
Abstract
Background:
This is a retrospective review of patients who have had a Lapidus procedure for hallux valgus deformity correction, performed by a single surgeon.
Methods:
The clinical records, operation notes and available weightbearing preoperative and postoperative radiographs of all patients who had a Lapidus procedure between February 2008 and July 2018 for hallux valgus deformity were reviewed. The preoperative and postoperative hallux valgus angle (HVA), intermetatarsal angle (IMA), and talometatarsal angle (TMT) on anteroposterior (AP) and lateral radiographs were recorded. The postoperative Foot and Ankle Ability Measure (FAAM) scores were obtained from phone interviews.
Results:
Two hundred thirteen Lapidus procedures were identified between February 2008 and July 2018 and included in the final analysis. The average preoperative and postoperative HVA was 36.3 and 18 degrees, respectively, with an average improvement of 18.3 degrees. The average TMT angles showed a preoperative and postoperative difference of 1.1 degrees on the AP radiograph and 2.4 degrees on the lateral. The average preoperative and postoperative IMA angles were 16.5 and 7.4 degrees, respectively, with an improvement of 9.1 degrees. There were 9 cases (4.2%) of nonunion confirmed on radiography, of which 3 cases (1.4%) had revision fixation with bone graft and went on to radiologic union. Final FAAM scores were available for 151 patients (70.9%). From this group, 74.8% (113/151) scored higher than 90%, 16.6% (25/151) scored between 70% and 90%, and 8.6% scored between 50% and 70%. The patient satisfaction rate was 92.9% overall.
Conclusion:
This single-surgeon retrospective review of a relatively large number of Lapidus procedures reports acceptable radiologic correction and patient satisfaction.
Level of Evidence:
Level IV, Large case series.
Introduction
Hallux valgus is a complex foot deformity for which there have been many procedures described in the literature for surgical correction.8,15,16 A major advantage of the Lapidus procedure is its ability to stabilize the first ray and restore the weightbearing tripod of the foot, thus protecting the lesser rays from overload symptoms and associated progressive toe deformities. The most commonly described indication for a Lapidus procedure is hypermobility or instability of the first ray with moderate to severe hallux valgus deformity.2,4,9,11 The operation involves the release of the adductor hallucis tendon and lateral capsule distally. 15 The medial eminence is partially excised, followed by fusion of the base of the first metatarsal to the medial cuneiform with correction of the abnormal intermetatarsal angle (IMA).2,20 Modern fusion rates are considered to be much higher now with the advent of stable internal fixation techniques, including plate and/or screw fixation at the fusion site. Nonunion rates were previously up to 12%, but are now 3% to 4%.9,14,20 This is a retrospective review of patients treated with a Lapidus procedure for the correction of hallux valgus deformity performed by a single surgeon. The primary aims of the review were to examine the medium- to long-term results, including radiologic correction and patient satisfaction.
Methods
This is a retrospective analysis of all Lapidus procedures performed by a single surgeon between February 2008 and July 2018. Patients with bilateral operations were performed in a staged fashion and were recorded as a separate case. The clinical records, operation notes, and available radiographs of all patients who had a Lapidus procedure for hallux valgus were reviewed. Weightbearing foot radiographs were performed preoperatively, then postoperatively at 6 weeks, 3 months, 6 months, and 12 months at the time of a clinical review. Figure 1 and 2 demonstrate an example from the case series preoperative radiographs and then postoperative radiographs respectively. Figure 3 is a clinical picture demostrating hallux valgus deformity prior to correction in clinic. The preoperative and postoperative hallux valgus angle (HVA), IMA, and talometatarsal (TMT) angles on the most recent weightbearing radiographs were recorded. This was done by a single independent investigator. The IMA and HVA have been validated in assessing hallux valgus deformity and surgical correction. 7 The first TMT angles were included as an indication of foot alignment and arch height for those with hypermobility of the first ray. 13 The postoperative foot and ankle ability measure (FAAM) scores were gathered from phone interviews and were recorded as a percentage. Overall patient satisfaction was recorded from the clinical records.

