
Abstract
Background:
Studies on decompression metatarsal osteotomy without cheilectomy for hallux rigidus are limited. This study aimed to review the data of patients who underwent this surgery for all grades of hallux rigidus.
Methods:
The medical records of patients who underwent this surgery between August 2017 and January 2021 were retrospectively reviewed. The outcomes were assessed using the visual analog scale (VAS), the Japanese Society for Surgery of the Foot (JSSF) score, and the hallux dorsiflexion angle. Patients who were followed up for more than 2 years were included. The plantar shift of the first metatarsal head (PS) and the shortening of the first metatarsal (SH) were measured to supplementally investigate the associations with other measurements.
Results:
A total of 76 patients (female, 42; male, 34; mean age, 60.3 years; mean body mass index, 23.1) with 80 feet were enrolled. Six patients (7.5%) were grade 1, 20 (25.0%) were grade 2, 30 (37.5%) were grade 3, and 24 (30.0%) were grade 4. The mean follow-up duration was 3.5 years. Overall, the mean VAS score improved from 63.2 to 6.2, the mean JSSF score from 59.0 to 82.6, and the mean dorsiflexion angle from 37.3 to 56.3 degrees. These measures improved for all grades, but the dorsiflexion angles and JSSF scores decreased as the grade advanced. No clear associations were found between the postoperative VAS and the PS and SH. Eight patients (10.5%) had complications: 4 (5.2%) had occasional plantar discomfort under the metatarsal head, 2 (2.6%) required shoe modification, 1 (1.3%) had wound pain, and 1 (1.3%) experienced breakage of a K-wire.
Conclusion:
The VAS scores, dorsiflexion angles, and JSSF scores improved for all grades of hallux rigidus within a relatively short period of follow-up; however, the dorsiflexion angles and JSSF scores decreased as the grade advanced.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Hallux rigidus is defined as degenerative changes in the first metatarsophalangeal joint, characterized by limited dorsiflexion of the hallux. Conservative treatment, such as medication, shoe modification, orthotics, physical therapy, injections (steroids or hyaluronic acid), manipulation under anesthesia aiming at breakdown of intraarticular adhesions, 25 and proliferation therapy (growth factor injection) 8 can be used as first-line treatment, 10 but if the condition fails to respond to conservative treatment, surgery is considered. The surgical treatments reported to date include cheilectomy, osteotomy of the proximal phalanx, osteotomy of the metatarsal (closing wedge or decompression), sesamoidectomy for releasing flexor hallucis brevis spasm and the fibrous ankylosis between the sesamoids and the metatarsal head, cartilaginous replacement (synthetic cartilage implant), arthroplasty (resection, joint replacement, or interposition), and arthrodesis.6,24,26
Decompressive metatarsal osteotomy for hallux rigidus is osteotomy that moves the metatarsal head plantar-proximal, loosening the flexor hallucis longus and brevis tendons, and thus allowing less pressure on the dorsal articular surface when pushing off during gait. Although decompressive osteotomies have reported good outcomes, the grades of articular involvement for which the procedure was applied were diffuse and have not been established.1,2,4,7,11,12,18 -20,22,23,27,28 Moreover, those osteotomies were combined with cheilectomy; therefore, it was unclear whether the good outcomes were due to metatarsal osteotomy or cheilectomy. 21
To our knowledge, there has been only 1 case series study on patients with hallux rigidus who underwent decompressive metatarsal osteotomy without cheilectomy (Figure 1). 15 This study suggested that decompressive metatarsal osteotomy itself is effective for hallux rigidus, independent of a cheilectomy. Moreover, the study reported that decompressive metatarsal osteotomy provided good outcomes for all grades of hallux rigidus. However, the study reported the frequent occurrence of occasional postoperative plantar discomfort under the metatarsal head (28%). That may be because only 1 K-wire was used and the K-wire was placed longitudinally as a blocking pin on the metatarsal head (Figure 1C). In such a method, when the dorsal exostosis is large, the metatarsal head is shifted too plantar, which may cause postoperative plantar discomfort. Therefore, the author hypothesized that another fixation technique using K-wires could better control the position of the metatarsal head and lower the rate of postoperative plantar discomfort.

