
Abstract
Background:
Young adults often tolerate the increased energy expenditure, coordination, and stance limb discomfort associated with walking aids for nonweightbearing ambulation. Adults aged ≥50 years may not have the same tolerance. Therefore, the objective of this study was to determine how walking aid selection affects stance limb plantar force, walking speed, perceived exertion, and device preference in adults aged ≥50 years.
Methods:
A prospective randomized crossover study was performed using healthy adults, aged ≥50 years, with no use of walking aids within 5 years. Participants walked 200 m in 4 randomized conditions: single nonweightbearing ambulation using crutches, a walker, a wheeled knee walker, and unaided walking. An in-shoe sensor measured stance limb plantar force, a stopwatch timed each walk, perceived exertion was reported using the BORG CR-10 scale, and device preference was identified.
Results:
Twenty-one participants (7 male; age: 56 ± 5 years; BMI: 26.6 ±1.9) showed stance limb plantar force was lowest when using a wheeled knee walker (P < .001). Walking speed was similar in unaided and wheeled knee walker conditions (1.41 and 1.31 m/s), but slower with crutches or a walker (42%-68%, P < .001). Perceived exertion was similar in unaided and wheeled knee walker conditions (1.6 and 2.8), but higher with crutches or a walker (5.7 and 6.1, P < .001). Most (20/21) participants preferred the wheeled knee walker.
Conclusions:
Using a wheeled knee walker for nonweightbearing ambulation reduced stance limb plantar force, maintained unaided walking speed and perceived exertion, and was preferred to crutches or a walker.
Level of Evidence:
Level II, comparative study.
Introduction
Walking aids are commonly prescribed to offload a lower extremity after operative repair or to aid diabetic foot ulcer healing, but little consideration has been given to their effect on loading of the stance foot. Limited reports of benefits from walking aid use to facilitate activity are available, but evidence suggests that nonweightbearing (NWB) ambulation to completely offload an injured lower limb using standard walking aids can cause axillary/hand pain or stance limb pain in 68% of users. 3,11,14 Major concerns are that walking aid selection may alter stance limb plantar force (SLPF), stepping frequency, and percentage of time weightbearing (% WB), and increase risk of injury. 7 Further, the increased physical demand of using standard walking aids, especially in older adults, negatively impacts user compliance and often results in patient discontinuance. 2 Therefore, standard walking aids may place patients in a dilemma; discontinuance could lead to delayed healing while maintaining use impacts activities of daily living performance.
The wheeled knee walker (WKW) is a walking aid designed to completely offload the foot and ankle, but limited research is available regarding WKW use in older adults. Anecdotal evidence suggests it may be more stable, easier to use, and reduce SLPF when compared to routinely prescribed walking aids. 7 In healthy young adult populations (24-38 years of age and 35 ± 9 years, respectively), WKW use resulted in approximately 40% less VO2 intake and 23% lower heat rate compared with a walker or crutches and was preferred over axillary crutches 88% of the time. 8,13 However, a current knowledge gap exists as to whether adults aged ≥50 years and older would experience similar benefits from WKW use.
The encumbrance of a walking aid for NWB ambulation could make multiple purposeful walks (∼800 m) prohibitive. 18 Patients scheduled for orthopedic foot and ankle surgery (mean age 32 years) reported significantly more fatigue and dyspnea when walking with standard axillary crutches than a hands-free single crutch. 11 Since fatigue is evident from walking aid use in younger adults, it would suggest different approaches are needed when targeting older adults for offloading a lower limb as current prescriptions often result in wheelchair confinement. 6,15
Therefore, the objective of this study was to measure SLPF, step frequency, % WB, rating of perceived exertion (RPE), self-selected walking speed (SSWS), and walking aid preference in a healthy population of adults aged ≥50 years. Walking aids used were axillary crutches, a walker, and a WKW with unaided walking acting as a control. Our first hypothesis was that SLPF, step frequency, % WB, and perceived exertion would be lowest among all walking aids when using a WKW. Our second hypothesis was that SSWS would be highest when using the WKW compared with the other walking aids. Our third hypothesis was that participants would select the WKW as their preferred walking aid.