Preoperative anteroposterior and lateral radiographs show severe hallux valgus deformity.

Clinical photograph showing bilateral feet with hallux valgus deformity on left foot.

Postoperative anteroposterior and lateral radiographs after Lapidus procedure.
Operative Technique
Patients were positioned supine with a tourniquet and a wedge under the ipsilateral hip to control limb alignment. Skin preparation was with chlorhexidine and alcohol solution and the limb draped using disposable drapes. The distal soft tissue procedure was completed first. The first web space was entered using the technique described by Panchbhavi et al and the lateral capsule and adductor tendon released, as illustrated in Figure 4. 15

Distal incision at the first web space, to facilitate the lateral capsule and adductor tendon releases.
A separate medial incision over the first MTP joint was then made to expose the joint. The medial collateral ligament and medial capsule are stripped off the metatarsal head. The medial eminence of the first metatarsal is partially removed with a small saw as demonstrated in Figure 5.

Surgical photograph showing the distal medial incision over the first MTP joint. The medial collateral ligament and the medial capsule were stripped off the metatarsal head. The medial eminence of the first metatarsal was partially removed with a small saw.
Correctability of the first metatarsal is assessed, with the aim of 30 degrees of varus at the metatarsophalangeal joint and if necessary further soft tissue release performed on both sides of the joint. Another more proximal medial incision centered over the tarsometatarsal joint is made to expose the joint medially and dorsally, and a distractor is used to improve access and articular cartilage debridement, this seen in Figure 6.

Surgical photograph demonstrating more proximal medial incision, centered over the tarsometatarsal joint and distractor inserted to open up the joint.
To correct metatarsus varus and dorsiflexion deformities, a small saw is used to excise bone from the plantar lateral aspect of the joint. The debrided subchondral bone surfaces were then perforated with a 4-mm burr to expose underlying bone to the fusion site and the bone dust left in situ as bone graft. 22 The first ray was then positioned and aligned anatomically and the joint was held in the corrected position with a temporary Kirschner (K)-wire. The definitive fixation was undertaken with 2 crossed 4-mm cortical screws placed from the dorsal surface of the first metatarsal and medial cuneiform, respectively; the screws were not lagged. In most cases, an intermetatarsal 4-mm screw was used to control height, varus/valgus alignment, and rotation of the first metatarsal to allow 3-dimensional correction of the deformity.
If hindfoot correction was necessary to correct axial alignment, a calcaneal osteotomy was performed before the Lapidus procedure aiming to work proximal to distal. Similarly, if a gastrocnemius lengthening was deemed to be necessary, a Baumann technique 1 was used before the Lapidus procedure. If additional forefoot procedures were required such as a second metatarsal Weil osteotomy, hammer toe correction, or tenotomies for toe deformities, these were generally undertaken following the Lapidus correction.
Wound closure was routinely performed using 2.0 Vicryl (Ethicon, Somerville, NJ) interrupted subcutaneous sutures and 4.0 Monocryl (Ethicon) with buried knots. Patients had light dressings and application of a well-padded below-knee or shoe cast, depending on additional hindfoot procedures.
Patients were casted for 6 weeks and made partial weightbearing through the heel on crutches or on a knee scooter after an initial period of strict elevation.
At 2 weeks, the cast and dressing are changed. Patients are allowed to begin full weightbearing following radiographs at 6 weeks after confirming healing, while avoiding prolonged walks or heavy physical activity. At the 12-week mark, bony union is assessed on radiographs and unrestricted activities allowed if there are no concerns.
Results
Two hundred thirty-five Lapidus procedures were identified between February 2008 and July 2018. Twenty-two cases were excluded because of unavailable preoperative and postoperative radiographs, bringing the total number of included procedures to 213 in 185 patients. There were 54 bilateral procedures, all staged and performed at least 3 months apart. The mean age of patients at the time of surgery was 57.86 years (range, 19-87) and 94% of patients (200/213) were female (male-female ratio of 1:15). The average follow-up was 7.2 years or 86.4 months (range, 6-148 months), this all outlined in Table 1. Additional simultaneous surgeries were performed on 54.9% of cases (117/213) because of varying pathologies associated with hallux valgus deformity, including calcaneal osteotomy, flexor digitorum longus transfer and spring ligament reconstructions for progressive collapsing flat foot deformity, proximal interphalangeal joint fusion for clawed toes, tendon transfers, second metatarsal Weil osteotomy, and gastrocnemius slide procedures.
Patient Demographics (N = 213).

