
Abstract
Background:
Hallux rigidus (HR) is a common source of forefoot pain and disability. For those who fail nonoperative treatment, minimally invasive dorsal cheilectomy (MIDC) is an increasingly popular alternative to the open approach with early positive results. Early failures may be due to lose bone debris from the MIDC as well as other intra-articular pathology that cannot be addressed with MIDC alone. Metatarsophalangeal (MTP) arthroscopy can be used in addition to MIDC to assess the joint after MIDC and address any intra-articular pathology while still maintaining the benefits of minimally invasive surgery. We report our clinical outcomes following MIDC combined with MTP arthroscopy.
Methods:
From November 2017 to July 2020, a retrospective analysis of all MIDC cheilectomies with MTP arthroscopy performed by the 2 senior authors was done. Wound complications, infections, revision rates, need for future surgery, conversion to fusion rates, pre- and postoperative range of motion, visual analog scale (VAS) scores, time to return to normal shoe, intraoperative arthroscopic findings, and operative time were collected. Follow-up average was 16.5 months (range 3-33 months).
Results:
A total of 20 patients were included with an average follow-up of 16.5 months. The average VAS score improved from 7.05 preoperatively to 0.75 postoperatively (P < .05). Average range of motion in dorsiflexion increased from 32 to 48 degrees (P < .05) and plantarflexion increased from 15 to 19 degrees plantarflexion (P < .05). All patients were weightbearing as tolerated immediately after surgery in a postoperative shoe and transitioned to a regular shoe at average of 2.1 weeks. We had no wound infections, wound complications, revision surgeries, tendon injuries or nerve damage. One patient required conversion to a fusion 3 years after the index procedure. Average tourniquet time was 30.39 minutes (range 17-60 minutes) and total average operating room time was 59.7 minutes (range 40-87 minutes). On arthroscopic evaluation of the MTP joint after MIDC, 100% of patients had bone debris, 100% had synovitis, 10% had loose bodies, and 30% had large cartilage flaps within the joint.
Conclusion:
MIDC and first MTP joint arthroscopy for treatment of hallux rigidus provide improved pain relief with minimal complications while still maintaining the benefits touted for minimally invasive operative procedures. Additionally, we have shown a high rate of intra-articular debris along with intra-articular pathology such as synovitis, loose chondral flaps, and loose bodies that exist after MIDC. This combined procedure has the potential for improving patient outcomes and may minimize risk of future revision surgeries compared with MIDC alone.
Level of Evidence:
Level IV, case series study.
Keywords
Introduction
Hallux rigidus is a common source of forefoot pain and disability, with 2.5% of individuals aged ≥60 years having this diagnosis. 14 Initial nonoperative management can lead to satisfactory outcomes in up to 55% of patients, however, for those who fail these measures, operative treatment is indicated, with overall very positive results. 7,15
End-stage first metatarsophalangeal (MTP) osteoarthritis with mid-range symptoms are best served with arthrodesis. 2,3 -6,9,11,13,15,16,20,21,27,31 Patients with mild to intermediate-grade changes who lack midrange pain have traditionally had excellent outcomes including improved pain and range of motion with open dorsal cheilectomy. 10,12,17,24,26,27
Minimally invasive dorsal cheilectomy (MIDC) has become an increasingly popular alternative to the open approach. Commonly using a dorsomedial stab incision and percutaneous instrumentation, the dorsal osteophyte resection can be performed under fluoroscopic guidance. 30 Several recent studies have reported faster rehabilitation, lower overall morbidity, with clinically significant improvement in pain and range of motion. 18,30 However, despite these initially positive results, there are also reports of increased rates of complications and reoperation when compared to the open technique because of learning curve–associated technical errors, incomplete resection, retained bone fragments within the MTP joint, and other associated MTP joint pathology that goes unaddressed with the use of MIDC alone. 28,30
In order to overcome some of the limitations of isolated MIDC, while still maintaining the benefits of this minimally invasive surgery, the senior authors combine this procedure with first MTP arthroscopy. This allows for direct visualization of the joint, which aids in removal of any retained bone fragments from the MIDC but also helps to identify and treat other intra-articular pathology, including synovitis, chondral injuries, and loose bodies.
