
Abstract
Background:
The Ponseti method is today’s standard treatment of idiopathic talipes equinovarus (ITEV). Compliance with foot abduction bracing (FABO) and socioeconomic factors have been shown to impact treatment outcome. We wished to further study socioeconomic factors using the Area Deprivation Index (ADI), a more comprehensive way to evaluate socioeconomic status, which has not been done before.
Methods:
All TEV patients from 2010 through 2019 treated with the Ponseti method were reviewed. Standard demographic variables, as well as the number of casts to complete initial correction, FABO compliance, and occurrence of relapse were tabulated. Socioeconomic level was quantified with the 2018 ADI.
Results:
There were 168 children; 151 had typical and 17 complex TEV. Average follow-up was 4.3 ± 1.8 years; relapse occurred in 46%. There were no significant differences in the percentage of relapse by sex, race, or ADI. FABO noncompliance was present in 46%. Relapse increased with increasing time of follow-up and FABO noncompliance (76% vs 21%, P < 10−6). Multivariate logistic regression analysis revealed that only FABO compliance and length of follow-up were associated with relapse. The OR of relapse for FABO noncompliance was 17.9 (7.6, 42.4, P < 10–6) and for follow-up >4 years the OR was 4.97 (2.1, 11.70, P = .0003).
Conclusion:
The outcome of the Ponseti method for TEV treatment is dependent on local circumstances. In our state, socioeconomic status, as determined by the ADI, was not associated with the occurrence of relapse. Thus, each center needs to assess its results, and analyze its own reasons for relapse. There were no other demographic variables associated with relapse except FABO compliance and length of follow-up. Parents should be strongly advised that FABO compliance and follow-up appears paramount to achieving the best results, and that complex TEV are at greater risk for relapse.
Level of Evidence:
Level IV, case series
Clubfoot, or talipes equinovarus (TEV), is a well-known congenital deformity, and can be either an isolated idiopathic deformity (ITEV) or associated with various syndromes. 37 Within the ITEV group, it can be either typical or complex.25,32,49 Complex clubfeet are those having rigid equinus, severe plantar flexion of all metatarsals, a deep crease above the heel, a transverse crease in the sole of the foot, and a short hyperextended first toe. 32 The current preferred treatment for both typical and complex idiopathic TEV is the Ponseti method8,24,26,43,50 with overall successful outcomes worldwide.
Relapse is common 12 and often needs further treatment (repeat casting, repeat Achilles tenotomy, tibialis anterior tendon transfer, and rarely more extensive surgery). Reported relapse rates in the literature vary from 22.7% to 68%.5,24,34,38,50 Relapse is associated with compliance of nighttime abduction bracing. 8 Compliance can be dependent on many issues: parental education level, 8 socioeconomic status (transportation difficulties), 33 and cultural/ethnic interpretation of the bracing instructions.2,27,33 It was the purpose of this study to analyze our outcomes with the Ponseti method in the treatment of ITEV. We specifically wished to (1) study the effect of socioeconomic status on ITEV relapse at our institution by utilizing the Area Deprivation Index (ADI) in our state of Indiana and (2) determine any variables associated with relapse at our center. The ADI is based on a measure created by the Health Resources and Services Administration and has been recently refined and adapted to the US Census block group/neighborhood level. This allows for rankings of neighborhoods by socioeconomic disadvantage, which is more granular than using zip codes, as there can be many neighborhoods in one zip code. It includes factors for the domains of income, education, employment, and housing quality. It has been used extensively across medicine; a few such examples are in chronic medical diseases,17,19,42,48 trauma,16,45 joint arthroplasty,14,28 and pediatrics/pediatric orthopaedics.3,4,21,23
Materials and Methods
This was a single cohort retrospective review of all ITEV patients treated at our institution, along with using a national database for the determination of socioeconomic status. The electronic medical records for all patients with TEV seen at our tertiary referral children’s hospital for the years 2010 through 2019 were searched. As it was unknown if those providers who initiated treatment outside of our institution were trained in the Ponseti method, such cases were excluded. All 6 of the attending surgeons at our institution over the time period studied were trained in the Ponseti technique. Although the Ponseti method works well in untreated, older children,10,22,41,44,47 we wished to keep this study homogenous, and therefore excluded those children initially treated at another institution, after 6 weeks of life, and children from other states.
