joint surgery can present as a complicated problem and often involve using an allograft bone block arthrodesis with a nonunion rate reported up to 21%. 6 Therefore, we combine a Masquelet technique with impaction bone grafting to improve the biology of the area to try and minimize the rate of nonunion while still allowing for appropriate length of the first ray.
All 3 patients had 1-year follow up with 100% fusion rate. Fusion rate was assessed on weightbearing AP, lateral and oblique radiographs of the foot and clinical examination. At final follow-up, none of the patients reported pain in the surgical area, and they were all back to wearing regular shoes. There were no infections, revision surgeries, or hardware failure. One patient did develop postoperative metatarsalgia at 5 months but it resolved when she transitioned to a regular shoe with an insert. The overall time to weightbearing was on average 10.3 weeks. Patient satisfaction was excellent in all 3 cases. There was well-maintained length with average shortening of 0.16 cm compared to the preoperative state (Table 2). Two cases resulted in shortening, and 1 case was lengthened. Limitations of the study include the small sample size and the usage of augment; however, because of failed previous surgeries, this was used to try and help improve the fusion rate.
First Ray Length, Preoperative vs Postoperative.

Our described technique demonstrates safety, efficacy, and reliability for failed first metatarsophalangeal procedures with large bone loss as an alternative to allograft bone block distraction arthrodesis. Prospective randomized studies should be done to further validate this surgical option as a treatment alternative to bone block distraction arthrodesis.
Footnotes
Ethical Approval
Institutional review board application was completed and submitted, and the committee exempted the study (project 1917040-1).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.