
Abstract
Background:
Surgeons who lack experience with total ankle arthroplasty (TAA) may remain hesitant to introduce this procedure owing to previously published results of high complication rates during initial cases. The purpose of the present study was to report the development of a TAA program through intermediate outcomes and complications for an initial consecutive series of TAA patients of a single community-based foot and ankle fellowship–trained orthopedic surgeon with little TAA experience using a co-surgeon with similar training and TAA exposure.
Methods:
The initial 20 patients following third-generation TAA with a single surgeon were reviewed. Clinical outcomes were measured and radiographs were evaluated to determine postoperative implant and ankle position. Complications were also measured including intraoperative, early (<3 months), and intermediate postoperative complications.
Results:
With a minimum follow-up of 2 years and average follow-up of 51 months (range 24-70 months), the mean American Orthopaedic Ankle & Foot Society Ankle-Hindfoot score was 87.7 (59-100) and VAS was 1.0 (0-5.5). All patients were improved following TAA. Radiographic evaluation demonstrated no evidence of component malalignment or ankle joint incongruity. There were no intraoperative complications nor any wound complications. Three patients returned to the operating room for placement of medial malleolar screw placement, and 1 had asymptomatic tibial component subsidence.
Conclusions:
Orthopedic surgeons with a proper background and updated training may be able to perform TAA with good outcomes. A TAA program was developed to define minimum training criteria to perform this procedure in our community. Our complication rate is consistent with those reported in the literature for experienced TAA centers, which contrasts previous literature suggesting increased complication rates and worse outcomes when surgeons perform initial TAAs. Utilization of an orthopedic co-surgeon was felt to be instrumental in the success of the program.
Level of Evidence:
Level IV, retrospective case series.
Keywords
Introduction
Patients with advanced ankle arthritis and failure of nonoperative management have a drastic decrease in quality of life and significant limitation with mobility. 24 Results following total ankle arthroplasty (TAA) have revealed significant improvement in pain, gait, and functional outcomes. 2,4,8 Long-term success of this procedure has been shown to be related to patient selection, technical ability, and avoiding intraoperative and perioperative complications. 11,14,23,26
TAA is a technically demanding procedure with many known complications. 5,6,10,26 Historically, the literature has reported a steep learning curve associated with successfully performing TAA. 4,6,11,12,22 Previous studies have suggested higher initial perioperative complications, with an improvement in outcomes and decrease in complication rates only after surgeon experience with the procedure. 2,7,12,20 -22,26 Because technical ability and experience with TAA are considered major predictors of successful outcomes, many orthopedic foot and ankle surgeons with little TAA experience may be hesitant to perform this procedure. This may be due to TAA experience during surgical training, and/or the surgeon may feel geographically isolated with little TAA surgeon mentorship. To our knowledge, there have not been published reports of low complication rates and good patient outcomes from inexperienced TAA surgeons since this procedure has become established.
The purpose of this study is to report the success of a TAA program initiated in a community with little surgical experience with this procedure. The program included components of arthroplasty training during orthopedic residency, foot and ankle–focused practice, training course in TAA, and mentorship with a co-surgeon with a minimal equivalent experience. Evaluation of the program was determined through intermediate outcomes and complications of a single community-based foot and ankle fellowship–trained orthopedic surgeon’s initial consecutive series of TAA patients. The surgeon had little exposure to the procedure before initiating a TAA program. The purpose of this study is to identify if proper training, background, and current fund of knowledge from the orthopedic community can aid in decreased complication rates and maintaining satisfactory outcomes while introducing TAA into an orthopedic surgeon’s practice.
Methods
Total Ankle Arthroplasty Program
The development of a TAA program was initiated in order to minimize complications while introducing this procedure to our community. Collaboration with a second orthopedic foot and ankle surgeon from a different local group with limited TAA exposure as well as with surgeons outside the community with extensive TAA was sought to determine minimum parameters to perform this procedure. From this, hospital privileges were developed specifically for TAA through the medical staff and hospital bylaws (Table 1).
Hospital Requirements for Total Ankle Arthroplasty Privileges.
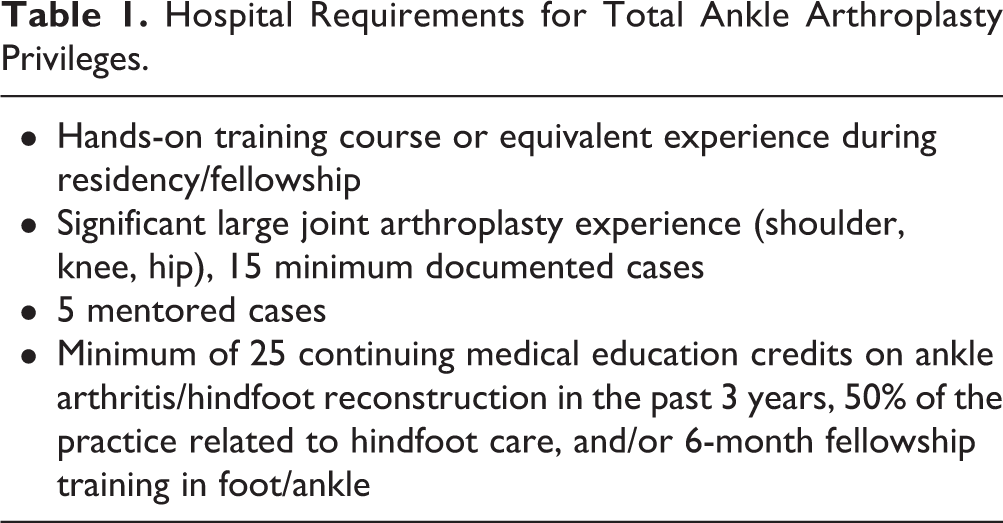
Neither surgeon had significant TAA training during fellowship and were at least 4 years out from fellowship in private practice prior to performing any TAAs. Before performing a TAA, both surgeons independently attended the implant company’s instructional and cadaveric training course. In addition, they traveled to observe a well-experienced surgeon perform 3 TAAs. Finally, all of the TAA cases in this study were performed in conjunction with the other community orthopedic foot and ankle surgeon, utilizing both the knowledge and perspective of each surgeon throughout the case. Both met the hospital’s requirements developed for TAA privileges.