Materials and Methods
This study was a prospective, randomized crossover design and was conducted at the University of Saskatchewan, School of Rehabilitation Science between 2018 and 2019.
Participants
Participants were recruited from the general Saskatoon area through flyers and word of mouth. Informed consent was obtained prior to data collection. Eligible participants attended a single testing session. Participant inclusion criteria were as follows: age ≥50 years, independent community dwellers in good overall health with no self-reported neuromuscular, musculoskeletal, or cardiovascular condition that would affect walking, self-reported upper body strength that would adequately support their body weight, and self-reported ability to walk 800 m. Individuals were excluded if they weighed more than 114 kg (weight capacity of the walker), had a painful upper or lower extremity, or a history of walking aid use within the last 5 years. All participants were instructed to wear comfortable clothing and shoes they would normally wear for activities of daily living. The University of Saskatchewan Ethics Committee approved the study (BIO32NER) and informed consent was obtained from all participants prior to study enrollment.
Procedures
Participants answered basic demographic questions about age, sex, and medical history. They were asked if they had ever used crutches or a walker and if they thought they were in good health. Height and weight were recorded using a physician beam scale with height rod. Participants were instructed on use of the Borg revised category-ratio scale and were asked to rate their exertion where 0 represented “nothing at all” and 10 represented “maximal” exertion. 1 The axillary crutches (Guardian, Adult Quick-Fit, Medline Industries, Inc, Pittsburgh, PA), walker (Duro-Med Folding Walker; Breg Inc, Carlsbad, CA) and WKW (Drive steerable aluminum knee walker; Medical Depot, Inc, Port Washington, NY) were fitted individually for each participant (Figure 1). All participants were provided a familiarization period with each device. Participants choose the foot they would use for weightbearing and propulsion. The contralateral limb maintained an NWB gait pattern with the foot completely unloaded; compliance was ensured by observation from the researcher during walking trials.

Assistive devices used within this study: (A) crutches (Adult Quick-Fit; Medline Industries Inc); (B) a walker (Duro-Med Folding Walker; Breg Inc); and (C) a wheeled knee walker (Drive steerable aluminum knee walker; Medical Depot Inc).
A wireless insole force sensor (LoadSol; Novel Inc) was fitted in the shoe of the stance foot to measure SLPF during each walking trial. This force sensor covered the entire plantar surface of the foot and was calibrated following the manufacturer’s protocol for each participant before data were recorded at 100 Hz via Bluetooth connection to an iOS device (ie, an iPad). Prior work has demonstrated that these force sensors provide a valid total ground reaction force, normal to the sensor’s surface, with excellent reliability when compared with force plates or instrumented treadmills during walking, running, or jumping activities. 4
Participants walked 200 m, on a straight 50 m indoor path free of any obstructions, for 4 trials total with a randomized presentation of walking aid. This distance was selected as purposeful walking trips are ∼800 m and we speculated that exceeding this total could be problematic for future comparison to a clinical population’s physical capacity. 18 Time to complete each walking trial, at a comfortable walking pace, was used to calculate SSWS. Immediately following each walking trial, participants stated their RPE and were given 2 minutes of rest before starting the next walking trial. Participants could stop walking at any point if they chose not to continue. If this occurred, the researcher noted elapsed time, distance walked, and asked for RPE. After completion of all trials, the participants were asked if needed, which device they would prefer to use.