The indication for surgery was symptomatic hallux valgus deformity in 196 cases (92%), recurrent hallux valgus in 17 cases (7.9%), and nonunion of a previous Lapidus procedure in 1 case. The 17 revision cases included 4 previous Lapidus procedures, 2 Weil osteotomies, 3 scarf and Akin procedures, 1 minimally invasive chevron and Akin procedure (MICA), 2 McBride procedures, 2 chevron osteotomies, and 1 Mitchell osteotomy. Two patients had first metatarsophalangeal joint fusion that required an additional Lapidus procedure for ongoing first-ray instability. Four cases (1.9%) required revision of their Lapidus procedure—3 for nonunion and 1 for recurrent deformity.
Postoperative FAAM scores were obtained in 70.9% (151 cases) of the cohort. FAAM scores were not obtained in 26.3% cases (56) whom we were unable to contact, 1.8% (4 cases) declined to participate, there was 1 death, and 1 patient had cognitive impairment. From the available FAAM scores, 74.8% (113/213 cases) scored >90 points of a maximum of 100, and 16.6% (25/213 cases) scored between 70 and 90 points, 8.6% (13/213 cases) had scores below 70. From the total cohort, 93% (198/213) of patients were overall satisfied with their operation. This is summarised in Table 2 below.
Patient-Reported Outcomes: Postoperative FAAM Scores and Patient Satisfaction. a
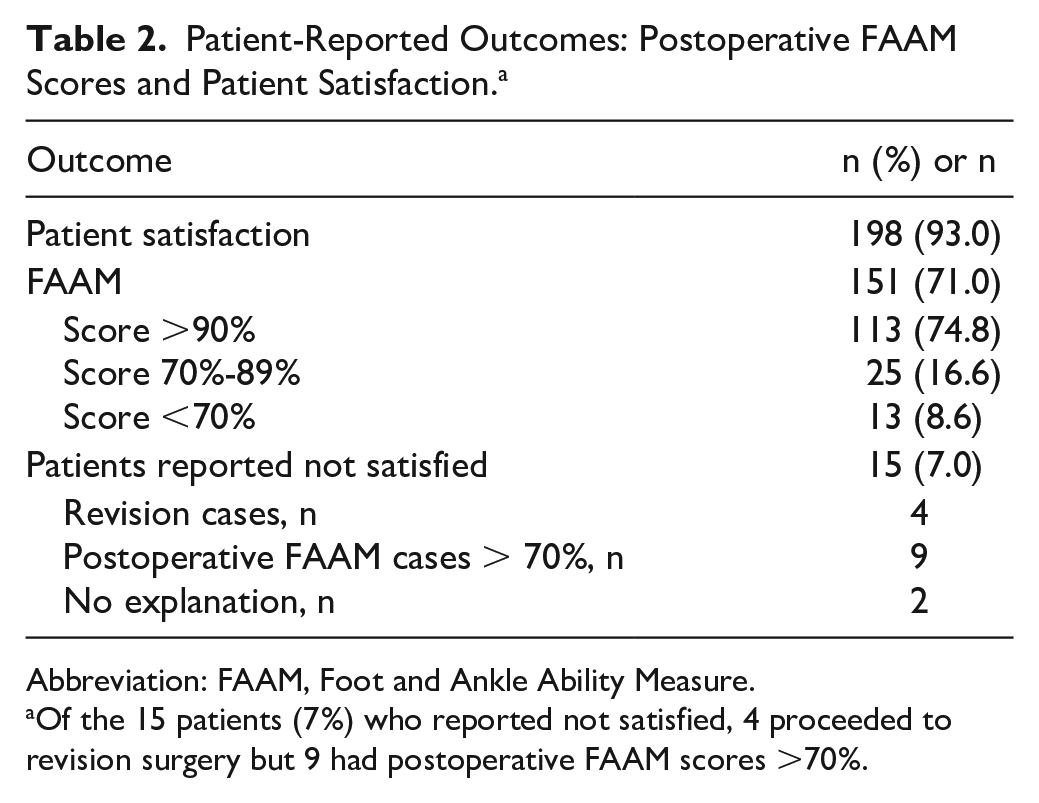
Abbreviation: FAAM, Foot and Ankle Ability Measure.
Of the 15 patients (7%) who reported not satisfied, 4 proceeded to revision surgery but 9 had postoperative FAAM scores >70%.
The average preoperative HVA was 36.2 degrees, correcting to an average postoperative HVA of 18.1 degrees, giving an average correction of the HVA of 18.1 degrees. The average preoperative IMA was 16.5 degrees and postoperative IMA 7.5 degrees, with an average improvement of 9 degrees. The average talus first metatarsal AP angle preoperatively was 6.5 degrees and corrected to an average of 5.7 degrees postoperatively, with a difference of 1.1 degrees. And the average lateral talus first metatarsal angle measured 7.7 degrees preoperatively, correcting to 5.1 degrees postoperatively and giving a difference of 2.4 degrees. This is summarised in Table 3 below. This correction of the lateral talometatarsal angle was thought to be in keeping with the intention of plantarflexing the first ray slightly to correct the first ray elevation seen in hallux valgus deformity, thus restoring the weightbearing tripod.
Summary of Average Radiologic Correction. a

