
Abstract
Background:
In 2019 the majority of US medical students were women (50.5%). However, despite this representation, female representation within orthopaedic surgery remains low when compared to male counterparts. Previously, the American Society for Surgery of the Hand (ASSH) and Pediatric Orthopaedic Society of North America (POSNA) published their gender diversity data. No such study has been conducted in the American Orthopaedic Foot & Ankle Society (AOFAS), which is the largest membership organization for foot and ankle–trained orthopaedic surgeons. This study sought to investigate whether increased female representation in the AOFAS membership roster is reflected in different levels within the organization.
Methods:
The 2012-2022 membership rosters were obtained from the AOFAS and compared by gender. Volunteer, elected, and appointed leadership positions as well as rates of engagement were compared for each of the activities. Leadership positions were defined as committee chair, vice chair, or board of directors (BOD). When available, time for advancement through leadership positions to the presidential role was analyzed by gender. Comparative data were available for 2 other respective subspecialty groups, ASSH and POSNA, from previously published studies.
Results:
Between 2012 and 2022, the percentage of female membership in the AOFAS has continued to increase from 7.5% (n=76) to 13% (n=163). Engagement in committee membership positions during this time has more than doubled from 11 of 26 (14.4%) to 57 of 163 (34.9%). When participation trends were evaluated by gender, women showed higher rates of committee involvement than their male counterparts. In 2021 compared to 2012, the percentage of female committee members more than doubled compared with their male counterparts (female 34.9% to male 23.2% vs female 14.4% to male 16.8%). This increase in female gender committee composition trend has been seen in the ASSH and POSNA, but it is more pronounced in the AOFAS. Representation of women in committee chair positions and elected positions has not seen this same parallel increase.
Conclusion:
The female membership of the AOFAS has a similar gender composition to other orthopaedic subspecialities. Female membership within the society has increased over the past 10 years. The rates of female involvement within committee membership positions have seen a parallel increase. It will take time to mature into leadership roles as we continue to increase diversity within our respective subspecialty organizations. Inception of the AOFAS Diversity Equity and Inclusion and Women’s Subcommittee demonstrate a continued emphasis on this core value within the society.
Level of Evidence:
Level IV, cohort study.
Keywords
Introduction
There are now more women enrolled in US medical schools than men. According to Association of American Medical Colleges (AAMC) 2019 data, the majority of US medical students enrolled were female (50.5%). 4 Despite the achievement of gender equity in medical schools, the number of women entering surgical subspecialties lags behind. Furthermore, orthopaedic surgery remains significantly less diverse than medical and other surgical subspecialties with respect to race/ethnicity and gender.2,3,5,6,11,16 In 2019, female physicians represented 36.3% of active practicing physicians in the United States. 1 Female representation was as high as 64.3% in the pediatric specialty and as low as 5.8% in orthopaedic surgery according to AAMC data. 1
At the fellowship level, this is supported by the lack of increase in diversity in gender as well as race/ethnicity over a recent 10-year evaluation of American College of Graduate Medical Education (ACGME)–accredited orthopaedic fellowship programs. 14 The top 3 subspecialty fellowship choices among female orthopaedic surgeons are pediatrics, musculoskeletal oncology and hand. 14 Foot and ankle surgery ranks as the fourth most popular specialty choice among women ahead of trauma, sports, spine, and adult reconstruction in order of gender diversity. 14 Although, these results may be biased as only 40% of orthopaedic fellowship programs are ACGME accredited as of 2021. 8 The American Society for Surgery of the Hand (ASSH) and Pediatric Orthopaedic Society of North America (POSNA) published their gender diversity data from 2014-2018.9,13 Despite rising popularity among female orthopaedic residents, no such study has been conducted in the largest orthopaedic foot and ankle society: the American Orthopaedic Foot & Ankle Society (AOFAS).
Our study sought to evaluate whether an increase in female representation within the AOFAS translated to representation within different levels of the organization. Second, the average time to presidency from membership initiation within the AOFAS was investigated.