Data Analysis
Data were processed using custom software in Matlab 9.6 (R2019a, The Mathworks Inc, Natick, MA). Calibrated plantar forces were exported from the LoadSol application and screened for missing values or abnormal trends. One participant’s plantar force data could not be used because of calibration issues with the insole force sensor but SSWS, RPE, and device preference were still included in our analyses. Thirty seconds of data, between 30 and 60 seconds, of each walking trial were selected for analysis to allow participants sufficient time to reach steady-state walking in each condition (Figure 2). 9,10 Individuals’ steps were identified within walking conditions using a 50 N threshold (∼7% of mean participant bodyweight) from plantar force timeseries data to avoid false positive step identification when the force sensor deflected within the shoe. 7 The frequency of steps occurring within our 30-second epoch was reported as step frequency for each walking aid. Identified step periods were used to define the percentage of our 30-second epoch that was spent weightbearing.
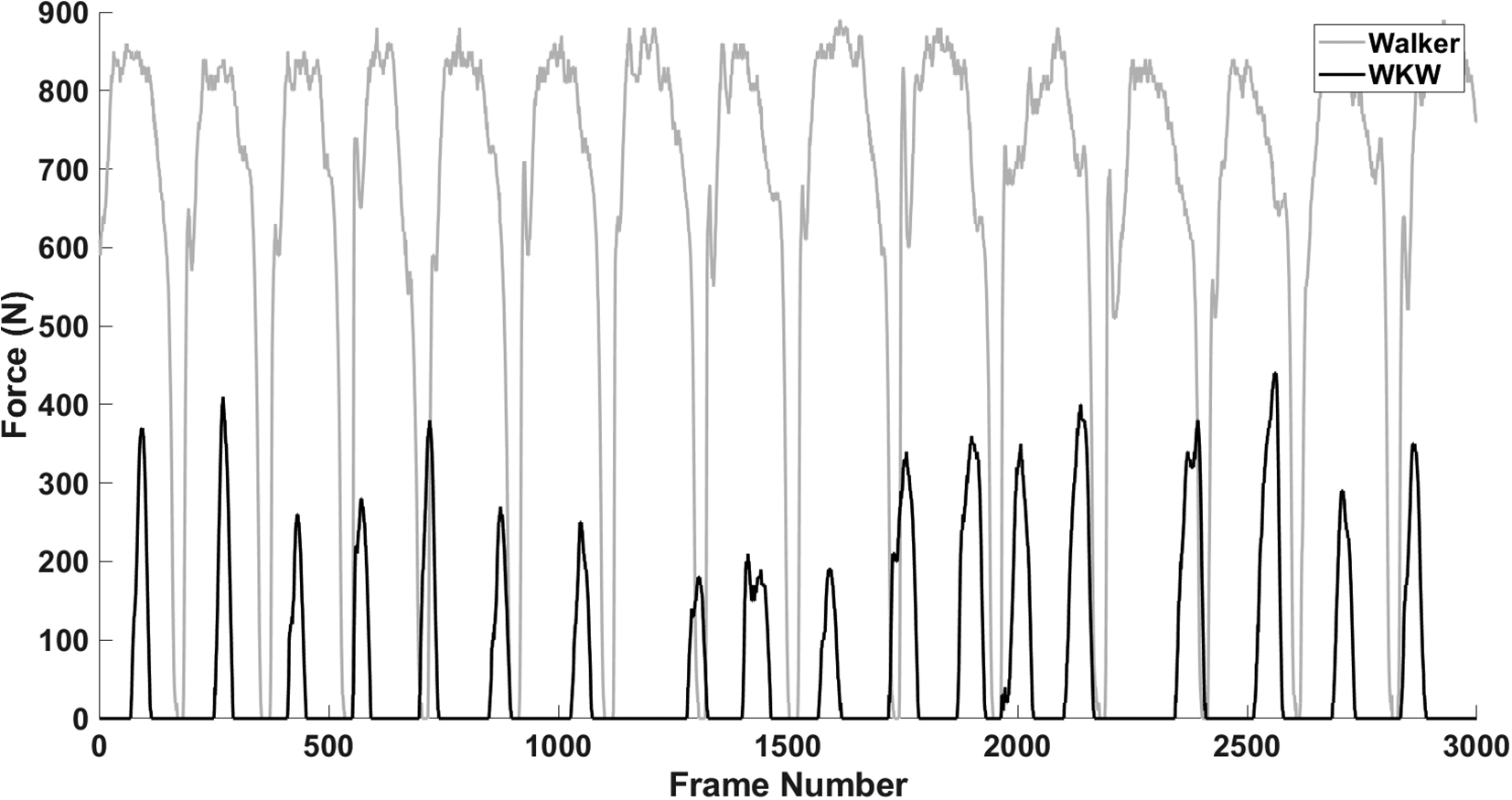
Stance limb plantar force data epoch (30-60 seconds of trial) used for outcome measure calculations in 2 walking conditions from a representative participant. Fifteen steps were taken with the walker (gray) and 18 steps were taken with the wheeled knee walker (WKW [black]).
