
Abstract
Background:
The hindfoot fusion nail has become a popular implant for tibiotalocalcaneal (TTC) arthrodeses given its rigidity, ease of insertion, and potential for less invasive surgical approaches. The purpose of this study was to evaluate fusion and complication rates following the use of a straight, retrograde intramedullary nail for TTC arthrodeses, and the influence of diabetes and smoking on these results.
Methods:
A review of patient cases performed by a single surgeon at a single institution was performed. Variables included age, comorbidities, smoking history, BMI, hemoglobin A1c, preoperative and postoperative visual analog scale pain scores, assessment of healing, and complications. Relative and absolute risk were assessed for smoking, diabetes, fusion, and surgical complications through risk ratios. Cox proportional hazards survival analyses were performed to assess the effects of smoking and diabetes on fusion rates and complications. Linear regressions were performed to investigate the effects of smoking and diabetes on patient-reported pain levels.
Results:
Of 103 patients, there were 37 cigarette smokers and 30 diabetic patients. Eighty-three patients achieved union of all involved joints and 19 patients achieved union of 1 or 2 joints. Smokers demonstrated a 1.46 (risk ratio) (95% CI 1.03-2.07) times greater risk of nonunion but were not at an increased risk of experiencing surgical complications (0.86, 95% CI 0.56-1.33). Diabetic patients did not demonstrate an increased risk of nonunion (0.86, 95% CI 0.56-1.33) or complications (1.18, 95% CI 0.76-1.83).
Conclusion:
Because of increased nonunion risk, patients undergoing elective tibiotalocalcaneal arthrodesis should be counseled increased nonunion risks associated with smoking. In this series, we did not find a relationship between diabetes and complications or nonunion.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
The tibiotalocalcaneal (TTC) arthrodesis remains a popular and effective surgical intervention in the management of numerous conditions affecting the foot and ankle. 11 TTC arthrodeses are successfully used in the management of acute and chronic conditions, including nonreconstructable fractures, end-stage arthritis, severe deformity, neuromuscular impairment, avascular necrosis of the talus, failed total ankle arthroplasty, and diabetic Charcot neuroarthropathy.4,6,7,9,15 The primary constructs used to achieve a solid TTC fusion are the retrograde intramedullary hindfoot fusion nail, the plate and screw construct, the screws-only construct, and the application of the ankle-spanning external fixator. Of these methods, the hindfoot fusion nail and the plate and screw constructs are the most often used. The hindfoot fusion nail, in particular, has become a popular choice given its increased rigidity, ease of insertion, and potentially less invasive surgical approaches. 1
Complications of arthrodesis procedures include superficial and deep infections, nonunion, malunion, symptomatic hardware, persistent pain, blood clots, and additional surgeries. Complications specific to the retrograde intramedullary nail include plantar heel pain at the insertion site, damage to the medial plantar nerve, tibial cortical hypertrophy, tibial stress fractures, and intraoperative tibial fractures. It is well established that smoking and diabetes are associated with increased incidence of complications following arthrodesis procedures about the foot and ankle.8,10,19 Patients who smoked were observed to have increased rates of nonunion and increased relative risk of nonunion.2,8 Patients with diabetic and Charcot neuroarthropathy were identified to have an increased risk of nonunion and an overall decreased amount of solid bony fusion.10,19
The purpose of this study was to evaluate fusion and complication rates following the use of a straight, retrograde intramedullary nail for TTC arthrodeses and to determine the influence of diabetes and smoking on these results. We hypothesized that diabetes and current cigarette smoking would be associated with increased rates of nonunion and overall complications.
Methods
Retrospective Chart Review
After obtaining approval for the retrospective review of patient records and radiographic images from our Institutional Review Board, the operative logs of the senior author were reviewed to identify patients who underwent a tibiotalocalcaneal arthrodesis with an intramedullary implant between October 2010 and November 2017. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were used in designing and reporting the study. 20 All preoperative orthopaedic diagnoses were included, and both diabetes patients and cigarette smokers were also included. Exclusion criteria included patients under age 18 years, patients with less than 3 months of postoperative follow-up, and patients without 3-month postoperative radiographs.