Methods
The active membership roster was obtained from the AOFAS starting from 2012-2022 and compared by gender. Male vs female identity was a self-reported binary choice, and data reported in this study is representative of AOFAS member–reported gender identity. Both voluntary and elected leadership positions were collected over the 10-year span. Committee positions were also evaluated by gender. Leadership positions were defined as appointment to committee chair or vice chair, appointment to elected positions or board of directors (BOD) and presidency. The AOFAS invites eligible members to apply to serve on committees each year, with a small number of committees directly appointed by the board. Applications are reviewed by the Governance Committee. Selection of members is dependent on committee chair evaluation rankings, prior experience on AOFAS committees, the number of positions available as well as the number of appointments already offered to that individual to maximize the number of members who serve, per the Executive Director of AOFAS.
Time from membership initiation to elected leadership positions as well as AOFAS presidency was analyzed by gender. The AOFAS Board of Directors currently consists of 11 members, 5 of whom are voted on each year by AOFAS Active Members. The Nominating Committee selects nominees for these 5 positions each year. The Nominating Committee consists of 3 elected members, the Immediate Past President and a President-appointed member. The Board of Directors is composed of the President, President-Elect, Vice President, Secretary, Treasurer, the Immediate Past President, the Past President, and 4 Members-at-Large. One or more of the Members-at-Large is younger than 45 years of age as of the election date. Only Active Members of the Society, in good standing, are eligible to serve as elected officers.
Results
Membership Participation
The total membership of the AOFAS increased from 1018 to 1252 members during the time period of 2012-2022. The percentage of female membership during that time increased from 7.5% (n=76) to 13% (n=163), whereas the total percentage of male membership has decreased slightly from 92.5% (n=942) to 86.9% (n=1088) (Table 1).
Ten-Year (2012-2022) Membership Roster for AOFAS. a

Abbreviation: AOFAS, American Orthopaedic Foot & Ankle Society.
Note that 2014 and 2015 gender breakdown is an estimation based on previously available 2013-2016 data. Overall, 10-year trend points to increasing female membership within the society.
Committee Participation
On average, 110 applications are received each year from active members for continuation or to begin service on a committee. Membership has been broken down by gender for each of the respective subcommittees. The female committee involvement has more than doubled since 2012 (Table 2). Females holding committee membership positions increased from 6.5% (n=11) to 18.5% (n=57) compared to male committee membership positions declining from 93.5% (n=6.5) to 81.5% (n=252) (Figure 1).