Values are in degrees.
Complications
There were 9 cases (4.2%) of radiologic nonunion, of which 3 had revision fixation with bone graft and progressed to radiologic union. There was 1 revision for recurrent deformity from malunion. A total of 13 cases (6.10%) required removal of metalware for pain and discomfort medially, including 4 for excessive plantarflexion of the first ray and another due to an area of ulcerated skin over a prominent screw. There were no wound infections or significant wound breakdowns. There were 4 symptomatic venous thromboembolic events despite routine foot pumps on the contralateral side, early mobilization with either enoxaparin or aspirin chemical prophylaxis for venous thromboembolic event. All cases had confirmed superficial venous thrombosis on ultrasonography, including 1 soleal vein and 3 gastrocnemius vein thrombosis. One patient had a history of provoked deep vein thrombosis and had a preoperative anticoagulation plan with warfarin postoperatively. The other 3 cases had no additional risk factors. All patients were touch weightbearing in a cast for 6 weeks and also had additional gastrocnemius slide procedures. These complications are summarised in Table 4 below.
Summary of Postoperative Complications and Breakdown of Revision Surgeries.

Abbreviations: SSI, surgical site infection; VTE, venous thromboembolic event.
Discussion
Hallux valgus is a common foot condition with variable severity.4,16 There are more than 100 procedures described in the literature to address this deformity surgically,4,8,9 including distal and proximal metatarsal osteotomies, soft tissue releases, and fusions with indications depending on the clinical and radiological severity.8,16,18 The indication for a Lapidus procedure is moderate to severe hallux valgus with arthritis or hypermobility of the first tarsometatarsal joint,2,14,20 characterized by an HVA of 30 to 40 degrees and an IMA of more than 14 degrees.3,4,9,10,20 In this series, all patients had conventional indications for a Lapidus procedure; 92% (196/213) were primary cases and 8% (17/213) were revision cases for recurrent deformity. Although recurrent hallux valgus deformity and prior correctional surgery is a risk factor for nonunion, 20 Coetzee et al 4 in a prospective study suggested that a Lapidus procedure is adequate for treating refractory and recurrent hallux valgus deformity, despite previous surgical correction.
The main reservations about performing a Lapidus procedure include the steep learning curve, risk of shortening the first ray (>0.5 cm), dorsal positioning of the first metatarsal leading to transfer metatarsalgia, and risk of nonunion.4,11,17,20,21 There have been many modifications to the original Lapidus procedure in order to address some of these problems.2,6,9,11,19
Correlation of PROM to Radiologic Correction
Table 5 compares radiologic correction of deformity and patient satisfaction between this study cohort and other case series published in the literature.2,11,12,20 In comparison, our series was larger with more advanced deformity preoperatively and similar rates of nonunion and patient satisfaction.
Comparison of Results With Other Study Cohorts.