There have been no prior studies reporting outcomes from this novel combined approach. Therefore, the purpose of this study is to assess infection rates, wound complication rates, revision rates, visual analog scale (VAS) scores, pre- and postoperative range of motion, and intra-articular finding of MIDC in combination with first metatarsophalangeal arthroscopy. We hypothesize that MIDC with first MTP arthroscopy will result in significant improvement in patient pain and function while at the same time addressing MTP joint pathology, leading to improved patient outcomes and lower rates of revision surgery.
Methods
This study was approved by our institutional review board. We performed a retrospective review of all patients with the diagnosis of hallux rigidus who underwent a minimally invasive cheilectomy in combination with first MTP joint arthroscopy and debridement between November 2017 and July 2020. Patients were identified using Current Procedural Terminology (CPT) code 28289. All patients had failed nonoperative treatment prior to operative intervention. MIDC with MTP arthroscopy was indicated for patients with physical examination findings consistent with pain at the extreme ranges of dorsiflexion and plantarflexion, negative grind test, and radiographic imaging with dorsal first MTP osteophytes. The surgeries were performed by one of 2 fellowship-trained orthopedic foot and ankle surgeons (J.K. and T.G.). Patients were followed for a mean follow-up of 16.5 months (range 3 and 33 months).
Operative Technique
The patient is positioned supine with their heel at the end of the bed. A thigh tourniquet is placed and set to 275 mm Hg. When possible, dorsomedial cutaneous nerve to the hallux was marked with an operative marker. The operative incision was marked approximately 1.5 to 2.5 cm proximal to the hallux metatarsophalangeal joint. A 2-mm incision is made through the skin with a beaver blade and a blunt curve snap is used to spread down to the bone (Figure 1). A periosteal elevator is then used to elevate the periosteal tissue and the joint capsule off of the dorsal spur on the hallux metatarsal head. A high-speed, low-torque burr is used to complete the cheilectomy. A 3.1×13-mm wedge burr from either Wright Medical (Memphis, TN) or Novastep (Orangeburg, NY) was used to complete the cheilectomy under fluoroscopic guidance with a mini-C-arm) (Figure 2). While performing the debridement, the hallux is held in a neutral to slight dorsiflexed position to take the tension of the extensor hallucis longest tendon and protect it. The wound is irrigated copiously using a syringe with an Angiocath tubing attached with normal saline as well as specialized rasp used to remove any large fragments from the soft tissue. This is done prior to the arthroscopic portion of the case to remove any major debris from the dorsal aspect of the metatarsal head or hallux metatarsophalangeal joint and aide in initial visualization with the arthroscope.

Clinical image demonstrating incisions for MIDC with first MTP arthroscopy. (A) MIDC incision. (B) Dorsomedial arthroscopy portal incision. (C) Dorsolateral arthroscopy portal incision. MIDC, minimally invasive dorsal cheilectomy; MTP, metatarsophalangeal.

(A). Preoperative lateral radiograph demonstrating dorsal spurring. (B) Postoperative lateral radiograph demonstrating resection of dorsal spurring.
Once sufficient debridement is completed, the minimally invasive burr is removed and the first MTP arthroscopy is performed. The bed attachment is placed at the end of the bed and the noninvasive ankle distractor is placed and angled away from the edge of the bed in line with the hallux. To achieve traction, a 2-inch Kling gauze is wrapped around the hallux proximal phalanx and tensioned around the distraction bar. Once traction is achieved, this Kling gauge is tied upon itself and reinforced with a Kocher clamp (Figure 3). The extensor hallucis longus tendon is marked, and standard dorsomedial and lateral portals are made. A blunt trochar is used to enter into the joint and a 1.9- or 2.7-mm 30-degree angled arthroscope (Arthrex, Naples, FL) is used for the arthroscopy. The dorsolateral portal is triangulated under direct visualization with an 18-gauge needle. Diagnostic arthroscopy is performed to evaluate the extent of cartilage loss on the metatarsal head and proximal phalanx, evaluate for intra-articular pathology such as focal osteochondral defects, cartilage flaps, or loose bodies and evaluate for the presence of any retained bone debris from the cheilectomy (Figure 4). Debridement of the joint is completed with a small joint 3.0 dissector shaver (Arthrex). Care is taken to not only debride any intra-articular synovitis, cartilage flaps, loose bodies but also retain bone debris from the cheilectomy. Additional shaving of the hallux metatarsal head can be done under direct visualization of the arthroscope using either the arthroscopic shaver through the portals or with the minimally invasive burr through the initial incision to smooth out the prior resection.