Radiographs showing sliding oblique metatarsal osteotomy fixated with a K-wire without cheilectomy. (A) Anteroposterior view. A K-wire was located along the extensor hallucis longus tendon. (B) Lateral view. A good example. The K-wire functioned as a blocking pin to the metatarsal head. The osteotomy site was not widened. (C) A bad example. The metatarsal head was lowered too much. It is difficult for one K-wire as a blocking pin to control the amount of the shift of the metatarsal head when the dorsal exostosis is large.
The aim of this study was to retrospectively review a case series of patients with hallux rigidus who underwent an oblique metatarsal osteotomy, fixated with K-wires, without cheilectomy, to assess whether the procedure was effective for all grades of hallux rigidus.
Materials and Methods
The medical records of patients with hallux rigidus who underwent surgical treatment after not responding to more than 3 months of conservative treatment between August 2017 and January 2021 were retrospectively reviewed. All these patients underwent sliding oblique metatarsal osteotomy fixated with K-wires, without cheilectomy, as described below, and no other procedures were performed. In this study, the patients who were followed up for more than 2 years were included, and patients who had less than 2 years of follow-up were excluded.
Surgical Procedure
All the operations were performed by the author. The patients were placed in a supine position. The surgeon positioned himself on the opposite side of the foot to be operated on. A thigh tourniquet was applied. The foot for operation was placed on the table with the lateral side down. A 1.5-cm skin incision was made on the medial side of the first metatarsal neck with a dorsal distal-proximal plantar 60-degree inclination to the metatarsal axis, and blunt dissection was performed to expose the metatarsal neck (Figure 2A). The periosteum was cut and denuded for osteotomy, and osteotomy was performed in the same direction as the skin incision under fluoroscopic guidance (Figures 2B and 3A). A flat chisel was introduced into the osteotomy site and twisted to make the metatarsal head easily mobile, which enabled the metatarsal head to easily slide 3 to 4 mm down (Figure 2C). First, the 2 osteotomized bone fragments of the first metatarsal were fixated obliquely with a 1.8-mm K-wire. Second, the proximal fragment and the second metatarsal, and finally the capital head and the second metatarsal head, were fixated transversely with 1.8-mm K-wires (Figures 2D, 3B, and 4). The K-wires were bent and cut. The skin was sutured with 5-0 nylon. The protruding K-wires were fixated with Steri-Strip (3M, St Paul, MN), wrapped with strips of gauze, and covered with a film (Figure 2E).

Intraoperative photographs. (A) The position of the operated foot and the planned skin incision. The foot was placed on the table with the lateral side down. A 1.5-cm planned skin incision with a 60° inclination to the metatarsal shaft was marked using a surgical pen under fluoroscopic guidance. (B) Osteotomy. The osteotome was set in the same direction as the skin incision. The assistant stabilized the foot. (C) A flat chisel was introduced into the osteotomy site and twisted to make the metatarsal head easily mobile. (D) Fixation using K-wires. The metatarsal head was slid 3-4 mm down along the osteotomy site. First, the two osteotomized fragments; second, the metatarsal head and the second metatarsal; and finally, the first metatarsal shaft and the second metatarsal, were fixated with 1.8-mm K-wires. (E) Postoperative dressing. The protruding K-wires were bent and cut, fixated with Steri-Strip™, wrapped with strips of gauze, and covered with a transparent film.

Intraoperative fluoroscopy. (A) Osteotomy. A perfect lateral view was obtained, and the blade of the osteotome was set at the metatarsal neck with a 60° inclination to the metatarsal shaft. (B) Fixation using a 1.8-mm K-wire. The metatarsal head was slid 3-4 mm down. The K-wire was about to fixate the osteotomy site.

Postoperative radiographs. (A) Anteroposterior view. Two 1.8-mm K-wires penetrated the 1st and 2nd metatarsals and a third 1.8-mm K-wire penetrated the osteotomized fragments. (B) Lateral view. The osteotomy line demonstrated a 60° inclination to the long metatarsal axis. The metatarsal head slid down approximately 4 mm.
Postoperative Care
Full weightbearing, with postoperative shoes (DARCO OrthoWedge Shoe; Huntington, WV) that restricted forefoot weightbearing, and active range of motion exercise of the hallux were initiated 1 day after surgery. 15 The K-wires and the nylon sutures were removed 4 weeks after surgery. Full weightbearing, without the postoperative shoes, was initiated 6 weeks after surgery. Sport activities were initiated 10 weeks after surgery, as tolerated.