All children were treated using the Ponseti method.6,30,31 All of the cast applications and the percutaneous Achilles tenotomy were performed by the attending physician or with the attending physician personally supervising a trainee. The percutaneous Achilles tenotomy was either performed in the outpatient clinic with local anesthesia or in the operating room with general or spinal anesthesia. 1 Post tenotomy, a cast was applied for 3 weeks, after which the foot abduction orthosis (FABO) was fitted by a certified orthotist. The FABO used was the Mitchell-Ponseti foot abduction brace. 32 The FABO was prescribed to be worn 22 hours a day for the first 3 months post tenotomy, and then at bedtime and naps thereafter until age 4 years. Relapse was defined to have occurred when the attending orthopaedic surgeon recommended to the family that further casting and/or surgery be performed, regardless of whether it actually happened. Noncompliance with the FABO was when the caregivers stated such, when the Department of Social Services became involved regarding issues of compliance, and when in the physician’s opinion the Mitchell shoes showed no signs of wear after 6 months of being prescribed. The presence of relapse was not used as a proxy for noncompliance as relapse can occur with compliant FABO wear.8,15,24 Temperature monitors inside the shoes were not the standard of care in our practice during the time of data collection, 39 and reported hours of wear by the parents was not used as it is known that the reported hours differ from the actual hours by the temperature monitor study of Sangiorgio et al. 39 Noncompliance was managed by many different ways, including changing the abduction angle of the FABO, physiotherapy, and repeat casting.
We recorded the child’s sex, race, type of idiopathic TEV (typical vs complex) 32 , laterality, and number of casts to achieve successful, initial correction. The number of casts to achieve initial correction included the cast applied at the time of tenotomy. Race was self-described by the parent or guardians of the child. The designation of the TEV being typical or complex was made by the attending orthopaedic surgeon on clinical grounds using the definition as described in the introduction 32 ; no radiographs were used in this determination. Those with <2 years of follow-up were excluded.
The socioeconomic level of the patient/family is known to impact compliance and thus treatment outcome.2,8,27,33 In this study, the socioeconomic level of the patient/family was assessed using the 2018 Area Deprivation Index (ADI) 18 from the Neighborhood Atlas Mapping project. The 2018 version was used as the 2015 first version was not readily available online. The ADI is a validated tool that measures economic disadvantage using 17 variables related to income, employment, education, and housing, resulting in a composite average socioeconomic status of a population within a given neighborhood.9,17,19 Both state and national decile/percentiles for the ADI can be obtained. For the purposes of this study, state ADI deciles of 1 to 3 were labeled as lowest deprivation, deciles of 4 to 7 as mid-deprivation, and deciles of 8 to 10 as highest deprivation. The study was approved by our local institutional review board.
Statistical Analysis
Continuous variables are expressed as the mean ± 1 standard deviation. Categorical variables are expressed as frequencies and percentages. Differences between continuous variables were analyzed using nonparametric statistics because of nonnormal distributions (Mann-Whitney U test: 2 variables; Kruskal-Wallis test: 3 or more variables). Differences between categorical variables were analyzed by the Fisher exact test (2 × 2 analyses) and the Pearson χ2 test (greater than 2 × 2 analyses). Predictors of relapse were determined using logistic regression analysis, both univariate and multivariate. For the multivariate analysis, a backwards stepwise estimation was used. Entry into the model was set for all bivariate analyses with a P <.20 and exit from the model for all P >.05. The odds ratio (OR) for relapse along with the 95% confidence interval of the OR are reported. All analyses were performed with Systat 10 software. A P <.05 was considered statistically significant.
Results
There were 318 children with idiopathic TEV initially treated at our institution within the first 6 weeks of life that met the inclusion criteria; 168 had at least a 2-year follow-up. Of these 168 children, 151 had typical and 17 complex TEV (Table 1). The average follow-up was 4.3 ± 1.8 years and average age at follow-up 4.4 ± 1.8 years. Relapse occurred in 78 (46.4%) of children at final follow-up; FABO noncompliance was present in 77 (45.8%).
