
Abstract
Purpose
End-stage ankle arthrosis causes severe pain and limited movement. Tibiotalocalcaneal arthrodesis with arthroscopy-assisted hindfoot nailing can be used to achieve a high union rate and low complication rate. We aimed to examine the early- and mid-term results of patients treated with this technique from various perspectives and to evaluate them by comparing them with the current literature.
Methods
Data were collected from 25 patients who met the established criteria and underwent TTCA with arthroscopic-assisted hindfoot nailing. In addition to the demographic data of the patients, their clinical and pain scores were evaluated using the American Orthopedic Foot and Ankle Society (AOFAS) and visual analogue scale (VAS). Additionally, the union time and complication data during the follow-up period were examined.
Results
When the AOFAS and VAS scores of the 25 patients were examined, a significant improvement was observed in the preoperative period and early postoperative period comparisons (p < .001). No significant change was observed between the comparison of the postoperative 12th month and last postoperative control clinical scores. While the union rate of the patients was observed to be 92%, the average union time was 13.1 ± 3.5 weeks. During follow-up, peri-implant fracture, deep infection, and non-union were observed in one patient each (12%).
Conclusion
The early- and mid-term postoperative results of patients treated with TTCA surgery with posterior approach arthroscopic-assisted hindfoot nailing show that this technique may be an option with low complication and high union rates for the appropriate group of patients planned for ankle arthrodesis.
Introduction
End-stage osteoarthritis of the ankle joint is often associated with extreme pain and severe functional limitation. 1 First-line treatment includes conservative options such as activity modification, orthotic devices to immobilize the ankle, and nonsteroidal anti-inflammatory medications. Arthrodesis remains clinically accepted as the gold standard for end-stage ankle arthritis that does not respond to conservative treatments.2,3
Tibiotalocalcaneal arthrodesis (TTCA) is a surgical procedure that aims to restrict tibiotalocalcaneal joint movement and relieve pain caused by ankle movement. Indications for TTCA include osteoarthritis, talar osteonecrosis, chronic inflammatory diseases, diabetic neuropathic arthropathy, chronic ankle instability, talocrural arthroplasty or arthrodesis failure, and neurological deformities that make plantigrade positioning and stable walking in the hindfoot impossible. 4
Traditionally, open ankle arthrodesis has been accepted as the basic treatment technique, and various approaches have been described in previous studies. 5 Although most open surgical methods have achieved good curative effects, they are associated with several complications.6,7 These complications of open ankle fusion have led to the development of less invasive techniques such as arthroscopic ankle fusion. 8 Many studies suggest that arthroscopic ankle fusion has advantages such as faster union time, lower morbidity, lower blood loss, faster rehabilitation, and shorter length of stay than open surgery.9–12 These advantages of arthroscopic ankle fusion are believed to be due to the fact that periosteal stripping is not required and local circulation remains intact, creating a more favorable environment for fusion to occur. 13
Various implants and surgical techniques are available for the treatment of TTCA. In terms of implant selection, biomechanical studies have demonstrated the superiority of intramedullary nails over screws, plates, and external fixators.14–17 Regarding the surgical technique, the majority of TTCA cases performed with nails are open surgeries. 18
In line with this information, we decided to examine the effectiveness of the arthrodesis procedure achieved with the posterior arthroscopic technique and hindfoot nailing, as well as the possible risks and benefits of the method used. We planned to evaluate the functional scores, radiographic results, and complications in a series of patients treated with this technique. The aim of this study is that the posterior approach arthroscopy-assisted TTCA surgery with hindfoot nailing would provide effective and preferable results in the early and mid-term postoperative periods.
Materials & methods
Participants
Data of patients diagnosed with tibiotalar and subtalar arthrosis who underwent TTCA with arthroscopy-assisted hindfoot nailing were collected retrospectively between January 2016 and December 2019. The study was conducted in accordance with the ethical standards of the 1964 Helsinki Declaration, as revised in 2000. Appropriate Local Ethics Committee approval and written informed consent were obtained.