Abbreviations: HVA, hallux valgus angle; IMA, intermetatarsal angle; N/R, not reported.
This cohort also included primary TMTJ fusions, for flat foot reconstructions.
When correlated to radiologic correction, those with a postoperative FAAM score of less than 70 had an average radiologic correction of their HVA from 36 (24.7-52.5) to 19.8 degrees, with a difference of 16.3 degrees. The average preoperative IMA was 15.3 (12.4-19.2) degrees, correcting to 8.2 degrees, with a difference of 7.1 degrees. These results are within the average radiologic correction of the whole cohort. There were no identifiable patient characteristics or details in surgical technique to account for the lower postoperative FAAM scores in these patients.
Cases Requiring Revision
All 4 cases that required revision for nonunion or recurrent deformity reported being dissatisfied with the initial Lapidus procedure. However, 3 cases that required revision had postoperative FAAM scores of >90% following their revision surgery. We were unable to contact the fourth case who had a revision, so we could not obtain the postoperative FAAM score.
The nonunion rate in this study was 4.2% (9/213 cases) and is in keeping with nonunion rates in the current literature of 3.3% and 12%.4,8,14,20 Given the majority of radiologic nonunion cases become asymptomatic, it is the surgeon’s preference to allow adequate time and opportunity progress to a delayed union, provided they are comfortable. Two of the patients were revised 3 years after their index procedures because of worsening pain. One of these cases had a severe preoperative deformity with an HVA of 45.7 degrees and an IMA of 18.9 degrees. The third nonunion was revised earlier for unresolved pain and recurrent deformity, using further fixation with screws and bone graft from the proximal tibia. The final revision case was for recurrent deformity, with a preoperative HVA of 41.6 and IMA of 12.5, corrected to 31.1 and 9.6 degrees, respectively, at the index Lapidus operation. This patient had a previous osteotomy 10 years prior but had recurrent symptoms as well as clawed toes. She had a revision first tarsometatarsal joint fusion and second metatarsophalangeal joint Weil osteotomy and third MTP release 2 years following the index Lapidus procedure.
Analysis of Operative Technique
It is difficult to identify any part of the operative technique or specific patient factors that may contribute to recurrent deformity or nonunion following a Lapidus procedure. The conventional modern Lapidus procedure with internal fixation using crossed screws at the first tarsometatarsal joint was described by Sangeorzan et al 17 and is the technique employed by the primary surgeon. An intermetatarsal screw was added to prevent diastasis of the first and second metatarsals. Optimal joint preparation is advised with thorough debridement of the joint to expose subchondral bone.4,14,20 Shortening is kept to a minimum by removing only the articular cartilage layer and then fenestrating the subchondral bone with a burr rather than making substantial bone cuts with a saw. 22
To further increase chances of union, a burr is used to penetrate the subchondral bone, with the burrings left in situ as osteogenic bone dust, a technique described by Wheeler et al 22 and demonstrated in Figure 7. Other described techniques include fenestrating the fusion site with a drill or K-wire or using a saw or curettage to increase bony contact area.4,14,20

