
Abstract
Background:
Instability of the first-tarsometatarsal (TMT) joint has been proposed as a cause of hallux valgus. Although there is literature demonstrating how first-TMT arthrodesis affects hallux valgus, there is little published on how correction of hallux valgus affects the first-TMT joint alignment. The purpose of this study was to determine if correction of hallux valgus impacts the first-TMT alignment and congruency. Improvement in alignment would provide evidence that hallux valgus contributes to first-TMT instability. Our hypothesis was that correcting hallux valgus angle (HVA) would have no effect on the first-TMT alignment and congruency.
Methods:
Radiographs of patients who underwent first-MTP joint arthrodesis for hallux valgus were retrospectively reviewed. The HVA, 1-2 intermetatarsal angle (IMA), first metatarsal–medial cuneiform angle (1MCA), medial cuneiform–first metatarsal angle (MC1A), relative cuneiform slope (RCS), and distal medial cuneiform angle (DMCA) were measured and recorded for all patients preoperatively and postoperatively.
Results:
Of the 76 feet that met inclusion criteria, radiographic improvements were noted in HVA (23.6 degrees, P < .0001), 1-2 IMA (6.2 degrees, P < .0001), 1MCA (6.4 degrees, P < .0001), MC1A (6.5 degrees, P < .0001), and RCS (3.3 degrees, P = .001) comparing preoperative and postoperative radiographs. There was no difference noted with DMCA measurements (0.5 degrees, P = .53).
Conclusion:
Our findings indicate that the radiographic alignment and subluxation of the first-TMT joint will reduce with isolated treatment of the first-MTP joint. Evidence suggests that change in the HVA can affect radiographic alignment and subluxation of the first-TMT joint.
Level of Evidence:
Level IV, retrospective case series.
Keywords
Introduction
There has been much debate over the role of the first-tarsometatarsal (TMT) joint in hallux valgus. Many surgeons feel that hypermobility or instability of the first-TMT joint contributes to the pathology seen in hallux valgus (Figure 1). It has been shown that first-ray mobility increases with the severity of hallux valgus deformity. 8,9,13 This association has been used to justify first-TMT arthrodesis as an operative treatment option for hallux valgus.

(A) Preoperative radiograph demonstrating hallux valgus with an increased 1-2 IMA and first-TMT subluxation. (B) Postoperative radiograph demonstrating reduction of the 1-2 IMA and improved congruency of the first-TMT joint (red arrows).
Although an arthrodesis of the first-TMT joint can control the radiographic alignment of the first ray, few studies have addressed the radiographic alignment and congruency at the first-TMT joint after a first-metatarsophalangeal (MTP) joint arthrodesis. The purpose of this study was to determine if correction of the hallux valgus angle (HVA) impacts the first-TMT alignment and congruency. Improvement in these parameters would provide evidence that hallux valgus is associated with first-TMT instability. We hypothesized that correcting the HVA would have no effect on the first-TMT alignment and congruency.
Methods
Institutional review board approval was obtained. A retrospective review of 92 consecutive patients who underwent first-MTP arthrodesis between 2015 and 2019 for a diagnosis of hallux valgus from a single surgeon was performed. Inclusion criteria were patients aged >18 years, preoperative hallux valgus angle greater than 15 degrees, and those who underwent a first-MTP arthrodesis. Excluded patients were those with incomplete radiographs and those who underwent additional operative alignment procedures at the time of the arthrodesis. Patient demographics including sex, age at time of surgery, laterality, and BMI were recorded.
Weightbearing radiographs were reviewed preoperatively and postoperatively. Radiographic measurements obtained included hallux valgus angle, 1-2 intermetatarsal angle (IMA), first metatarsal–medial cuneiform angle (1MCA), medial cuneiform–first metatarsal angle (MC1A), relative cuneiform slope (RCS), and distal medial cuneiform angle (DMCA) as previously described 10,11,14 (Figure 2). All radiographic measurements were obtained using our institution’s PACS software and were performed by the first author. Verification was performed by the senior author to ensure accuracy and consistency of measurements.

Measurements of hallux valgus are illustrated and include (A) hallux valgus angle (HVA), (B) intermetatarsal angle (IMA), (C) first metatarsal–cuneiform angle (1MCA), (D) medial cuneiform–first metatarsal angle (MC1A), (E) relative cuneiform slope (RCS), and (F) distal medial cuneiform angle (DMCA).
Paired sample t test was used to compare means of all measurements in the preoperative and postoperative groups.
Results
A total of 76 patients met the inclusion criteria. There were 6 patients who underwent bilateral, staged first-MTP arthrodeses. The mean age was 61. A total 85.5% (n=65) were female.