Preoperative medical records were reviewed for age at the time of surgery, gender, medical comorbidities, smoking history, body mass index (BMI), hemoglobin A1c levels, and preoperative and postoperative visual analog scale scores for pain. Preoperative pain scores were documented on the day of surgery, postoperative pain scores were documented at the final follow-up appointment. Perioperative and intraoperative records were reviewed for American Society of Anesthesiologists (ASA) status, type of anesthesia used, laterality, intraoperative complications, and concomitant procedures performed. Postoperative records were reviewed for duration of follow-up, postoperative visual analog scale pain scores, radiographic assessment of healing, additional surgeries performed, and complications.
Operative Technique
The majority of procedures were performed using regional anesthesia, although some patients received general anesthesia or general anesthesia and regional anesthesia. Thigh tourniquets were used, and patient positioning was determined by surgical approach. Anterior, lateral, and posterior surgical approaches were used during the study period, and this decision was made preoperatively based on the condition of the surrounding soft tissues. The lateral approach involved resection of the distal fibula, which was subsequently used as bone graft material. Anterior approaches to the ankle were performed in combination with a sinus tarsi incision to gain access to the subtalar joint, and posterior approaches were performed using a central Achilles splitting technique. All patients in this study received the same implant, the Smith & Nephew, Inc (Memphis, TN), Trigen Hindfoot Fusion Nail.
After exposure of the ankle and subtalar joints, the articular cartilage was entirely removed using sharp osteotomes and periosteal elevators. After removal of the articular cartilage on both sides of the joint, the subchondral bone was feathered with a 6-mm osteotome. If a lateral approach was performed, the resected fibula was morselized and mixed with demineralized bone matrix. This mixture was subsequently inserted into both joints. When anterior or posterior approaches were used, a mixture of cancellous allograft and demineralized bone matrix was inserted into the joints. Following joint preparation, the ankle was placed into neutral dorsiflexion, the hindfoot was placed into 5 degrees of valgus, and the external rotation was set to match the contralateral limb. While maintaining this position, a guide pin was inserted through a plantar heel incision just distal to the plantar fatpad. This pin was driven in a retrograde fashion across the ankle and subtalar joints, and into the tibial medullary canal. After confirming the pin’s position fluoroscopically, the pin was over-reamed with the entry reamer. The pin was removed and immediately replaced with a bulb-tipped guidewire that was sequentially reamed to exactly the proposed diameter of the nail (ie, a 10-mm reamer for a 10-mm-diameter nail). The intramedullary nail was inserted and the depth was confirmed fluoroscopically. Distal interlocking screws were placed through the attached jig, with the number and configuration based on the bony anatomy of the hindfoot. The joints were manually compressed by striking a mallet to the jig impactor attachment. One or 2 tibial interlocking screws were placed from medial to lateral through the jig’s outrigger attachment. After light irrigation, the wounds were closed in a layered fashion, and the patient was placed into a short leg fiberglass cast. All patients were made nonweightbearing for 6 weeks in a cast, followed by an additional 4-6 weeks of nonweightbearing in a fracture boot. Follow-up visits were initially scheduled at 3, 6, and 12 weeks, with additional follow-ups scheduled at 3- to 6-month intervals as needed. Anteroposterior and lateral view weightbearing radiographs were ordered for each visit, and computed tomography scans were only ordered to evaluate for potential nonunions. For weightbearing radiographs, union was defined as full callous formation or cortical bridging across the ankle and subtalar joints with no lucency between fusion surfaces. 12
Statistical Analyses
Prior to analyses, missing data were assessed as 3% for all variables; thus, complete case analyses were performed. Descriptive statistics were reported as mean (standard deviation) for continuous normally distributed variables, median (25th quartile, 75th quartile) for continuous nonnormal distributed variables, and percentage for count variables. Relative and absolute risk were assessed for smoking and diabetes status and fusion and surgical complications through risk ratios (RRs) and risk difference (RD) with 95% CIs. Risk ratio provides a relative risk calculation of the ratio of risk between the exposure group (ie, smokers) and the nonexposure group (ie, nonsmokers). Risk difference provides an absolute risk calculation that is the difference between the exposure group and unexposed group. Cox proportional hazards survival analyses were performed to assess the relationship between smoking, diabetes status, fusion, and surgical complications. Cox survival analyses were controlled for age, gender, and BMI. Linear regressions were performed to investigate the relationship between smoking, diabetes status, and change in pain. Linear regressions were also performed to investigate the relationship between smoking, diabetes status, and nonunion in relation to change in pain. Regressions were controlled for initial pain score, age, gender, BMI, and presence of comorbidities other than diabetes. Sensitivity analyses were performed to assess the stability of the results. A sensitivity analysis of posttraumatic arthritis was performed for all risk, survival, and regression analyses for smoking and diabetes status. All analyses were performed in R version 4.02 (R Core Team, 2013), using the dplyr package for cleaning and coding, epiR package for risk calculations, survival package for survival analyses, and the glm function for linear regressions.