Data Collection
Informed consent for the use of the data in the medical records was obtained from all patients before surgery. 13 The data for analysis included sex, age, and body mass index at the time of surgery, visual analog scale (VAS, 0-100 mm) for rating pain, Japanese Society for the Surgery of the Foot (JSSF) scale score (0-100 points; Figure 5),16,17 passive dorsiflexion angle of the first metatarsophalangeal joint, complications, plantar shift of the first metatarsal head, and shortening of the first metatarsal. The VAS scores were obtained by asking the patients their pain severity during daily activities and the patients marking the answer on a 100-mm line that best described it. The passive dorsiflexion angle was measured using an external hand-held goniometer with the ankle in the neutral position. The grade classification for the radiography and computed tomography of hallux rigidus in this study was defined for clarity as follows, referring to and taking care to approximately match the grade classifications reported so far3,5: grade 1, normal or mild joint space narrowing; grade 2, joint space narrowing without loss of joint space; grade 3, joint space narrowing with <50% loss of joint space in anteroposterior or lateral view; and grade 4, joint space narrowing with ≥50% loss of joint space in anteroposterior or lateral view. Radiograph images were initially used for grading, and when a radiograph image was difficult to grade, the computed tomography image was used.

Japanese Society for the Surgery of the Foot scale (Hallux metatarsophalangeal-interphalangeal scale).
The plantar shift of the first metatarsal head and the shortening of the first metatarsal were measured to supplementally investigate the associations with other measurements. Shortening of the first metatarsal was measured and calculated using the distance from the tip of the metatarsal head to the line that passed through the tip of the second metatarsal head and was vertical to the second metatarsal shaft in the pre- and postoperative anteroposterior radiographs (Figure 6A). Plantar shift of the first metatarsal head was measured using the distance between the dorsal cortex lines of the osteotomized first metatarsal fragments in the lateral radiograph (Figure 6B).

Radiographs showing measures of the plantar shift of the metatarsal head and the shortening of the metatarsal. (A) Shortening of the metatarsal. The distance (d) from the tip of the metatarsal head to the line that passed through the tip of the second metatarsal head and was vertical to the second metatarsal was measured using pre- and postoperative anteroposterior radiographs. Postoperative (d) – preoperative (d) was the shortening of the metatarsal. (B) Plantar shift of the metatarsal head. The plantar shift of the first metatarsal head (p) was measured using the distance between the dorsal cortex lines of the osteotomized first metatarsal fragments in the lateral radiograph.
Preoperative data were the data 1 month before surgery, and postoperative data were the data at the final follow-up. All data were obtained by the author.
Statistical Sample Size Calculation
The calculations of the post hoc power analysis were as follows, using α = 5% and power = 80% for all calculations: the required sample size calculated using difference of the mean = 50 and SD = 18 in terms of the VAS score was 4; the required sample size calculated using difference of the mean = 23 and SD = 13 in terms of the JSSF score was 5; the required sample size calculated using difference of the mean = 14 and SD = 17 in terms of dorsiflexion was 14; and the required sample size calculated using difference of the mean = 10 and SD = 12 was 24 for each length of the plantar shift of the metatarsal and the shortening of the metatarsal. Therefore, these analyses were sufficiently powered to detect improvements in outcomes other than dorsiflexion grade 1. 14
Statistical Analyses
Pre- and postoperative measures for the whole and individual grades were compared using the Wilcoxon signed-rank test, and the differences in the postoperative VAS scores with the different lengths of plantar shift of the metatarsal head and the shortening of the metatarsal were analyzed using the Kruskal-Wallis test. All tests were 2-tailed, and differences were considered statistically significant when the P value was less than .05. Additionally, post hoc power analyses were performed considering the means and SDs of the outcomes. All statistical analyses were performed using EZR (easy R), version 1.54 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a modified version of R version 4.0.3 commander (The R Foundation for Statistical Computing, Vienna, Austria) designed to add statistical functions for biostatistics.9,13
Results
Demographics
A total of 76 patients (female, 42 [55%]; male, 34 [44%]) with 80 feet were enrolled in this study. The mean age was 60.3 ± 10.2 (range, 20-78) years, and the mean body mass index was 23.1 ± 3.4 (range, 16.8-32.8). Among them, 46 patients (female, 20; male, 23) participated in recreational sports activities. The mean follow-up duration was 3.5 ± 0.7 (range, 2.0-4.9) years. The baseline characteristics are shown in Table 1. Six patients (7.5%) were grade 1, 20 (25.0%) were grade 2, 30 (37.5%) were grade 3, and 24 (30.0%) were grade 4.