Patients aged between 20 and 80 years whose complaints related to arthrosis persisted for at least 6 months and who did not benefit from conservative treatment during this period were included in the study. All patients included in the study had arthritic changes of varying severity in the tibiotalar and subtalar joint regions. Hindfoot nailing was also applied to patients with tibiotalar region arthrosis and arthritic changes in the subtalar region that were not at the level of end-stage arthrosis. All patients were informed that ankle-hindfoot joint movements would be restricted after surgery, and informed consent was obtained. Additionally, clinical and gait analysis studies show that protecting the subtalar joint does not make a significant difference in similar situations.19,20 Patients who did not have a follow-up period of at least 18 months, who had missing clinical or radiological data during this period, who had evidence of deep ulceration or osteomyelitis, or who had significant malalignment requiring osteotomy were excluded from the study. A total of 14 of the 39 patients who underwent this surgery were excluded from the study, including three cases with additional pathologies and 11 cases with insufficient follow-up time or data.
Information regarding the patient’s age, sex, operated side, and length of hospital stay was collected from the patient data. The Charlson Comorbidity Index (CCI) was calculated for each patient. Preoperative and postoperative 3-month, 12-month, and final follow-up (18–24 months) visual analog scale (VAS) and American Orthopedic Foot and Ankle Society (AOFAS) scores were retrospectively collected. Owing to the restriction of ankle movements of the patients after surgery, the highest AOFAS score was taken into account as 86/100. Antero-posterior and lateral ankle radiographs of the patients taken during routine control periods were examined. Unions in the tibiotalar and subtalar joints were monitored using evaluations performed by the same person. If cortical bridging was observed in at least three (anterior-posterior-medial-lateral) planes in both joint regions, this was considered a union.
Surgical technique and rehabilitation
All surgeries were performed using the same approach by the same surgeon with more than 15 years of experience in foot and ankle surgery. Prophylactic antibiotics were administered before surgery and appropriate medical thromboembolism prophylaxis was continued following surgery.
Surgery was performed under spinal anesthesia. A tourniquet was wrapped around the thigh area, the appropriate preparation was completed in the prone position, and no traction was applied. Their feet and ankles were placed away from the operating table to facilitate easier maneuvers and better fluoroscopic control during the surgical procedure.
While the patient was in the prone position, the medial and lateral portals were opened 1 cm above the intersection of the lines drawn horizontally from the lateral and medial malleoli, and longitudinally from the medial and lateral Achilles tendons. After opening the portals, the fatty tissue on the back of the ankle was cleaned using a shaver. Then, the os trigonum and flexor hallucis longus (FHL) tendons were identified. The synovial tissues around the FHL tendon were cleaned, and the os trigonum, if present, was excised. The posterior talofibular and transverse tibiofibular ligament tissues were resected from the posterior ankle capsule.
Subsequently, the cartilage tissue was excised from both the tibiotalar and subtalar joints with open and closed curettes. The ankle was placed in maximum dorsiflexion, particularly for cartilage excision in the anterior part of the talus. The anterior vascular nerve bundle was preserved using the anterior capsule as a reference. To avoid damage to the tibialis posterior artery and nerves, care was taken not to distort the subtalar joint line.
After these procedures were completed, arthroscopy was terminated, and the longitudinal intersection points of the anterior and lateral tibia were determined using fluoroscopy under the guidance of the Kirschner wire. An incision was made, using the intersection point on the heel as a reference. The entry guide of the nail was advanced such that it reached the center of the tibial medulla. After reaming with the entry reamer, a hindfoot nail of the appropriate size (Trigen Hindfoot Arthrodesis Nail; Smith & Nephew) was placed using an external guide. The locking process was completed by placing the proximal locking screw with the distal screws. Weight bearing was restricted to the operated side for 3 weeks after surgery. During follow-up, after wound control was completed, weight-bearing was allowed on the surgical side.
Statistical analysis
The data obtained in this study were statistically analyzed using IBM SPSS Statistics version 20. The arithmetic mean, standard deviation, and median were used as continuous variables, and counts and percentages were used for categorical measurements. The Shapiro–Wilk test was used to evaluate the normal distribution of the preoperative and postoperative scores obtained using the AOFAS and VAS scoring systems. After normality analysis, repeated measures ANOVA and Friedman test were used for time-dependent comparison of the data, and pairwise comparisons were made with the Wilcoxon test. The Bonferroni test was used for post hoc analyses. p-values < 0.05 were used to detect statistically significant differences between mean values.