Results
A total of 103 patients (Figure 1, Tables 1 and 2) were included.
Descriptive Statistics, Preoperative Diagnoses, Directions of Approach, and Concomitant Procedures.

Abbreviations: BMI, body mass index; IQR, interquartile range.
Preoperative Diagnoses, Direction of Approach, and Concomitant Procedures.

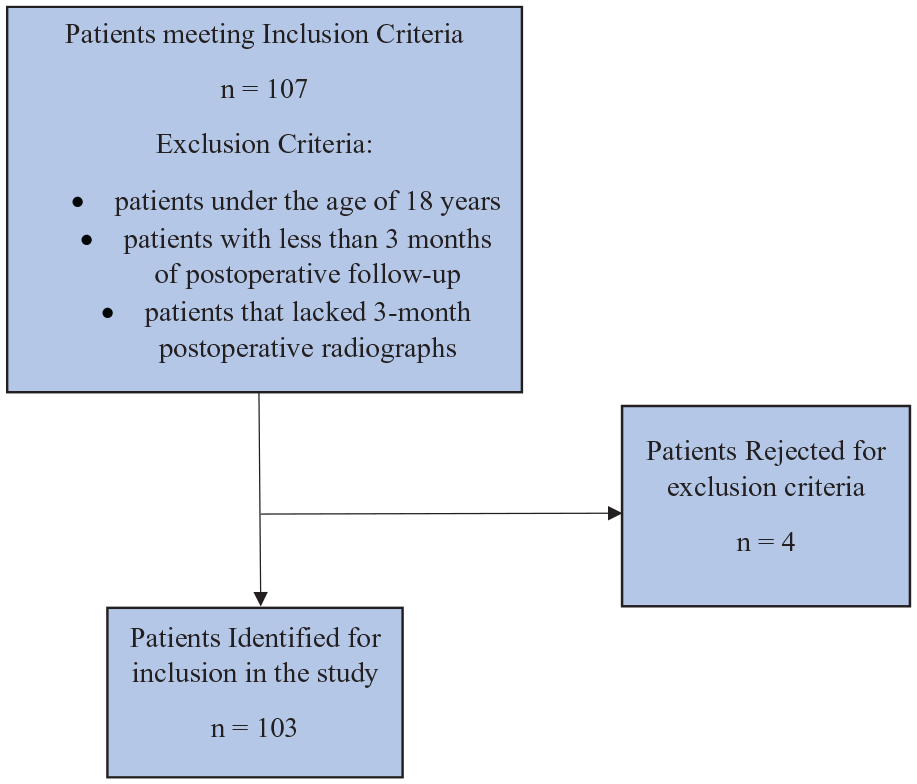
Patient selection.
Complications
Eight patients (8%) underwent revision procedures, and 18 patients (17%) underwent hardware removal (Figure 2). Six patients (6%) experienced superficial wound dehiscence, 6 patients (6%) experienced loosened hardware, and 3 (3%) had loosened screws removed.

Complications.
Patients who smoked were not found at an increased risk of experiencing complications (Table 3). Patients who smoked showed no difference in the time required to experience a complication (Figure 3). Patients with diabetes were not found at an increased risk of experiencing complications (Table 3). Patients with diabetes showed no difference in time to experience a complication (Table 4).
Risk Ratios and Risk Difference of Nonunion and Complications for Diabetic Patients and Smokers.