The mean preoperative HVA and 1-2 IMA was 36.1 degrees (SD = 10.0) and 14.4 degrees (SD = 4.1), respectively. There was mean improvement of 23.6 degrees (P < .0001) in the HVA and 6.2 degrees (P < .0001) in the 1-2 IMA.
Significant preoperative and postoperative differences were noted within 1MCA (preoperative mean, 98.9 degrees, SD 8.7; postoperative mean, 92.6 degrees, SD 6.2; P < .0001), MC1A (preoperative mean, 25.0 degrees, SD 5.9; postoperative mean, 18.6 degrees, SD 4.4; P < .0001), and RCS (preoperative mean, 33.0 degrees, SD = 9.0; postoperative mean, 29.6 degrees, SD = 7.5; P = .002). See Table 1.
Recorded Mean Values of Radiographic Measurements Preoperatively, Postoperatively and Mean Difference.
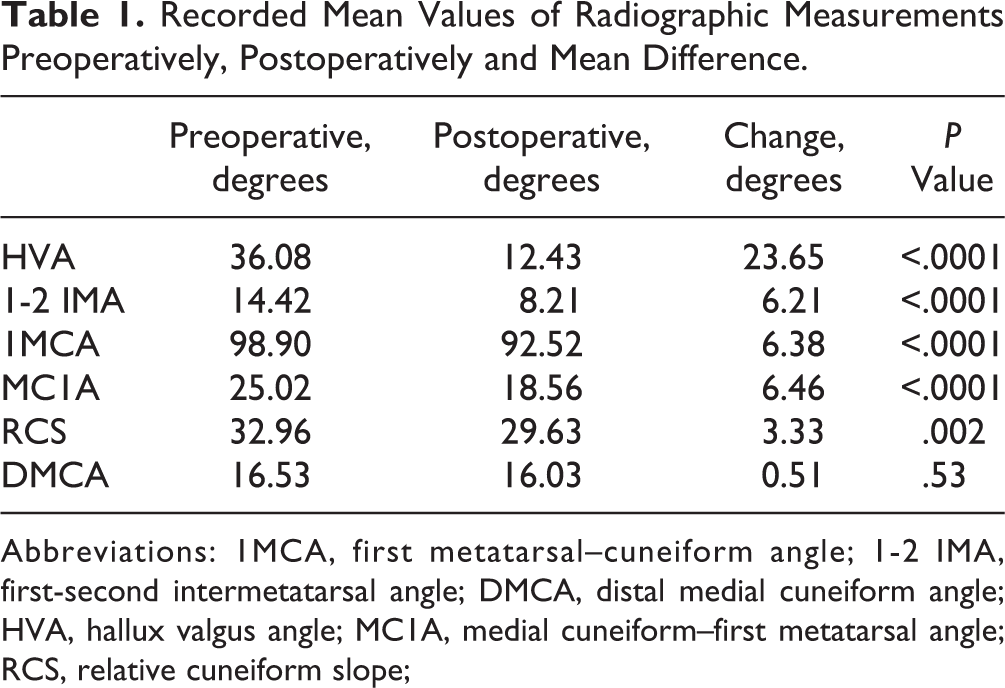
Abbreviations: 1MCA, first metatarsal–cuneiform angle; 1-2 IMA, first-second intermetatarsal angle; DMCA, distal medial cuneiform angle; HVA, hallux valgus angle; MC1A, medial cuneiform–first metatarsal angle; RCS, relative cuneiform slope;
There was no statistical difference between preoperative and postoperative DMCA measurements (preoperative mean, 16.5 degrees, SD 7.8; postoperative mean, 16.03 degrees, SD 6.4; P = .53).
Discussion
The current study demonstrates an improvement in the first-ray radiographic measures after an isolated first-MTP arthrodesis including improvement of the alignment and reduction of the first-TMT joint. This suggests that a change in the first-MTP joint can correct deformity at the first-TMT joint in patients with hallux valgus. Two of our measurements, first metatarsal–cuneiform angle and medial cuneiform–first metatarsal angle, included measurements using landmarks isolated to the bony structures of the first-TMT joint. Thus, we feel these are the best measures demonstrating improved alignment at that joint.
Although some surgeons choose to perform a first-TMT arthrodesis in the setting of first-TMT malalignment and hallux valgus, others choose to approach the deformity with first-TMT joint-sparing procedures. 3,4,6,7 In an RTC involving 101 patients, Faber et al was unable to show a difference in both clinical and radiographic outcomes between those who underwent a first-TMT arthrodesis with a distal soft tissue procedure and those who underwent a proximal first-metatarsal osteotomy alone. 7 In cadaveric and clinical studies, Coughlin et al has been able to demonstrate that mobility of the first-TMT joint decreases with distal soft tissue procedures in combination with a proximal first-metatarsal osteotomy. 3,4 These procedures spared the first-TMT joint.