MIDC done under fluoroscopy. (A) Identification of bone spur. (B) Placement of burr next to bone spur. (C) Cutting of spur. (D) Final resection of bone spur. MIDC, minimally invasive dorsal cheilectomy.
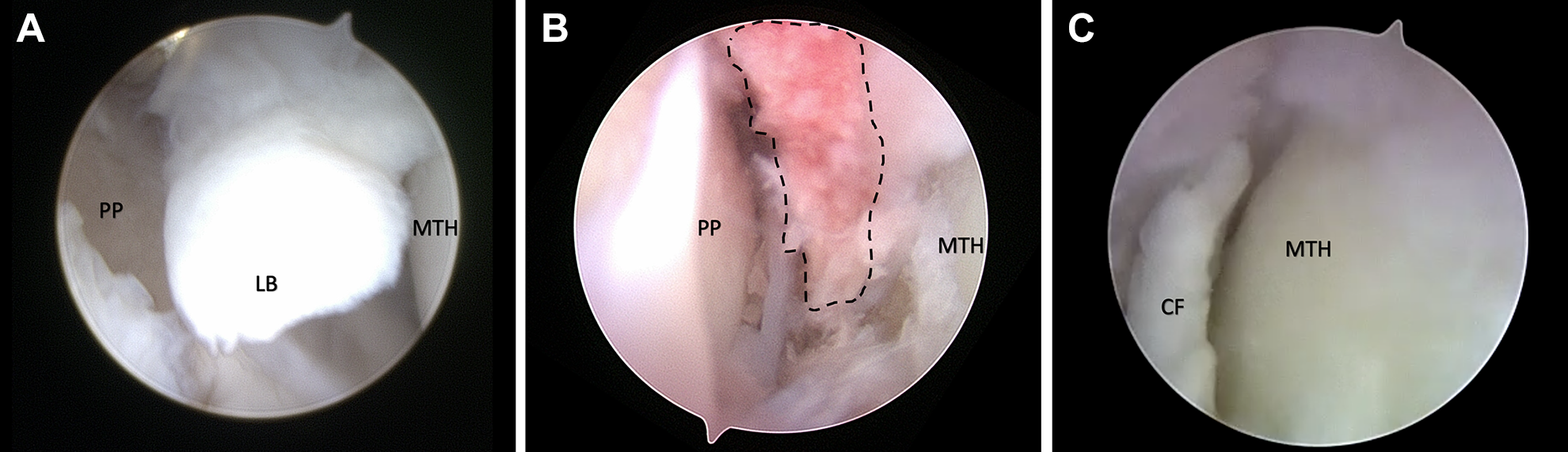
(A) Intraoperative image of first MTP arthroscopy demonstrating loose body. (B). Intraoperative image of first MTP arthroscopy demonstrating residual intra-articular debris (dashed line) after minimally invasive dorsal cheilectomy. (C). Intraoperative image of first MTP arthroscopy demonstrating chondral flap. CF, chondral flap; LB, loose body; MTH, metatarsal head, PP, proximal phalanx.
On completion of the arthroscopic portion of the case, the traction is released. The wounds are closed with 4-0 nylon suture. Sterile gauze with toe strapping are placed which remain on for 1-2 weeks. Postoperatively the patient is weightbearing as tolerated in a stiff-soled postoperative shoe for 1-2 weeks and then transitioned to regular shoes as tolerated. The patient is instructed on range of motion exercises for the hallux MTP joint to begin immediately postoperatively and is allowed to progress all activities as tolerated once transitioned to a regular shoe.