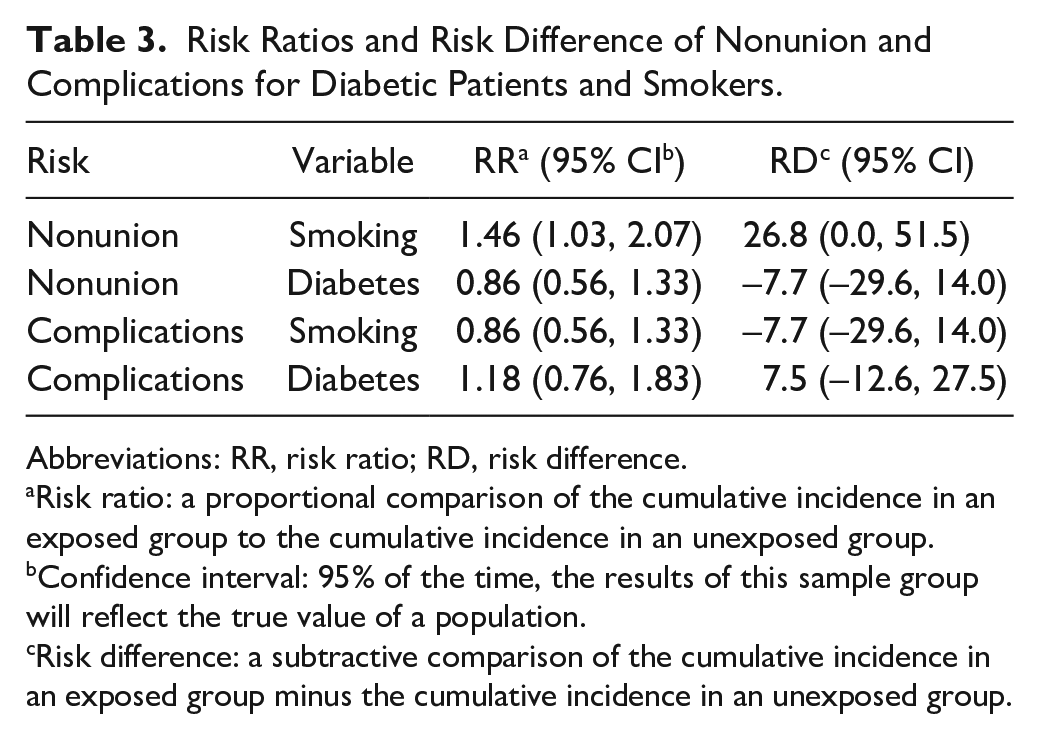
Abbreviations: RR, risk ratio; RD, risk difference.
Risk ratio: a proportional comparison of the cumulative incidence in an exposed group to the cumulative incidence in an unexposed group.
Confidence interval: 95% of the time, the results of this sample group will reflect the true value of a population.
Risk difference: a subtractive comparison of the cumulative incidence in an exposed group minus the cumulative incidence in an unexposed group.
Cox Survival Analyses.

Abbreviation: HR, hazard ratio.

Survival probability analysis of the relationship between smoking and fusion and surgical complications.
Nonunion
Patients who smoked were observed to have an increased risk of nonunion (calculated as risk of not achieving union at both joints) (Table 3). Time was not a factor in the association of smoking and nonunion (Figure 3). Patients with diabetes were not found to be at an increased risk of nonunion (Table 3). Time was not a factor in patients with diabetes’ risk of nonunion (Table 4).
Pain Scores
Patients who smoked were not found to have different changes in pain score (Table 5). Patients with diabetes were not found to have different changes in pain score (Table 5). Patients who did not achieve complete union were not found to have different changes in pain score (Table 5). These findings held consistent after controlling for preoperative pain score, age, gender, BMI, and other comorbidities (Table 5).
Pain Score Linear Regression.