It has been shown that the 1-2 IMA decreases with a first-MTP fusion. 2 Furthermore, it has been demonstrated that obliquity of the first-TMT joint can be corrected following a first-MTP fusion. 5 Our results support these findings. King et al was able to show that the first metatarsal–medial cuneiform angle measured on a lateral weightbearing radiograph was different in patients with hallux valgus vs controls. 12 There have been other published radiographic assessments of the alignment and congruency of first-TMT, joint including 1MCA, MC1A, RCS, and DMCA. Many have these demonstrated differences when comparing those with hallux valgus to controls. 10,11,14
When looking at the radiographic measurement of first metatarsal–cuneiform angle (1MCA) in patients with juvenile hallux valgus, Vyas et al determined there was a statistically significant difference between patients with JHV and those without. 14 Kaiser et al 11 was able to expand on this and demonstrated a correlation in 1MCA to the severity of HVA in patients with JHV. Our mean preoperative 1MCA was 98.9 degrees, reducing to 92.5 degrees postoperatively. This was slightly larger than the Vyas et al and Kaiser et al studies where their cohorts with JHV had mean 1MCA measurements of 90.1 and 94.1 degrees compared with 86.6 and 90 degrees in controls, respectively. In these studies, they only included patients with JHA and did not measure radiographs following operative correction. It is unclear if the known anatomic difference in patients with JHV may account for the differences noted.
Hatch et al analyzed various radiographic measurements in a study with 50 feet. They determined that the 1MCA for bunion deformities (mean 23.5 degrees) was significantly greater than that for the normal feet (mean 18.5 degrees) (P < .001). 10 Our mean preoperative 1MCA was 25.0 degrees and reduced to a postoperative level of 18.6 degrees, similar to the measurements among normal feet in the Hatch study.
The current study demonstrates that the DMCA was not significantly different between the preoperative and postoperative measurements. This is intuitive because the measurement is referenced along 2 medial cuneiform landmarks, and thus with an isolated procedure distally, we would not expect a change in the anatomic morphology of the bone. Similar to our results, when comparing DMCA in those with bunions to those without, Hatch et al was unable to demonstrate a significant difference. 10 Dayton et al measured the obliquity of the first-TMT joint before and after a first-MTP joint arthrodesis. For their measurement, they used the angle formed by a line perpendicular to the lateral border of the medial cuneiform and a line connecting the medial and lateral points of distal articular surface of the medial cuneiform. In their study of 86 patients, they were able to demonstrate a positive correlation between change in IMA and change in obliquity of the first TMT joint. However, they were unable to show a statistically significant correlation within the preoperative-only group and only within the subgroup of “severe” hallux valgus group postoperatively. Dayton et al hypothesized that positional changes occur postoperatively, and radiographically appear different with an improved alignment of the first ray and hallux valgus correction. 5 We used a similar angular measurement but were unable to demonstrate any difference before and after a first-MTP arthrodesis.
This study has several limitations. First, changes in x-ray beam orientation can create significant changes within the radiographic measurements of certain x-ray parameters. 1,10 Radiographs were obtained using standard protocols within the same facility, so variation is likely minimal. However, it is unknown how this affects the current data given that hallux valgus can affect radiographic parameters. Second, this is a single surgeon, single institution, and retrospective study, thus the results may not be generalizable. Lastly, our study only looked at patients with hallux valgus treated with a first-MTP arthrodesis. We did not evaluate patients who underwent joint-sparing hallux valgus treatments. However, as our study demonstrated reduction in HVA and 1-2 IMA through a first-MTP arthrodesis procedure, we would expect similar results with other joint-sparing procedures that also reduce the HVA and 1-2 IMA.
Conclusion
Our findings suggest that the radiographic alignment and subluxation of the first-TMT joint will reduce with isolated treatment of the first-MTP joint. This provides evidence that change in the HVA can cause changes in the first-TMT joint.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211008514 - First-Tarsometatarsal Joint Alignment After First-Metatarsophalangeal Joint Arthrodesis for Hallux Valgus
Supplemental Material, sj-pdf-1-fao-10.1177_24730114211008514 for First-Tarsometatarsal Joint Alignment After First-Metatarsophalangeal Joint Arthrodesis for Hallux Valgus by Christopher Traynor and James Jastifer in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Western Michigan University Homer Stryker M.D. School of Medicine Institutional Review Board (Waiver of HIPPA Authorization: WMed-2019-0511).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.