Demographics of Clubfoot Patients Treated by the Ponseti Method Separated by the Occurrence of Relapse and Compliance With Post-tenotomy Bracing. a
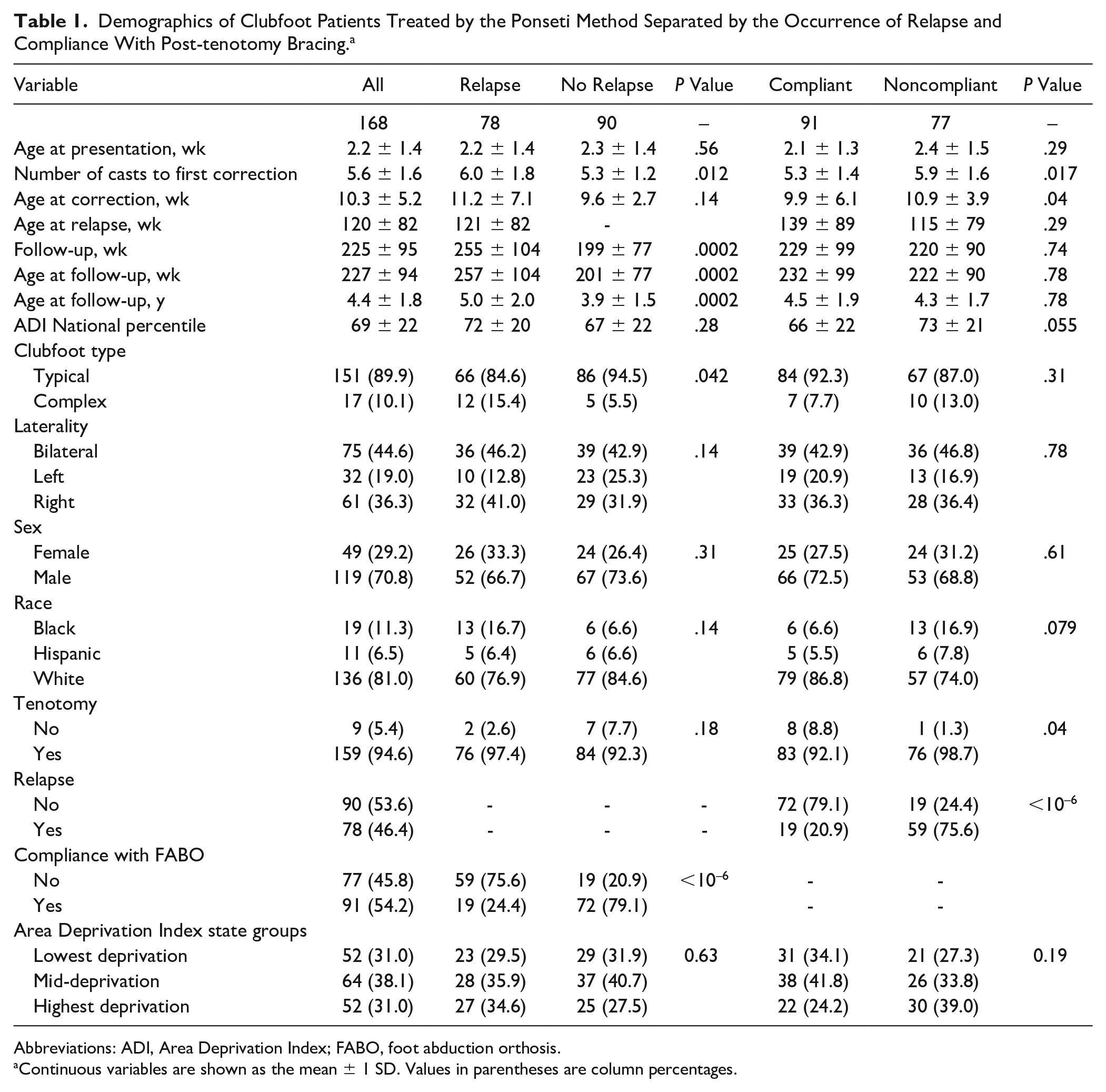
Abbreviations: ADI, Area Deprivation Index; FABO, foot abduction orthosis.
Continuous variables are shown as the mean ± 1 SD. Values in parentheses are column percentages.
Relapse increased with increasing time of follow-up (Figure 1). Relapse was greater (Table 1) in those needing more casts to reach initial correction (6.0 vs 5.3; P = .012), and noncompliance with the FABO (75.6% relapse in the noncompliant group vs 20.9% in the compliant group; P < 10–6). There were no significant differences in the percentage of relapse by sex, race, or ADI. There were no differences between the FABO compliant and noncompliant groups except for relapse. Power analyses were conducted to determine if our sample size was adequate. The major thrust of this study was to analyze the impact of the ADI on relapse; our study was adequately powered to determine a 9.1 percentile change in ADI, which is likely not clinically significant. Thus, we are confident that this study is adequately powered.