Sensitivity Analyses
Patients who smoked had elevated risk of nonunion, both in patients with posttraumatic arthritis (RR 1.58, 95% CI 1.06-2.36) and patients with all-cause (all patients, not just those with posttraumatic arthritis) injuries (RR 1.46, 95% CI 1.03-2.07), suggesting smoking status impact was independent of injury cause. Patients with diabetes did not demonstrate elevated risk of nonunion events, both in patients with posttraumatic arthritis (RR 1.59, 95% CI 0.84, 3.01) and patients with all-cause injuries (RR 0.86, 95% CI 0.56, 1.33), suggesting diabetes impact was independent of injury cause. We examined the impact of posttraumatic arthritis vs all-cause injuries in patients who smoked and with diabetes to assess the impact of injury cause on the risk of developing complications. Among patients who smoked, we detected elevated risk of surgical complications in patients with posttraumatic arthritis (RR 1.75, 95% CI 1.29, 2.32), although not for all-cause injuries among patients who smoked (RR 0.86, 95% CI 0.56, 1.33). This suggests that patients with posttraumatic arthritis who smoke are more likely to experience surgical complications than all-cause injuries in smokers. Patients with diabetes did not demonstrate an elevated risk of surgical complications, both in patients with posttraumatic arthritis (RR 1.06, 95% CI 0.59, 1.90) and patients with all-cause injuries (RR 1.18, 95% CI 0.76, 1.83), suggesting that among patients with diabetes, risk of surgical complications is not influenced by injury type.
Discussion
Ultimately, 81% of patients achieved union of all joints; an additional 18% of patients achieved union of 1 or more joints. Patients who smoked had a 1.46 times greater risk of nonunion. Although smokers had an increased risk of nonunion, time to event was not associated with union (Figure 3). One patient achieved union after 37 months of follow-up.
More than half of patients experienced a complication with the procedure. Our findings initially suggested an increased rate of complications (50.5%) compared with a previous multicenter hindfoot arthrodesis nail (HAN) study (23.7%, 95% CI 11.4-40.2) 16 ; however, our study included a broader criteria for complications, including partial nonunion (union of one joint [ankle or subtalar] but nonunion of the other), intraoperative bone fracture, and postoperative acute respiratory failure. Matching our criteria to the HAN study reduces our complication incidence to 37%, which was similar. A smaller study conducted by Pinzur and Noonan 15 noted a complication incidence of 22%. Our study’s sample size of 103 compared to the smaller (38) multicenter HAN study may contribute to these differences. A multisurgeon study of 154 tibiotalocalcaneal fusions with postoperative bone stimulators demonstrated postoperative infection incidences of greater than 27%. 3 Our postoperative infection rate was 6.8%. In evaluating the outcomes and complications of hindfoot arthrodesis nail procedures, it is important to remember it is salvage maneuver, intended to address hindfoot and ankle complications that could not be managed otherwise. 17 Thus, outcomes may vary substantially from those seen in nonsalvage procedures. Our study is reflective of our institution’s role in serving patients in a multistate region, often requiring hours of travel, suggesting that the impact of patient access to care on outcomes may represent an area for future study.
Two primary variables we examined were patients with diabetes and patients who smoked. Thirty patients (29.1%) had diabetes, a similar prevalence to previous research, 13 suggesting increasing generalizability of our results. Recent literature from Myers et al demonstrated improved outcomes and fewer surgical site infections in diabetic patients with tight, long-term glycemic control. 13 Our patients’ hemoglobin A1c values ranged from 5.1 to 14.6 (mean, 7.6; median 7.0), but our statistical analysis showed no differences between diabetic and nondiabetic patients. Lack of difference may also be attributable to a type 2 error. Traditionally, patients are expected to maintain tighter glucose management to minimize the risk of complications 21 ; however, this expectation was not supported by our findings, suggesting that diabetic control is not the only factor in surgical outcomes and representing an area for future research. We identified a difference in the risk of nonunion between all smoking patients and smoking patients with posttraumatic arthritis (RR 1.58, 95% CI 1.06-2.36). These results are consistent with meta-analyses on the risks of nonunion in smokers after fracture, osteotomies, or arthrodesis. 14 The meta-analysis suggests smoking cessation prior to surgery is beneficial for fracture healing; however, there exists a limited amount of data from which to draw this conclusion. The reasons for the efficacy of smoking cessation prior to surgery remain topics for further investigation. Patients with diabetes and patients who smoked were hypothesized to experience increased complications and nonunion and decreased change in pain scores. Our study only reflected an increased risk of nonunion events in patients who smoked, and an increased risk of postoperative complications in patients with posttraumatic arthritis who smoked. This divergence in expectations and outcomes represents areas for future exploration.