Baseline Characteristics of the 76 Patients With Hallux Rigidus Who Underwent Sliding Oblique Metatarsal Osteotomy, Fixated With K-Wires, Without Cheilectomy.

Outcomes
Overall, the VAS score improved from 63.2 to 6.2 mm, the JSSF score improved from 59.0 to 82.6 points, and the angle of dorsiflexion improved from 37.3 to 56.3 degrees. Moreover, these scales improved in every grade (Table 2, Figure 7). The pre- and postoperative VAS scores were similar for all the grades; however, the pre- and postoperative JSSF scores and angles of dorsiflexion decreased as the grade increased (Figure 7).
Pre- and Postoperative Measures for the 76 Patients With Hallux Rigidus Who Underwent Sliding Oblique Metatarsal Osteotomy, Fixated With K-Wires, Without Cheilectomy.

Abbreviations: JSSF, Japanese Society for Surgery of the Foot; VAS, visual analog scale.
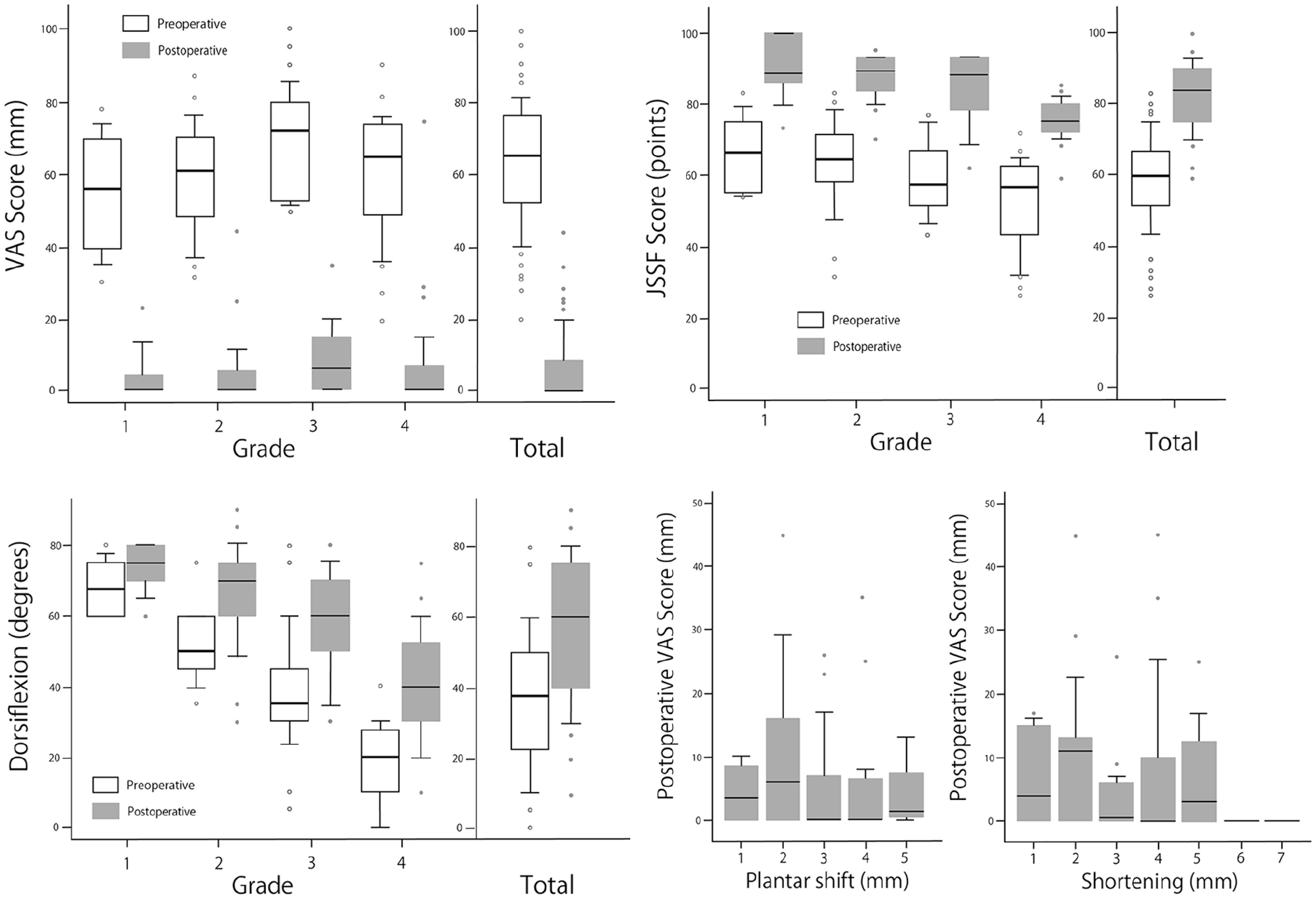
Box plots showing pre- and postoperative measures and differences in the postoperative VAS scores among the different lengths of the plantar shift of the metatarsal head and the shortening of the metatarsal.
The median length of the plantar shift of the metatarsal was 3 mm (range, 1-5), and the median length of shortening of the metatarsal was 4 mm (range, 1-7). The differences in the postoperative VAS scores among the lengths of the plantar shift of the metatarsal head or the shortening of the metatarsal are shown in Table 3 and Figure 7. In both the plantar shift of the metatarsal head and shortening of the metatarsal, there were no statistical differences in the postoperative VAS scores among the lengths with the numbers available (Kruskal-Wallis test, P = .26 and P = .67, respectively).
Differences in the Visual Analog Scale (VAS) Scores Among the Different Lengths of the Plantar Shift of the Metatarsal Head or Those of Shortening of the Metatarsal.

Complications
A total of 8 patients (10.5%) had complications; 4 (5.2%) had occasional plantar discomfort under the metatarsal head, 2 (2.6%) required shoe modification to fit the tip of the hallux (both patients had 5-mm shortening of the metatarsal), 1 (1.3%) had wound pain, and 1 (1.3%) experienced breakage of a K-wire.