Graph demonstrating that of the 78 patients with idiopathic TEV having relapse, the relapse occurred by age 1 year in 24% and by age 4 years in 86%. The numbers represent the number of patients. These changes over time were statistically significant (P < 10-6). TEV, talipes equinovarus.
The results for both compliance and relapse were reviewed to ascertain single variables that might be variables predictive of relapse using logistic regression analysis. After review of the data in Table 1, the variables selected were type of idiopathic TEV (typical/complex), race (Black, White, Hispanic), performance of a tenotomy (yes/no), compliance with FABO (yes/no), number of casts to complete first correction (≤5, >5), ADI state groups (1, 2, 3), and length of follow-up (≤4 years, >4 years). Multivariate logistic regression analysis revealed that FABO compliance and length of follow-up were significant. The OR of relapse for FABO noncompliance was 17.9 (7.6, 42.4; P < 10−6) and the OR for follow-up >4 years was 4.97 (2.1, 11.70; P = .0003). The OR for complex TEV type fell out of the multivariate regression analysis with a P of .051. State ADI levels fell out of the model with at the first backwards step with P values of .23 (level 1) and .40 (level 2) relative to the most deprived group (level 3). This confirms the above-mentioned power analysis.
Discussion
The Ponseti method of treatment for ITEV results in excellent outcomes, although certain variables impact its success. These are FABO compliance and length of follow-up. In one systematic review, 46 the rate of relapse varied widely from 3.7% to 67.3% of patients. In another systematic review, the relapse rate varied from 1.9% to 45%. 12 Much of this variability was due to length of follow-up, but also the definition of relapse.12,46 In this study, we defined relapse as when the treating physician recommended further casting and/or surgery and was 46% at an average follow-up of 4.3 years. The rates of relapse in the literature are 22.7% 24 in Massachusetts, 27% in Alabama, 5 33% in Puerto Rico, 34 and 52% 38 and 68% 50 in Los Angeles. Early relapse in rural New Mexico was 25%. 2 Our 46% rate of relapse is on the higher end of these values, and likely reflects our very conservative definition of relapse: any time when the attending orthopaedic surgeon recommended to the family that further casting and/or surgery be performed, regardless of whether it actually happened. The need for a few repeat casts is much different than surgery, but nonetheless does represent relapse.
Our study confirms the findings of many others2,8,13,24,34,38,52 that the risk of relapse is associated with FABO noncompliance. Dobbs et al 8 noted that noncompliance had an OR of relapse of 183, much greater than the 17.9 in our study. Goldstein et al 13 noted that the risk of relapse was 7.9 times greater in the noncompliant group, lower than our 17.9 and certainly less than the 183 in that of Dobbs et al. 8 Shabtai et al 40 noted that the duration of FABO use had a significant effect on the outcome and rate of subsequent surgery. Children needing further surgery used the FABO for 28 months vs 33 months in those not needing additional surgery. Richards et al 36 noted that patients who reported <75% FABO wear had a 34% relapse rate compared to those reporting >75% FABO wear had a 9% relapse rate. A more recent study has noted that a full 12 hours of FABO wear after the first 3 months is not necessary to achieve good results at 2-year follow-up 35 ; however, the minimum amount of time needed for FABO wear to minimize relapse is still unknown. One study noted no correlation with FABO compliance and relapse. 20 Importantly, it should be noted that the determination of noncompliance varies by study, and has been determined mostly by parental self reports5,8,13,15,50 and less commonly by temperature sensor devices.35,39 In this study, we used both parental self-reporting as well as objective observation by the physician that the shoes had clearly not been worn after a 6-month time span and/or if the caregivers had been formally reported to the Child Protective Services of failure to comply with FABO bracing. The reported rates of noncompliance in several of these studies are 31%, 8 50%, 35 54%, 15 and 63%. 50 Our rate of noncompliance was 46%, clearly similar to other studies.
Our study also confirms others12,24,38,46,52 that have shown that with increasing time of follow-up, the percentage of relapse increases. Mahan et al 24 noted that of their 22% with relapse, 56% had their initial relapse before 2 years of age and the remaining 44% after 2 years of age. We had very similar results, with 48% occurring by age 2 years; 83% of all our relapses occurred by age 4 years (Figure 1). Siebert et al 43 noted that 35% of patients having a successful Ponseti outcome at the age of 2 years eventually underwent subsequent surgical intervention.