Involvement Rate in Committees Open to Membership Broken Down by Gender.
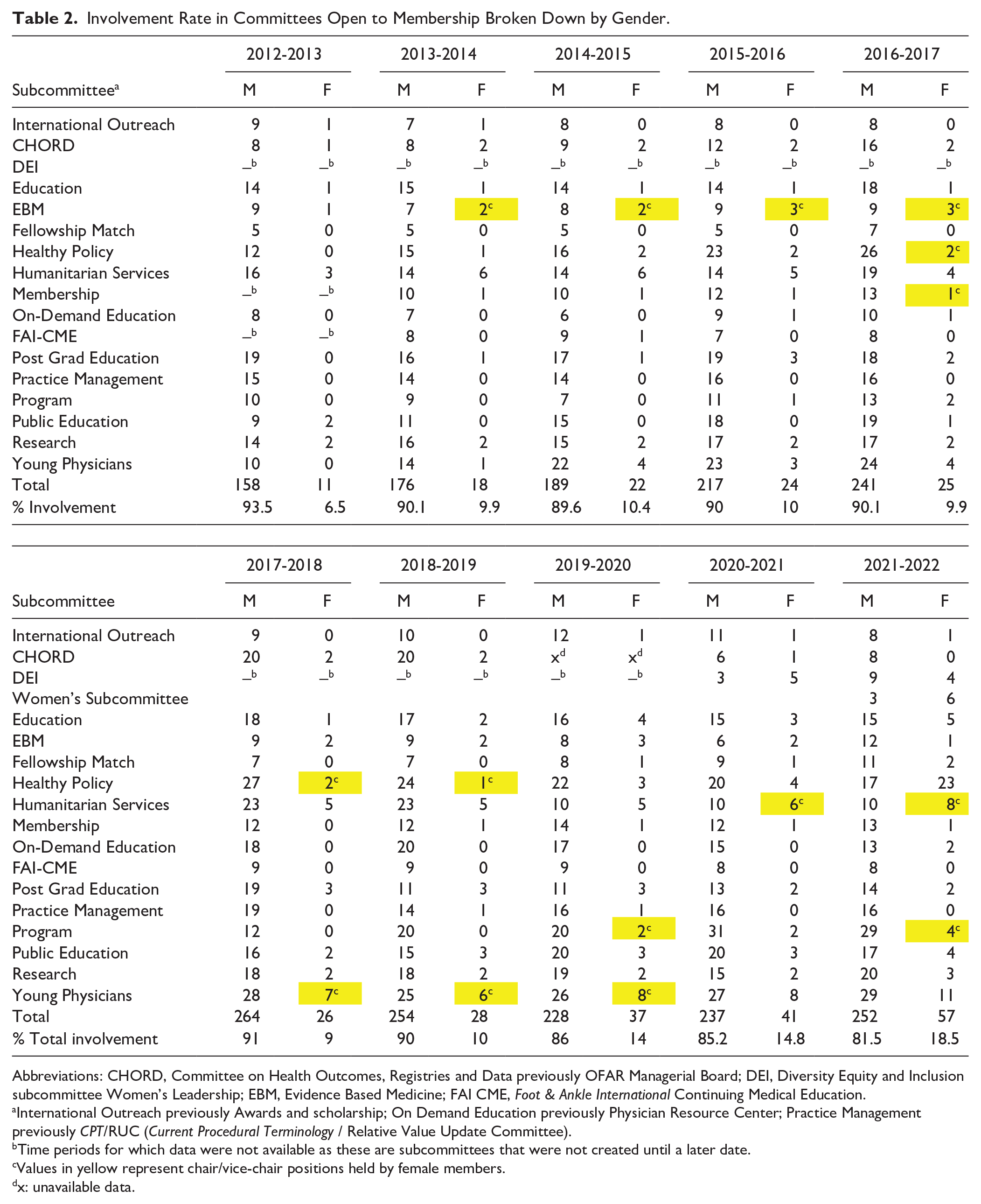
Abbreviations: CHORD, Committee on Health Outcomes, Registries and Data previously OFAR Managerial Board; DEI, Diversity Equity and Inclusion subcommittee Women’s Leadership; EBM, Evidence Based Medicine; FAI CME, Foot & Ankle International Continuing Medical Education.
International Outreach previously Awards and scholarship; On Demand Education previously Physician Resource Center; Practice Management previously CPT/RUC (Current Procedural Terminology / Relative Value Update Committee).
Time periods for which data were not available as these are subcommittees that were not created until a later date.
Values in yellow represent chair/vice-chair positions held by female members.
x: unavailable data.
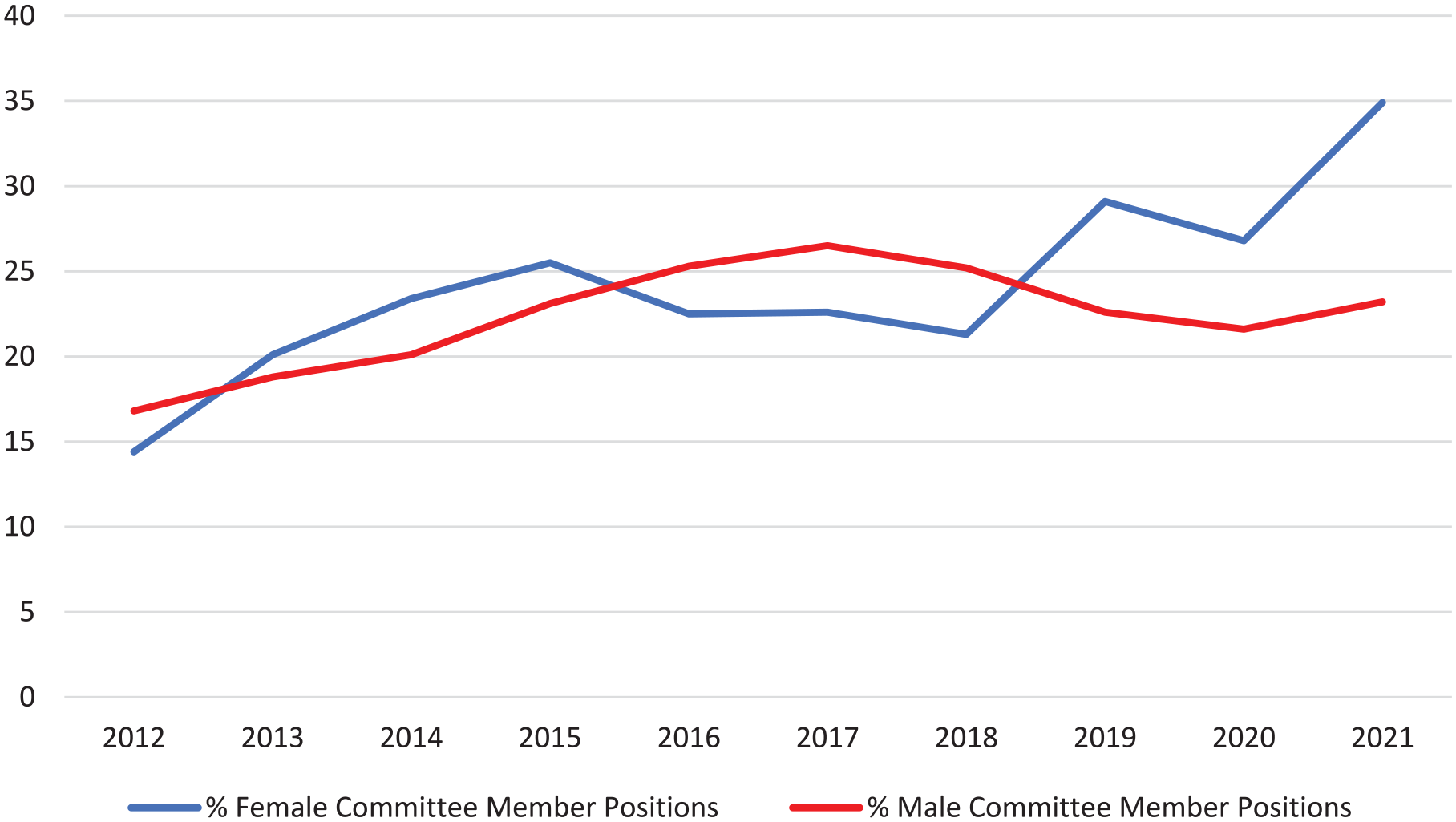
Percentage of female vs male representation within AOFAS volunteer committee positions from 2012-2021.
We further analyzed the data to evaluate the proportion of men and women in AOFAS involvement at the committee level. For each year examined, there was a higher proportion of female AOFAS members (total active number of female members/female volunteer committee members) involved in committees (Table 3). This increased from 14% (11 of 76) to 34.9% (57 of 163) among female AOFAS members vs 16.8% (158 of 942) to 23.2% (252 of 1086) among male members.
Involvement Rate Within Volunteer Committee Positions Relative to Overall Active Members, by Gender From 2012 to 2021.