Outcomes
Preoperatively visual analog scale (VAS) pain levels and range of motion were recorded. Intra-operatively data recorded included evaluating for the presence of intra-articular pathology including synovitis, cartilage damage, loose bodies, and remaining bone debris from the cheilectomy. Tourniquet time and total operative time were collected. Postoperatively VAS pain levels, range of motion, need for secondary surgery, and time to regular shoes was recorded. Additionally, assessment for any complications was recorded, including wound dehiscence or infection, nerve complications, and extensor hallucis longus tendon injury. Statistical analysis was performed on VAS outcomes scores using a paired t test. Statistical significance was set at P <.05.
Results
A total of 20 patients were included in the study with an average age of 52 (range 40-69) years. Average VAS score preoperatively was 7.05, and postoperatively 0.75 (P < .05). Average dorsiflexion increased from 32 to 48 degrees (P < .05) and plantarflexion increased from 15 to 19 degrees plantarflexion (P < .05) (Table 1). There was no evidence of nerve injuries, damage to the extensor hallucis longus, wound infections, or wound complications. There were no revision cheilectomies; however, 1 patient required conversion to fusion at 3 years post index procedure. Average time to wearing a normal shoe was 2.1 weeks.
Patient demographics and Preoperative Range of Motion and Pain Scores.

Average tourniquet time was 30.4 (range 17-60) minutes, and the total average operating room time was 59.7 (range 40-87) minutes. On arthroscopic evaluation of the first MTP joint after MIDC, we found that 100% of patients had bone debris within the hallux metatarsophalangeal joint from the cheilectomy despite copious irrigation after the cheilectomy but before the arthroscopy. Additionally, 100% of patients had evidence of synovitis, 10% had a loose body within the MTP joint, and 30% had a loose cartilage flap.
Discussion
Our study looked at MIDC with first MTP joint arthroscopy and showed improvement in VAS score with a very low complication rate and revision rate. We also found high rates of intra-articular debris and synovitis after cheilectomy with our arthroscopic evaluation.
Minimally invasive forefoot surgery has grown over the last 2 decades and has shown many advantages over an open technique, with good patient outcomes including fewer complications, shorter operative time, smaller incisions, less soft tissue disruption, better cosmesis, lower risk of infection, and shorter postoperative recovery time compared with open procedures. 1,8,19,22,23,25,28 -30,32
Morgan et al 23 performed a prospective study comparing open cheilectomy and MIDC and found improvement in foot pain, function, and social aspect in the MIDC group comparable to the open group. They had 3 failures in the open group that were converted to fusions and none in the MIDC group. Razik et al 25 reviewed 47 patients at a minimum of 1 year postoperatively, 22 with MIDC and 25 with open cheilectomy. All patients had improvement in VAS pain scores; however, there were fewer reported incidences of infection and postoperative complications with minimally invasive surgery (MIS) compared with the open approach. We utilize the MIS technique for most primary cheilectomies. We consider open technique when it is a revision case or if there is a chance that the cheilectomy may require an additional procedure such as joint replacement or possible fusion due to significant cartilage loss. However, ultimately, the decision between open and MIS cheilectomy is up to the surgeon and their comfort and experience with this MIS technique.
In a separate study, Teoh et al 30 reported on their clinical outcomes in 98 operated feet undergoing MIDC. They reported an average VAS score improvement from 8 preoperatively to 3 postoperatively, as well as an in improvement in all MOxFQ domains. 30 Dawe et al 8 reported on infections and found that 1 in 16 patients in the MIDC group had a superficial infection that resolved with oral antibiotics whereas Stevens et al 28 reported no infections out of 133 patients who underwent MIS cheilectomy.