Patients who smoked and patients who smoked and had posttraumatic arthritis showed increased risk of nonunion (Table 3). This suggests the impact of smoking status on a patient’s risk of nonunion is independent of the patient having posttraumatic arthritis. We did not detect a difference in risk of nonunion in patients with diabetes and posttraumatic arthritis and among all-cause injuries. This indicates patients’ diabetic status and their risk of nonunion were independent of posttraumatic arthritis. Future studies should evaluate the risk associated with nonunion in specific joints in TTC arthrodesis.
Patients who smoked and had posttraumatic arthritis showed increased risk of postoperative complications compared with smokers with all-cause injuries (Table 3). This suggests that the impact of smoking status on a patient’s risk of complications may be related to comorbid posttraumatic arthritis. Evaluation of whether this relationship is correlative or causative represents an area for future study. Diabetic patients did not have a difference in risk of postoperative complications among patients with posttraumatic arthritis and all-cause injuries. This indicates patients’ diabetic status and risk of postoperative complications were independent of posttraumatic arthritis.
At this time, there are no data indicating ideal timing for a salvage procedure. Historically, patients have exhausted all options before a salvage procedure; however, more research should be done to determine if patient outcomes improve based on age at the time of surgery. Such a study would be difficult, given the prevalence of confounding comorbidities (diabetes, peripheral arterial disease, smoking, and isolated neuropathy). It would be difficult to find large cohorts who met the target ages but did not also have excessive confounding variables. Previous studies 18 using early arthrodesis in patients with early-stage Charcot joints showed reasonable success; however, they are not considered standard of care.
Strengths of this study are its large sample size, the diversity of patient ages at the time of surgery (range, 21-82 years), and the diversity of patient comorbidities, all of which increase the study generalizability. To our knowledge, 5 our study contains the largest analyzed sample of tibiotalocalcaneal fusion procedures performed by a single surgeon at a single institution. Another strength is the length of follow-up; one patient ultimately achieved fusion at 37 months, which suggests the healing process may continue even 3 years after surgery. Other strengths include the definitions of surgical outcomes; by considering partial unions separately from complete union and complete nonunion, we acknowledge the reality of salvage procedures—as a last-resort measure with highly variable outcomes. Our consideration of partial unions may also help lay the groundwork for studying factors that influence the rates of fusion within specific joints in TTC arthrodesis.
A limitation of this study is a lack of a control group; however, in a salvage procedure without definitive standard protocol, it would be difficult to select a single procedure as a control. Additionally, it would be inappropriate to perform a sham procedure on patients in need of intervention when we have reliable data that tibiotalocalcaneal arthrodesis by an intramedullary nail can improve outcomes in patients. 17 Another potential limitation of this study was that it did not consider the functionality of patients following the procedure. Although preoperative, postoperative, and the change in pain scores were documented and analyzed, they were not used in conjunction with data on the patients’ ability to return to work or other activities. Without these data, it is difficult to fully assess the outcomes and long-term impact.
Conclusion
This study demonstrates that smokers are at higher risk than nonsmokers of nonunion following tibiotalocalcaneal arthrodesis using an intramedullary hindfoot nail. Smokers with posttraumatic arthritis were noted to have higher risk of postoperative complications compared to all-cause injuries. In contrast to similar studies, our study demonstrated no difference in the risk of complications or nonunion in patients with diabetes; however, this may be due to the risk of Type 2 error. Time to event was not found to be a factor in the risk of nonunion between patients who were smokers and nonsmokers. Patients undergoing elective tibiotalocalcaneal arthrodesis with a hindfoot nail should be counseled on increased risks of smoking.
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Wake Forest School of Medicine Institutional Review Board (IRB00061644).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Smith & Nephew, Inc, payment made to Wake Forest Baptist Health Department of Orthopaedics. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All support for the present manuscript (eg, funding, provision of study materials, medical writing, article processing charges, etc). No time limit for this item: Smith & Nephew, Inc; payment made to Wake Forest Baptist Health Department of Orthopaedics.