Outcome Measures
Outcome measures for this study were average and peak SLPF, step frequency, %WB, SSWS, RPE, and walking aid preference.
Statistical Analysis
Statistical analyses were completed using Excel’s statistical toolbox (released 2016; Microsoft Corp, Redmond, WA). To determine differences in average and peak SLPF, step frequency, %WB, SSWS, and RPE across walking aids, 1-way repeated measures analysis of variance (fixed effect of walking aid condition) were performed. All statistical models used an a priori α = 0.05 with Bonferroni adjusted P values to correct for post hoc multiple comparisons. No statistical tests were performed for walking aid preference as we only report the frequency of selection.
Results
In total, 21 people participated in this study with demographic information reported in Table 1. In-text values are group mean differences with 1 standard deviation and the 95% confidence interval (CI) reported in brackets.
Demographics of Healthy Adult Participants.

Voluntary Walking Trial Cessation
Not all participants were able to complete the 200 m walking trial with each walking aid. Eleven and 15 participants were not able to complete the walking trial with crutches or a walker, respectively (Table 2). All participants completed the walking trial when unaided or using the WKW.
Distance Traveled by Participants When Using Respective Walking Aids in Meters.a

a No values for SD or range are reported for unaided walking or wheeled knee walker as all participants completed the 200 m walking trial.
Plantar Force and Time Weightbearing
A summary of average SLPF values is provided in Table 3. Average plantar force was at least 75% lower when participants used a WKW (84.6 N [61.8, 95% CI 57.5-278.4]) when compared to all other walking conditions (P < .001), but unaided walking also had at minimum 19% lower average plantar force than crutches or a walker (P < .001). Finally, crutches had an ∼10% lower average plantar force than when using a walker (P < .003). Peak plantar force was at least 46% lower when participants used the WKW (442.5 N [166.4, 95% CI 396-970.0]) than when compared to all other walking conditions (P < .001). No significant differences in peak plantar force were found among unaided walking, crutch, or walker use (Table 3).
Summary Plantar Force Values (n = 19) for Respective Walking Aids.a

Abbreviation: CI, confidence interval.
a Values that share superscripted letters (b-e) are not different at the P < .05 level. Bold values emphasize significantly different values.
Significant differences in % time weightbearing were found among all walking conditions with the most time weightbearing occurring during walker use 88.6% (4.5, 95% CI 86.6-90.6), followed by crutch use 79.0% (7.8, 95% CI 75.6-82.4), unaided walking 66.3% (3.9, 95% CI 64.5-68.1), and least time weightbearing with the WKW 48.3% (13.9, 95% CI 42.2-54.4) (P < .001) (Table 3).