Pirani or Dimeglio7,11,29 severity scores were not recorded in this study. We used the number of casts needed for correction as a proxy for TEV severity; we noted that relapse was higher in those patients needing more casts to achieve initial correction (6.0 vs 5.3), although this became insignificant after a multivariate logistic regression analysis. The literature is discordant regarding TEV severity and risk of relapse. Some studies do not correlate TEV severity (either by number of casts needed for correction and/or Dimeglio/Pirani scores) with relapse, 20 whereas others do.5,13,38 Our study agrees with others where those with relapse had a higher number of casts 5 equating to more severe TEV. 38
We wished to explore various demographic variables that might be predictive of relapse after Ponseti method treatment of idiopathic TEV. In the final multivariate logistic regression analysis, only noncompliance with the FABO and length of follow-up of more than 4 years were predictive of relapse; sex, race, TEV laterality, and socioeconomic status were not predictive. Ramírez et al 34 noted that sex of the patient had no impact on relapse. Zionts et al 51 noted that there were no demographic variables predictive of FABO compliance that directly impacts the risk of relapse. Our study also found no demographic variables predictive of relapse.
Compliance and length of follow-up may be proxies for underlying socioeconomic factors (eg, family income, insurance status, race, and ability to meet follow-up appointments). For example, lower family income may simply reflect inability to attend follow-up appointments because of travel expenses and lost wages for the parents, in spite of their desire to be compliant. Similarly lower family income may put them into a Medicaid insurance stratum with barriers for them obtaining appropriate FABO products. Certain managed Medicaid insurances in our state would not allow our own orthotists to immediately place the FABO and instruct the family in proper use, but rather require outside companies. This is not ideal, as it was often several weeks before the family obtained the FABO, the training of the orthotists in proper patient instruction was unknown. Thus, it is necessary to use an overall comprehensive assessment of socioeconomic level/deprivation when reviewing the results of the Ponseti method for ITEV treatment. Many authors have noted different outcomes for various descriptors of socioeconomic level (eg, parental education level, income, insurance status).2,5,8,27,33 In this study, we used the ADI as a comprehensive measure of socioeconomic level. As such, it is an improved estimate of socioeconomic status and thus has been widely used in recent studies of health outcomes relating to socioeconomic differences.9,17,19,42 Our study is the first to use the ADI. In studies by Avilucea, Chong, and Dobbs,2,5,8 socioeconomic status was a predictor of recurrence, but that was not the case in our study and more compatible with the results of Ramírez et al. 34 Further investigation is likely needed from different centers to further explore these differences.
There are certain limitations to this study. As with any retrospective study incorporating demographic variables, not all data are entered for every patient. However, sex and laterality were known for all patients and race for 98.97%. As with all retrospective clinical studies, those lost to follow-up are problematic. Those lost to follow-up were compared to those not lost to follow-up by sex, race, TEV laterality, typical or complex TEV, tenotomy performed (yes/no), and ADI national percentile and ADI state groups. The only difference found was in the performance of a tenotomy. In those lost to follow-up 20% did not have a tenotomy performed, whereas in those with follow-up, 8% did not have a tenotomy performed. Interestingly, there was no difference in the ADI between the 2 groups. Our relapse of 46% is on the higher end and may reflect that we had nearly 50% lost to follow-up; perhaps those lost to follow-up were doing well and just did not return. Those children with less than 2 and 2 or more years of follow-up demonstrated no significant differences in the ADI (70 ± 20 vs 69 ± 21; P = .77).
The strengths of this study are several. First, the ADI was used to study socioeconomic status as it is a more global estimate of socioeconomic status than one single variable and it has not been used in any TEV outcome study to date. Second, this is a large series from the United States with 168 patients having an average follow-up of >4 years. Third, it was adequately powered to find any ADI differences between those with and without relapse if it actually existed. Finally, it reflects the applicability of the Ponseti method to a typical US children’s hospital setting where all faculty are fellowship trained in pediatric orthopaedics and well versed in the Ponseti method.
In conclusion, our study demonstrates several important points. Although other centers have found socioeconomic status to impact outcomes of clubfoot treatment, we did not. We therefore recommend that each center analyze its own population and determine how socioeconomic status impacts the outcome of TEV treatment. If found important, then consideration should be given to care programs that might mitigate these issues. There were no demographic variables in this study associated with relapse other than compliance with the FABO and length of follow-up. Therefore, at our center we have elected to simply reinforce, as strongly as possible to all parents/guardians, that FABO compliance and follow-up appears paramount to achieving the best results.
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the Indiana University Institutional Review Board (protocol no. 2003738139).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.