Results
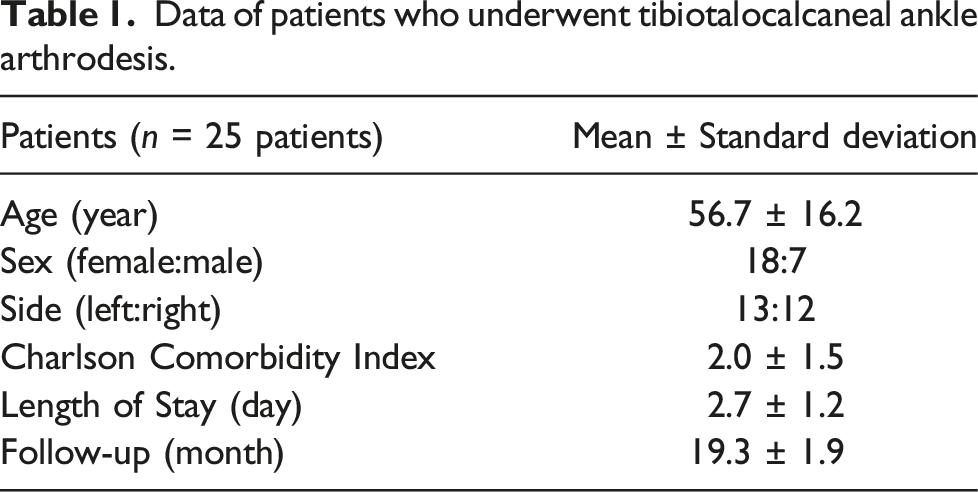
Data of patients who underwent tibiotalocalcaneal ankle arthrodesis.
The values of AOFAS and VAS scores by time.

Data are shown as mean ± standard deviation AOFAS: American Orthopaedic Foot and Ankle Society VAS: Visual Analog Scale.
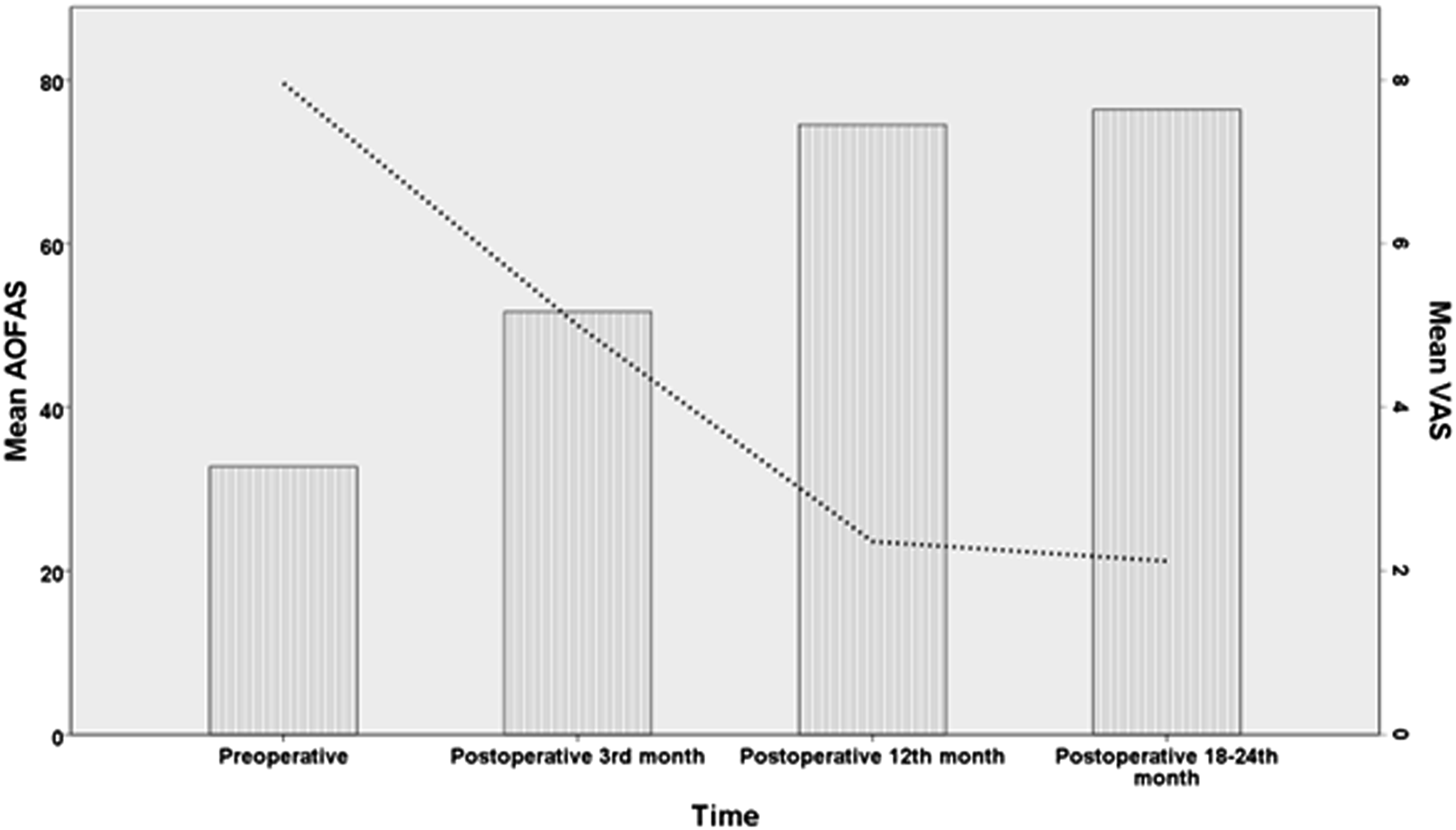
Dual axes graph presents the time-based results of AOFAS and VAS scores. Bars show mean values of AOFAS scores, interpolation line shows mean values of VAS scores. AOFAS: American Orthopaedic Foot and Ankle Society, VAS: Visual Analog Scale.
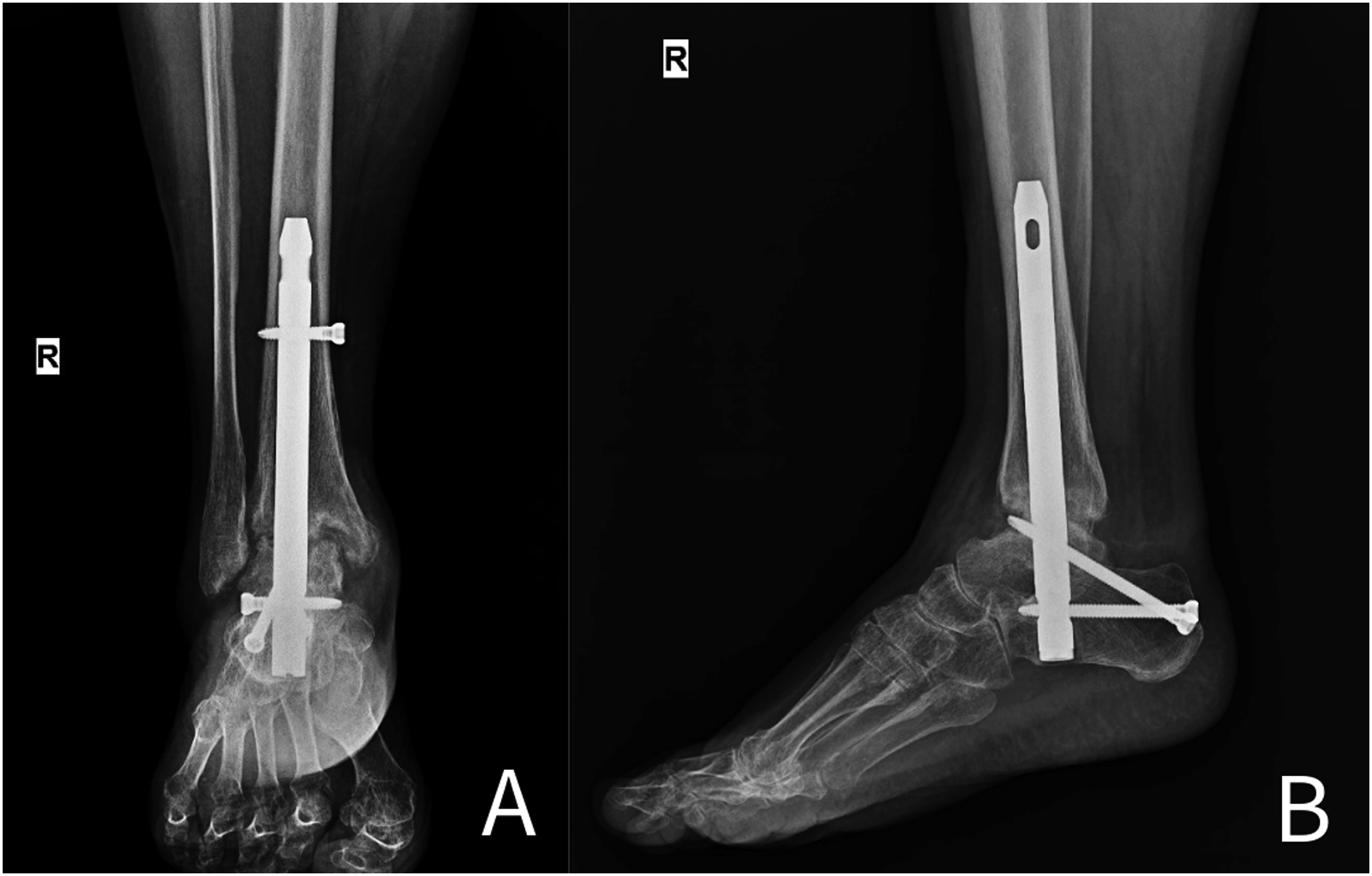
During the follow-up period, major complications developed in three patients (12%), and minor complications developed in two patients (8%). In one patient, a fracture occurred in the proximal hindfoot nail in the 3rd postoperative week, and revision surgery was performed using a longer nail. In another patient, an infection was observed in the early postoperative period. The nail was removed, a Kirschner wire coated with antibiotic cement was placed, and intravenous antibiotic therapy was administered for 6 months. When there were no signs of infection after 3 months, the antibiotic cement was removed and hindfoot nailing was performed again. Additionally, non-union was observed in one patient during follow-up, and as the patient’s complaints continued, plate fixation surgery was performed using an autograft. Except for these last two patients, bone union was observed in all patients (92%). Although union was observed in