Self-Selected Walking Speed and Step Frequency
A summary of SSWS and step frequency values is provided in Table 4. Self-selected walking speed did not differ between unaided walking 1.41 m/s (0.13, 95% CI 1.35-1.47) or when using the WKW 1.31 m/s (0.37, 95% CI 1.15-1.47). However, SSWS was slower with crutches 0.76 m/s (0.28, 95% CI 0.64-0.88) when compared to both unaided walking and the WKW or when using a walker 0.42 m/s (0.14, 95% CI 0.36-0.48) when compared to all other walking conditions (P < .001). Step frequency was at least 27% higher in unaided walking with 57.9 (10.8, 95% CI 53.0-62.8) steps/min when compared to all other walking conditions (P < .001). Step frequency did not differ among walking aids.
Summary Values for Self-Selected Walking Speed, Step Frequency of the Stance Limb, and Rating of Perceived Exertion (RPE).a

Abbreviations: SD, standard deviation; WKW, wheeled knee walker.
a Note that not all participant data were included for the reported variables due to force sensor issues. Values that share superscripted letters (b-d) are not different at the P < .05 level. Bold values emphasize significantly different values.
Rating of Perceived Exertion
A summary of RPE values is provided in Table 4. Rating of perceived exertion did not differ between unaided walking 1.6 (0.9, 95% CI 1.2-2.0) and the WKW 2.8 (1.3, 95% CI 2.1-3.3). However, RPE was at least 72% lower for unaided walking and 50% lower for WKW use when compared to walking with crutches or a walker (P < .001).
Device Preference
Participants overwhelmingly preferred the WKW over other walking aids as 95% or 20 of 21 participants stated they would use it as opposed to crutches or a walker.
Discussion
The objective of this study was to measure SLPF parameters, RPE, SSWS, and walking aid preference in a healthy adults aged ≥50 years. Participants performed 4 fully randomized walking trials, while unloading a single limb, when using walking aids of axillary crutches, a walker, and a WKW. Unaided walking acted as a control. This study was motivated by the high rate of noncompliance and rejection of walking aids among older adults, particularly when they have been prescribed for complete lower limb offloading after injury, operative intervention, or to promote wound healing. Overall, the WKW had significantly lower plantar force magnitudes when compared to the other walking aids or even unaided walking. Using a WKW also had minimal effects on SSWS or RPE when compared to unaided walking whereas crutches and a walker were detrimental to both speed and effort required. All but 1 participant stated they would choose the WKW over crutches or a walker if they were required for NWB ambulation.
In this study, we have reported unnormalized plantar forces, as opposed to a percentage of participant bodyweight (% BW) to provide a range of absolute values to the reader. Although participant mass would cause a relative increase in plantar force, tissues of the stance foot in a diseased state or at-risk population would likely be unconditioned from daily exposure. Similarly, the force sensor used in this study could be readily used by a clinician or physical therapist. The “raw” values reported in this study could be helpful in guiding walking aid selection as no calculations would be needed to assess plantar load exposure from the ‘typical’ ranges provided from our older adult population.
Our participants did not significantly change their SSWS when walking with the WKW as compared to unaided walking but were slower with crutches or a walker. Additionally, physical demands significantly increased while using a walker or crutches as indicated by the higher RPE reported by the participants. These physiological demands were evident from the inability of 50% (10 of 20) or 75% (15 of 20) of our participants to complete the 200-m walking trial with crutches or a walker. Given that all participants completed the 200-m walking trial with the WKW it shows promise that this device could increase independence and mobility if needed for NWB ambulation when compared to standard aids.
Our findings indicate that WKW use is preferred and that average and peak SLPF is significantly lower than when other walking aids are used for NWB ambulation. We believe these findings indicate that prescribing a WKW instead of other walking aids may increase compliance, diminish sedentary behavior and stance limb discomfort. Although our participants were healthy adults aged ≥50 years with no self-reported history of neuromuscular, musculoskeletal, or cardiopulmonary pathology, we believe our results can be generalized to healthy adults aged ≥50 years with lower extremity trauma. This is a distinct advantage of our work to a similar study on WKW use that was performed using 24 younger active military personnel that we assume would have a far higher physical capacity than our sample population. 8 Our cohort may not be generalized to older adults with pathology that may precipitate upper extremity weakness or chronic lower extremity injury such as diabetic foot ulceration, but this represents a potential area of further study.