The data on the 4 patients with occasional plantar discomfort under the metatarsal head are shown in Table 4. There was no clear tendency regarding the lengths of shortening of the metatarsal and the plantar shift of the metatarsal head.
Data on the Patients Who Had Occasional Postoperative Discomfort Under the Plantar Metatarsal Head.

Abbreviations: BMI, body mass index; VAS, visual analog scale.
Discussion
The study found that the VAS scores, angles of dorsiflexion, and JSSF scores improved for all grades of hallux rigidus, although dorsiflexion angles and JSSF scores decreased as the grade advanced (Table 2, Figure 7). This suggested that decompressive osteotomy of the metatarsal could be applicable for all grades of hallux rigidus.
The postoperative VAS scores decreased in all grades. Moreover, compared among the grades, the pre- and postoperative VAS scores were both similar (Table 2, Figure 7), which suggested that pain in hallux rigidus may not be dependent on the degree of the degenerative change of the joint. In hallux rigidus, damage to the cartilage on the dorsal third of the articular surface is seen, suggesting a heavy load when pushing off during gait. When this osteotomy is performed, the metatarsal head is shifted proximally, which loosens the muscles of the hallux, and the metatarsal head is lowered, which decompresses on the dorsal third of the metatarsal surface when pushing off during gait, thus decreasing pain. In addition, sliding the metatarsal head plantarward also lowers the large dorsal osteophytes so that the height of the osteophytes is approximately the same as the dorsal aspect of the metatarsals, reducing rubbing pain. The VAS improvement in all grades in this study suggests that the above mechanism functions in all grades.
Postoperative dorsiflexion improved in all grades (Table 2, Figure 7). The underlying mechanism may be that the hallux rode easily on the metatarsal head without impingement because of the lowering of the metatarsophalangeal head and loosening of the plantar soft tissues. However, both pre- and postoperative dorsiflexion angles decreased as the grade advanced (Figure 7). This suggests that articular degeneration is an important factor for range of motion.