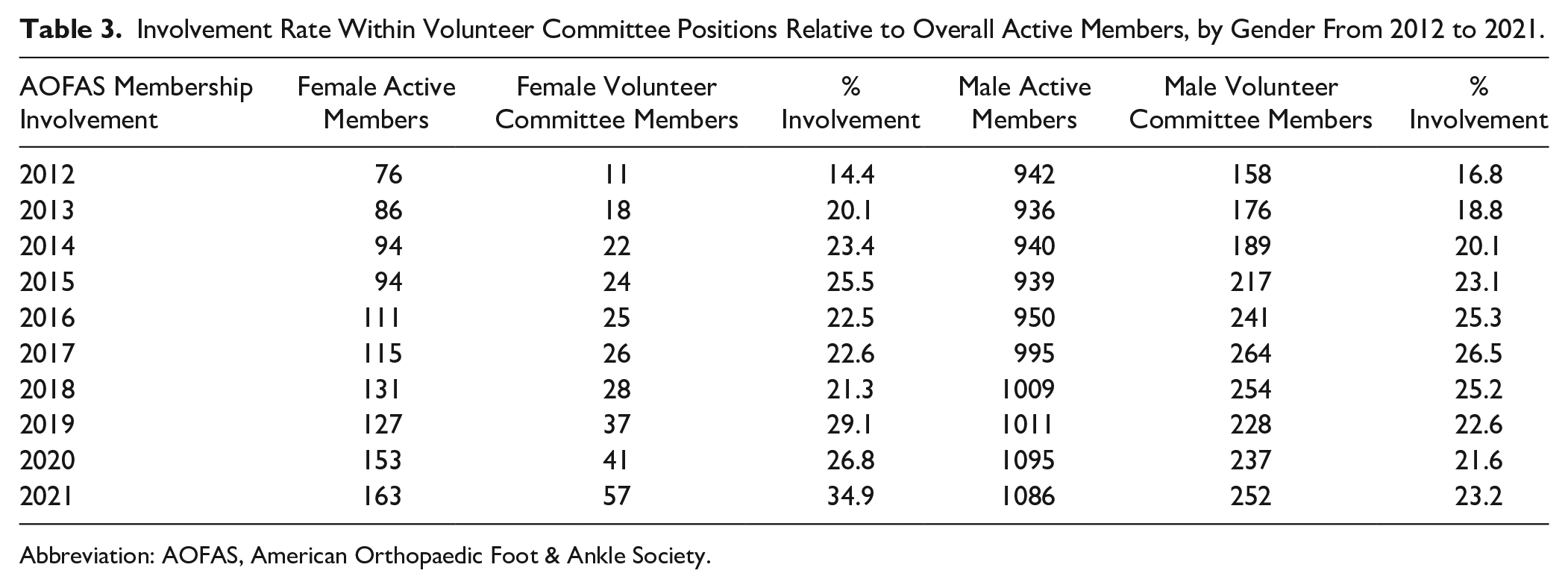
Abbreviation: AOFAS, American Orthopaedic Foot & Ankle Society.
Advancement to Leadership and Presidential Line
Since the inception of the organization in 1969, there has been only 1 female president. The time from membership initiation to AOFAS presidency for the female president was 17 years. Thirty-two previous AOFAS presidents were identified in the database available, with an average 17.7 years from membership to presidency. A 10-year review from 2012-2022 demonstrates that the average time from membership to presidency is trending upward to an average of 23.2 years. The percentage of female members holding elected positions including in the BOD and Committee chair positions are broken down by gender and presented in Table 4 and Figure 2.
Appointed or Elected Positions From 2012-2022.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; BOD, Board of Directors; COI, Committee on outside interests; FAI, Foot & Ankle International; FAO, Foot & Ankle Orthopaedics; OFAF, Orthopaedic Foot and Ankle Foundation.
Governance previously known as Committee-on Committees.
Time periods for which data were not available as these are subcommittees that were not created until a later date.

Percentage of leadership positions occupied by female AOFAS members from 2012 to 2021.
Discussion
In the past 10 years, the percentage of female membership in the AOFAS has increased steadily from 7.5% (n=76) to 13% (n=163). It is clear that this increase in membership has also translated into a comparable increase in the representation of women holding volunteer committee roles within the organization as this has more than doubled in 10 years (female: 14% [11/76] to 34.9% [57/163]) compared with the proportion of male involvement in committee-level positions (16.8% [942/158] to 23.2% [1086/252]). Representation of women in higher-level leadership positions within the organization is lower than the membership percentage. Despite this, the small number of women at the highest levels of the AOFAS society does not appear to correlate with a lack of participation among female members in their committee activity. The percentage of women in AOFAS applying for volunteer positions (2022; 34.9%) is greater than their society membership proportion (2022; 13%), suggesting that future women leaders are actively engaged in the organization.