The finding that average plantar force was highest during walker use was surprising as we anticipated higher magnitudes in the crutch condition due to a greater demand on the upper extremities. We assumed that relative instability of whole-body center of mass during swing phase when using crutches when compared to a walker would necessitate higher plantar forces. 17 Limiting our data analysis to within the first minute of walking (30-60 seconds) may have masked fatigue of the upper extremities that could affect control of body mass—and thus plantar forces—when walking for longer periods of time.
Further exploration of our data revealed that step frequency significantly differed among walking conditions, with fewer steps taken when walking with a walking aid than with unaided walking. This decreased step frequency, compounded by slower SSWS, with crutch and walker use significantly increased the percentage of time the stance foot was in contact with the ground. Interestingly, there was no difference in average SLPF when unaided walking (506.6 N [87.4, 95% CI 467.3-546.0]) was compared to walker use, which may be due to the high standard deviation associated with the average plantar force when using the walker.
Important limitations of the findings from this study include a small sample size, standardization of the walking path surface, and inability to measure force transfer to the walking aids. Although our sample of 21 participants is comparable to other studies investigating gait and foot pressures, more fulsome samples are required to have sufficiently powered studies for investigating potential gender effects in walking aid use. 12 Standardization of the walking path surface to a smooth indoor surface limits the application of our findings to other conditions such as carpet or outdoor environments as encountered in activities of daily living. Specifically, we did not assess the added difficultly walking aid selection could have on stair use. The WKW is heavier than the 2 other devices and would likely be more difficult to transfer if ascending or descending stairs independently. Of the walking aids tested, the only device that can safely be used on stairs for NWB ambulation are crutches. Even then, for safety, people who are NWB are encouraged to manage stair ascent or descent on their bottom. Finally, we did not have the capability to instrument our walking aids for investigating unloading mechanisms and force transfer to the upper extremity. Although limited work has been completed in the past on canes and walkers, this is a critical next step needed for WKW use in patient populations. 5,16
In conclusion, reduced SLPFs, maintenance of SSWS, and minimal increase to RPE may justify the use of the WKW over other walking aids when adults aged ≥50 years are prescribed a walking aid for NWB ambulation. This study demonstrates the impact of different walking aids on plantar force within a healthy adult population. Our findings are a critical first step in determining appropriate walking aid prescriptions for clinical populations. These data can be referenced as a baseline for future research focusing on how walking aids affect function and quality of life in people with pathologic conditions such as diabetic foot ulcers. Similarly, our results may help identify changes in elderly users who more heavily rely on these tools to maintain independence and mobility.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_2473011421998939 - Implications of Walking Aid Selection for Nonweightbearing Ambulation on Stance Limb Plantar Force, Walking Speed, Perceived Exertion, and Device Preference in Healthy Adults 50 Years of Age and Older
Supplemental Material, sj-pdf-1-fao-10.1177_2473011421998939 for Implications of Walking Aid Selection for Nonweightbearing Ambulation on Stance Limb Plantar Force, Walking Speed, Perceived Exertion, and Device Preference in Healthy Adults 50 Years of Age and Older by David C. Kingston, Sarah Ferwerda, Curtis Fontaine, Marhanda Keeping, Jeffrey Stewart, Rachel Ward, Jenelle Zapski, Kassondra Collins, Samuel K. Essien and Audrey R. Zucker-Levin in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval for this study was obtained from the University of Saskatchewan Ethics Committee (BIO32NER).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Audrey R. Zucker-Levin, MBA, PhD, was supported by the Kinsman Foundation Inc. The study sponsor had no influence on the design, collection, analysis and interpretation of data, or writing of this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.