There were no statistical differences in the VAS scores among the different lengths of the plantar shift of the metatarsal head and the shortening of the metatarsal with the numbers available (Table 3, Figure 7). However, the 2 patients with 5-mm shortening of the metatarsal required shoe modification. Moreover, a study where the plantar shift of the metatarsal was a median of 7 mm reported that 28% of patients had postoperative plantar discomfort. In contrast, occasional postoperative discomfort under the metatarsal head appeared to be unassociated with the lengths of the plantar shift of the metatarsal head and shortening of the metatarsal if the lengths were within 4 mm (Table 4). However, if a correction of 1 to 2 mm is the aim, there is a possibility that the correction will be insufficient. Considering these, a correction of 3 to 4 mm might be applicable for both shortening of the metatarsal and plantar shift of the metatarsal head.
The outcomes using the 3 K-wire technique and those using the one K-wire technique in another study 15 were similar; pre- and postoperative VAS scores were 63 to 6 and 70 to 6, pre- and postoperative JSSF sores were 59 to 82 and 61 to 86, and pre- and postoperative dorsiflexion was 37 to 56 and 53 to 66, respectively. 15 However, the occurrence rates of occasional postoperative plantar discomfort with 3 K-wires (5%) were lower than those with 1 K-wire (28%). The differences between the occurrence rates were considered to result from the differences in the surgical technique; 3 transverse K-wires could control the amount of plantar shift of the metatarsal head, whereas it was difficult to control with 1 longitudinal K-wire (Figure 1C). As a result, the lengths of the plantar shift with 3 K-wires (median 3 mm; range, 1-5 mm) were smaller than that with 1 K-wire (median, 7 mm; range, 3-10 mm).
We believe that decompressive osteotomy without cheilectomy could be considered as the first choice for all grades because this study demonstrated that this procedure was effective for all grades. In general, grades 1 and 2 are treated with cheilectomy, and grades 3 and 4 are treated with arthrodesis or arthroplasty. A cheilectomy requires resection of the dorsal one-third of the metatarsal head, which cannot be considered a minimally invasive surgery. Arthrodesis and arthroplasty are surgeries that destroy the articular surface. However, this technique does not damage the joint surface, and the surgical method is simple. Additionally, we believe that arthrodesis and arthroplasty should be used as salvage surgery after failure of this surgery, and cheilectomy without resection of the dorsal one-third of the metatarsal head should be used for treating the patients complaining of only dorsal rubbing of the spur in the shoe.
Limitations
This study had several limitations. First, the number of participants was small; therefore, (1) the analysis of dorsiflexion in grade 1 and the analyses of the differences in the VAS scores among different lengths of the plantar shift of the metatarsal head and the shortening of the metatarsal did not have adequate power; (2) the baseline characteristics could not be adjusted between the grades; (3) subclass analyses, such as comparisons between women and men or between a complication group and a noncomplication group, between patients who participated in sports activities and patients who did not could not be performed. Second, analyses combining discomfort with plantar shift of the metatarsal head, shortening of the metatarsal, and thickness of the plantar fat pad could not be performed. Additionally, changes in plantar pressure were quantically measured. Third, the follow-up duration was relatively short. Because the anatomic position of the metatarsal head was plantar-shifted in this procedure, the subsequent biomechanical change may cause transfer metatarsalgia and osteoarthritis in the metatarsal-sesamoid joint in the future. Fourth, all data were measured by the author alone. Therefore, the good results of this study may have resulted from observer bias. Fifth, all data were from a local hospital. The Japanese lifestyle of living barefoot indoors and often sitting on the floor may have influenced the good dorsiflexion angles in this study, and these results may not be applicable to other populations. Finally, the grading system used was not validated.
Conclusion
The VAS scores, the angles of dorsiflexion, and JSSF scores improved for all grades of hallux rigidus within a relatively short period of follow-up; however, dorsiflexion angles and JSSF scores decreased as the grade advanced.
Footnotes
Acknowledgements
The author would like to thank the Elsevier Language Editing Service for the English language review.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board of Yashio Central General Hospital (Approval number: YIHCE2021-11).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.