Joint preparation at fusion site using technique described by Wheeler et al, 22 a burr is used to penetrate subchondral bone and then the burrings left in situ as osteogenic bone dust.
With many plate and screw fixation construct combinations available,4,5,12 suboptimal screw placement or unstable fixation may also contribute to nonunion. It remains unclear in the literature if fixation with a more rigid construct leads to better outcomes and lower nonunion rates. The larger 4.0-mm cortical screws rather than the standard 3.5-mm screws were used given they are stronger and less likely to undergo fatigue failure.
Langan et al 12 suggested using a medial locking plate with the addition of a crossed intermediate cuneiform screw from the base of the first metatarsal. This increases the stiffness and stability of the construct to maintain correction and reduce the rate of nonunion. Both the reported nonunion and recurrence rate in their series of 62 cases was 3.3%. 12 Cohen et al 5 in a cadaveric study demonstrated superior results with the crossed-screw technique owing to better compression when compared with a locking plate. They suggested that good compression with screws was more advantageous than a rigid locking plate allowing better stability at the fusion site on weightbearing. 5 The aim in our series was not compression at the fusion site but for accurate coaptation of the bone surfaces. Given our adequate union rate, this may suggest that routine compression at the fusion site is not necessary.
Klos et al, 10 in a cadaveric study, demonstrated better strength with the medial locking plate following cyclical loading, compared to the traditional cross screw technique. They suggested that medial plating is more accessible and, with fixation of the tension side of the fusion, will be able to withstand bending forces across the fusion site, thus improving chances of union. Scranton et al 18 compared medial locking plates and a compression screw in another cadaveric biomechanical study and had similar findings. However, medial plates are bulky and can necessitate further surgery to remove the plate if irritating the skin or medial structures such as the tibialis anterior tendon.
Smoking is a well-established risk factor for nonunion of other joint fusions. Coetzee et al suggested the use of supplemental autogenous bone graft in smokers. 3 Smoking status was not available in this case series; however, in general the operation is not offered to known smokers because of the high risk of inferior results.
Complications
There were no deep infections in this case series and may be due to meticulous soft tissue handling, including using sharp dissection while avoiding underlying skin edges. Operative factors allowing optimum primary wound healing include reduced operating time and screw fixation, which is less bulky than plate fixation leading to less tension on the soft tissues. 7 The venous thromboembolic event rate was 1.8% and minimized with foot pumps, early mobilization, and low-dose enoxaparin or aspirin in high-risk cases. There were no recognized pulmonary emboli.
Limitations
Limitations include the generalizability of the findings to other populations of patients and surgeons and the inherent biases due to the retrospective nature of the study, leading to incomplete data. Some patients had moved location, which meant that patient contact details were not always up to date, limiting our ability to obtain a complete series of postoperative FAAM scores. We were unable to collect and compare preoperative FAAM scores. Much of the existing literature is retrospective, with small numbers. Although this study has large numbers, conducting a prospective study comparing another operative intervention with similar demographics and baseline characteristics would better evaluate the outcomes of the Lapidus procedure.
Conclusion
This is a relatively large cohort of Lapidus procedures by a single surgeon reported with medium to long-term follow-up. Preoperative and postoperative radiographs and postoperative FAAM functional scores suggest a high percentage of successful outcomes both in terms of sustained radiographic correction and patient satisfaction. Patients who reported low satisfaction scores and those with relatively low postoperative FAAM scores had hallux valgus and intermetatarsal angles in keeping with the overall cohort. However, patients with symptomatic nonunion requiring revision understandably had lower postoperative scores. Our study suggests that the Lapidus procedure is a successful operation for moderate to severe hallux valgus deformity, given its high patient satisfaction, low revision, and relatively low complication rates.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114221104825 – Supplemental material for Patient-Reported and Radiologic Outcomes With the Lapidus Procedure
Supplemental material, sj-pdf-1-fao-10.1177_24730114221104825 for Patient-Reported and Radiologic Outcomes With the Lapidus Procedure by Atua Fuimaono Asafo, Heidi (Hoi Ying) Chan, Che Siu Lim and Matthew Tomlinson in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because it is a retrospective analysis of cases done by a single surgeon. All work was original and appropriate references were used throughout the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.