these patients during the follow-up period, these data were not included in the average time to union. The average time to union was calculated as 13.1 ± 3.5 weeks. Preoperative radiographs, intraoperative arthroscopic images, and early and late postoperative radiographs are shown in Figures 2–5. Cases with minor complications were screw-related and the displaced distal locking screws were removed, which did not cause any pathologies related to bone union or stability. Preoperative antero-posterior (A) and lateral (B) right ankle radiographs. Intraoperative arthroscopic view after debridement. Postoperative 4th week antero-posterior (A) and lateral (B) right ankle radiographs. Postoperative 3rd month antero-posterior (A) and lateral (B) right ankle radiographs.


Discussion
Arthrodesis remains clinically accepted as the gold standard for end-stage ankle arthritis that does not respond to conservative treatment. 2 Traditionally, open ankle arthrodesis has been accepted as the mainstay of treatment and various surgical techniques have been described previously. 5 Owing to technological advances for arthroscopic techniques for ankle arthrodesis have only emerged in recent years. Arthroscopic techniques are becoming increasingly popular as foot and ankle surgeons gain experience in minimally invasive surgeries. 11 Our study was planned in light of this information, and TTCA was performed with arthroscopy-assisted hindfoot nailing in appropriate patients and was completed with positive clinical results. To the best of our knowledge, this study is one of the largest and longest follow-up case series performed using this method.
The debate continues regarding the best technique and material selection for ankle joint fixation surgery. Screw fixation has been suggested as the preferred procedure because of its ease of application and significant union rates. 21 Fixation with a plate is another option. In a systematic review of 164 patients, Kusnezov et al. reported a union rate of 97.6%. 22 In a study comparing plate and screw fixation, although no significant difference was observed in terms of the functional score during follow-up, the union time in screw fixation was longer than that in plate fixation. TTCA with hindfoot nails is another option. 23 In a cadaver study comparing intramedullary nail, screw, and plate fixation techniques, Hamid et al. found that the compressive force in screw fixation was less than that in other techniques. 24 It has been stated that the choice of intramedullary nail or plate may be considered in this region where compression is targeted. In a recent study comparing these three techniques, 42 patients were retrospectively examined. 14 Although van den Heuvel et al. did not encounter any complications in the patient group in which intramedullary nailing was applied, a significantly higher infection rate was observed in the plate fixation group. In our study, non-union and infection were observed in one patient each, and our results show that the desired results can be achieved with the hindfoot nail technique.