Despite these positive early reports, several issues have been brought up in the literature concerns with MIDC such as incomplete resection, need for revision surgery, and complications secondary to debride and loose bodies in the joint. 28,30 Teoh et al 30 reported they had a reoperation rate of 12% in their patients, 7 of whom underwent arthrodesis, 4 had repeat cheilectomy for residual impingement, and 1 had open removal of loose body. Stevens et al 28 had a similar reoperation rate in the MIS group of 12.8% owing to issues they related directly to MIS, including residual bone particles leading to impingement, stiffness and wound complications, dorsal medial cutaneous nerve injury, and extensor hallucis longus rupture.
This evidence supports that with MIDC alone, there is a possibility of loose bodies and debris within the joint despite irrigation after cheilectomy that can lead to continued pain, impingement, stiffness, and need for revision surgery. Teoh et al 30 attributed this to the learning curve that comes with the MIDC technique and the lack of visualization of the joint other than with fluoroscopy, whereas Stevens et al 28 found no association with a learning curve. Although the surgeon’s learning curve may be a contributing factor, we believe these problems relate to the inability to visualize the MTP joint as intra-articular pathology and retained bone debris are common in these procedures which probably is a contributing factor to many of these complications.
In our study, we found that 100% of our patients had bone debris within the joint after cheilectomy seen on first MTP arthroscopy despite copious irrigation after the cheilectomy was performed. Additionally, 100% of patients had intra-articular synovitis, 10% had loose bodies, and 30% had large cartilage flaps within the joint. Addition of first MTP arthroscopy after MIDC allows surgeons to perform a joint debridement, remove loose bodies and synovitis, and resect any cartilage flaps that may cause impingement. Therefore, we believe that complete visualization of the joint with first MTP arthroscopy after MIDC is an important factor in these cases to optimize outcomes. We believe the success of our patients with improved pain relief and minimal revision rates and postoperative stiffness is due to utilizing this technique and may not be associated with the learning curve alone.
Our outcome results are similar to those reported in the literature. Our average VAS preoperatively was 7.05 and postoperatively was 0.75 (P < .05). All patients were very satisfied and would have the procedure again. Range of motion improved on average from a preoperative 15 degrees plantarflexion and 32 degrees dorsiflexion to postoperative 19 degrees plantarflexion and 48 degrees dorsiflexion. In terms of activity, all patients were weightbearing as tolerated immediately after surgery in a postoperative shoe and had transitioned to a regular shoe average of 2.1 weeks and had been allowed to progress to all activities as tolerated. We had no wound infections, wound complications, tendon injuries, or nerve damage at an average final follow-up of 16.5 months. Our data suggest that the addition of the first MTP arthroscopy still allows for the benefits and early functional recover of MIDC alone but with the ability to visualize the MTP joint and address associated pathology.
Our study is not without limitations. One limitation is the relatively small number of patients, in which our cohort only includes 20 patients. Additionally, our cohort does not include a control group. However, given that there are no studies reporting on MIDC with addition of first MTP joint arthroscopy, we felt that reporting on our first 20 patients provides a potential foundation for future studies. This information we believe is valuable to anyone doing minimally invasive cheilectomies and has also prompted the senior authors to now start to organize a prospective randomized controlled trial to assess the true outcomes of MIDC with first MTP joint arthroscopy.
Conclusions
MIDC and first MTP joint arthroscopy for treatment of hallux rigidus may provide improved pain relief with minimal complications while still maintaining the benefits touted for MIS procedures. Additionally, we noted a high rate of intra-articular debris and other pathologies, such as synovitis, loose chondral flaps, and loose bodies. These pathologies can be addressed by adding first MTP joint arthroscopy after MIDC to improve patient outcome and minimize risk of revision surgeries.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_2473011421993103 - Minimally Invasive Dorsal Cheilectomy and Hallux Metatarsal Phalangeal Joint Arthroscopy for the Treatment of Hallux Rigidus
Supplemental Material, sj-pdf-1-fao-10.1177_2473011421993103 for Minimally Invasive Dorsal Cheilectomy and Hallux Metatarsal Phalangeal Joint Arthroscopy for the Treatment of Hallux Rigidus by Rachel L. Glenn, Tyler A. Gonzalez, Alexander B. Peterson and Jonathan Kaplan in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was obtained for this study from University of South Carolina IRB Committee (IRB number Pro00100902).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.