The time from membership initiation to AOFAS presidency for the only female president was 17 years. Thirty-two previous AOFAS presidents were identified in the available database, with an average of 17.7 years from membership to presidency. This is similar to data published from POSNA, with the average time from membership to presidency of their sole female president being 21 years, and 19.5 years for the average male president (range 14-30 years). 13
The American Academy of Orthopaedic Surgeons has highlighted the lack of diversity in gender and racial/ethnic minorities within the field of Orthopaedics as an important topic that needs to be addressed. 18 Rohde and colleagues 15 recently evaluated factors that limit female involvement within the field of orthopaedics, noting perceived work-life balance, physical strength requirements, and lack of female mentors and role models as leading reasons in deterring women from pursuing this specialty. Orthopaedics has the lowest percentage of female faculty and resident enrollment compared with other specialties. 12 In contrast, by 2020, general surgery became the most diverse among the seven surgical subspecialties by implementing a holistic review of resident applications and applying mentoring programs to address disparities. 7
The concept of mentorship and its role in helping women achieve their professional potential in orthopaedics has previously been well described. 17 However, to be an effective sponsor to trainees, sponsors must have substantial organizational influence to advocate for junior colleagues. Membership alone does not bolster women into leadership roles.
There is value in equity. Venkat et al 17 examined the case of gender equity advocacy on a value-based health care model, citing that sponsorship of women to achieve leadership roles creates value by driving return on workforce investments, protecting against attrition, and fulfilling patient expectations of a diverse clinical and surgical care team. Ultimately, this leads to a safe and culturally competent environment that benefits the diverse patient populations in which we care for.
Previously both the ASSH and POSNA examined their respective subspecialty societies participation from the perspective of gender and leadership over a 5-year span.9,13 These organizations represent 2 of the top chosen specialties for female orthopaedic residents. 14 Our numbers suggest a similar trend in leadership ascension within the AOFAS. Female membership has continued to increase over the past 10 years. Women are participating in society advancement pathways at a higher percentage than their male counterparts. One plausible reason for the lower rates of female representation to Board of Director (BOD) positions in this 10-year review is the time lag that exists for advancement to the highest levels of the organization. We found that it took, on average, about 17 years to reach the highest level of the organization. However, the smaller number of women holding high-level leadership/elected positions does not appear to correlate with a lack of participation at the committee level. This is encouraging, but we do recognize the importance of female leadership and the paucity of this currently existing within the AOFAS. We are hopeful that with continued female involvement in committees and increased awareness around the importance of diversity and equity, leadership roles will begin to reflect this. It has been shown that female mentorship is linked to promotion and retainment of females in academic medicine. 10 As female leadership becomes more prevalent, it may be important to establish mentorship programs to help promote this cause.
There are several limitations to this study. Specifically, this provides a short time period (10 years) of evaluation relative to the length of the organization’s history. It is, however, the longest review available to date compared with previous published reviews within other respective subspecialty organizations. We believe this 10-year evaluation both captures the current trends and accounts for natural variation in gender involvement within the society. Although the data presented are not generalizable to other subspecialty organizations as they capture only that from a single subspecialty, it is clear based on the currently available data that our society is trending in the right direction. Future studies can extrapolate on initiatives within the organization to increase diversity with female roles and the DEI subcommittee to determine if they will translate into leadership roles within the society.
Conclusion
Female involvement at the committee level within the AOFAS is increasing at a faster pace than their male counterparts, which indicates that females are actively engaged in the organization. Although the overall percentages have increased, the raw numbers are small and ongoing vigilance is needed to ensure growth within the organization. Inception of the Diversity Equity and Inclusion and Women’s Subcommittee demonstrate a continued emphasis on this core value within the society. It is imperative that the AOFAS continues to bring awareness to this issue and encourages further participation and fosters leadership opportunities that are more diverse and inclusive.
Footnotes
Acknowledgements
The authors would like to thank Elaine Leighton, Shelly Encher, and Nathaniel Kier and the AOFAS for their assistance in conducting this study
Author Note
Two authors have been members of the board of directors/previous president of the AOFAS. This work was completed in its totality in Portland, Oregon at Oregon Health & Science University.
Ethical Approval
Ethical approval was not sought for this study as it did not pertain to patient-acquired data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.