Comparisons of implants in the literature have been performed for open surgery; however, the arthroscopic technique has not yet been examined. In general, the arthroscopic technique promises lower morbidity and mortality, faster recovery, shorter hospital stay, and fusion time by minimizing soft tissue disruption. In their prospectively collected data, Woo et al. examined 28 patients who underwent arthroscopic TTCA and matched them to 56 patients who underwent open arthrodesis. 11 In the 2-year follow-up results, the arthroscopic technique was found to be statistically superior to the open technique in terms of the clinical functional score (AOFAS), frequency of postoperative complications, and length of hospital stay. Quayle et al. retrospectively examined patients who underwent 29 open and 50 arthroscopic ankle arthrodesis surgeries. 12 In the data evaluated during at least 1 year of follow-up, the frequency of complications was higher and the bone union time was later in the open surgery group. Systematic reviews and meta-analyses have also been conducted for comparison. In a review of six studies, Chandrappa et al. reported a higher union rate, shorter tourniquet, and shorter hospital stay in arthroscopic surgery; however, no significant difference was found in other aspects. 25 In another review conducted using data from seven retrospective studies, a higher clinical score, fewer complications, reduced blood loss, and shorter hospital stay were found with the arthroscopic technique. 26 In the most recent large-scale meta-analysis, Xing et al. showed that arthroscopic ankle arthrodesis was superior to open ankle arthrodesis alone in the treatment of ankle arthritis in terms of overall complication rate, intraoperative tourniquet time, hospital stay, non-union rate, and fusion rate. 27 However, in studies in which the arthroscopic approach was evaluated, fixation with screws was preferred for implantation, and the hindfoot nail used in our study was not examined.
In the literature, there have been few studies on TTCA with arthroscopic-assisted hindfoot nailing, with varying limitations, and a recent review attempted to report general results. 28 After examining the data of 65 patients in five studies, a significant increase in clinical scores was observed, with a major complication rate of 13.8%. Additionally, bone union was observed in 86% of the patients at an average of 12.9 weeks. Although all studies were arthroscopically assisted by the TTCA, there were technical differences. Only two of these five studies were performed with an isolated posterior approach, as in our practice, and the number of cases was six and seven, respectively.4,29 In the technical details of these studies, Mencière et al. applied percutaneous Achilles tenotomy, while Guerra Alvarez et al. added fibular osteotomy as a standard to the surgery. In these studies, the major complication rates were 17% and 29%, and the union times were 11.7 and 10 weeks, respectively. In our study, the incidence of major complications was lower (12%); however, the duration of union was longer at 13.1 weeks, which may be associated with additional surgical steps such as tenotomy and osteotomy. However, the bone union percentage and time were similar to those reported in the review study. Our study is the largest and longest follow-up study on posterior approach arthroscopic surgery.
This study has some limitations that warrant discussion. First, there was no control group; that is, there was no group in which open surgery or other arthroscopic approaches were applied. Although the technique we applied has been shown to be effective in the postoperative period, it is not appropriate for us to make a judgment on the superiority of other treatment options. Another limitation is that not all patients with hindfoot pathologies were included in the study. Patients who underwent this surgery did not plan to undergo additional osteotomy, which may have affected the results. As another limitation, we can mention radiological evaluations. In the postoperative period, only fusion evaluation was performed by a single investigator using plain radiographs. In future larger studies, fusion and alignment can be investigated with computed tomography, and the reliability of radiological evaluation can be increased with multi-practitioner measurement.
Conclusion
TTCA surgery with posterior approach arthroscopic-assisted hindfoot nailing can be used to reduce the occurrence of common complications in traditional procedures. Therefore, the satisfactory clinical results of the patients in this study using the arthroscopic technique show that this method can be used effectively. Large-scale prospective comparative studies of ankle arthrodesis surgical techniques may reveal the advantages of these techniques.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.