Patient Selection
The initial 20 patients following TAA with a single surgeon were recorded and reviewed. Preoperative radiographic evaluation included standing 3-view radiographs. Each of these patients had failed nonoperative management for end-stage ankle arthritis. Additional indications for TAA were coronal plane deformity less than 15 degrees and minimal or no ankle instability. Exclusion criteria included younger age (<45), significant ankle instability, peripheral neuropathy, and history of infection. Inflammatory arthritis and diabetes mellitus were not considered contraindications. This study was approved by our institutional review board panel.
A total of 23 patients met the inclusion criteria and underwent TAA with a tri-component, mobile-bearing device by a single surgeon. Three patients were lost to follow-up, leaving 20 patients available for review with a minimum follow-up of 2 years. Average clinical and radiographic follow-up was 51 months (range 24-70 months). Average age was 66.4 years (range 46-79 years) and 42% had comorbidities. All patients were nonsmokers. Etiology of the underlying arthritis was post-traumatic (63%), inflammatory arthritis (10%), and primary osteoarthritis or unknown (27%).
Operative Procedure
All TAAs were performed with a third-generation mobile bearing design (STAR, Stryker, NJ) and were performed in accordance with the technique guide. Two patients had prophylactic screws placed across the medial malleoli intraoperatively to avoid potential postoperative stress fracture. Postoperatively, patients were kept non-weightbearing in a splint for 2 weeks, followed by partial weightbearing in a boot for another 2 weeks. At 4 weeks, patients were allowed to advance weightbearing to tolerance in the boot with transition to normal shoe wear and full weightbearing at 6 weeks postoperatively. All patients began physical therapy at 2 weeks postoperatively.
Clinical Outcomes
Clinical outcomes were measured using both the American Orthopaedic Ankle & Foot Society (AOFAS) Ankle-Hindfoot Score and visual analog scale. These data were obtained at postoperative visits with a minimum follow-up of 2 years. Patients were also asked whether postoperative ankle pain and function were improved compared with their preoperative condition.
Radiographic Outcomes
Postoperative standing anteroposterior, lateral, and oblique radiographs were obtained at 6 and 12 weeks, and then on a yearly basis. Both coronal and sagittal alignment were measured using previously published techniques on both preoperative and latest postoperative radiographs (Figures 1 and 2). 1,17

Coronal alignment measured by evaluating the tibiotalar angle both pre- and postoperatively.
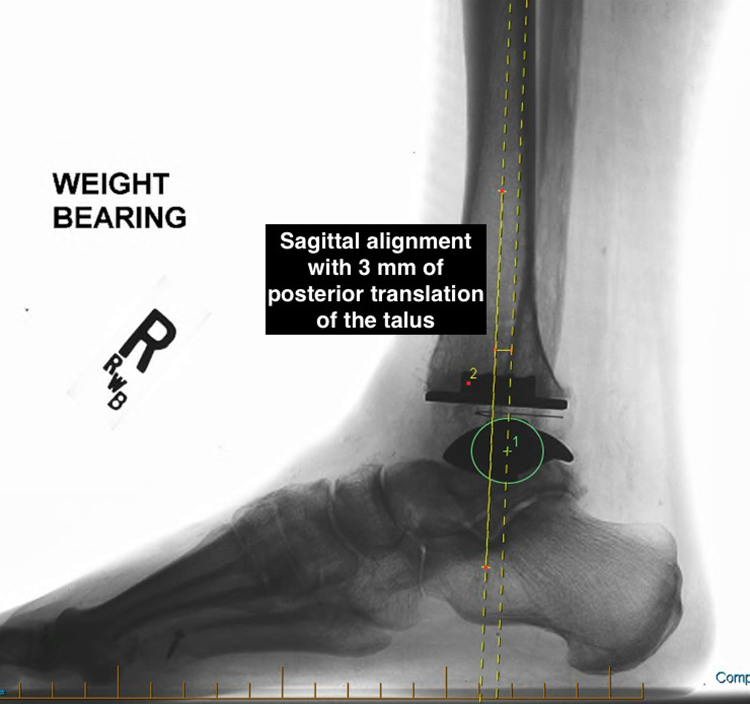
Sagittal alignment measured by evaluating the center of the talus in relation to the long axis of the tibia.
Complications
Complications measured included both intraoperative and early or late (>3 months) postoperative complications. Potential complications evaluated included infection, wound problems, malalignment, malleolar fracture, nerve or tendon injury, soft tissue impingement, heterotopic ossification, or need for second surgery related to the ankle joint or prosthesis.
Results
Clinical Outcomes
Mean AOFAS Ankle-Hindfoot score was 87.7 (range 59-100). The mean visual analog scale score was 1.0 (range 0-5.5). When asked if ankle pain and function improved following TAA, all patients answered yes (Table 2).
Summary of Clinical and Radiographic Outcomes of the Present Study.
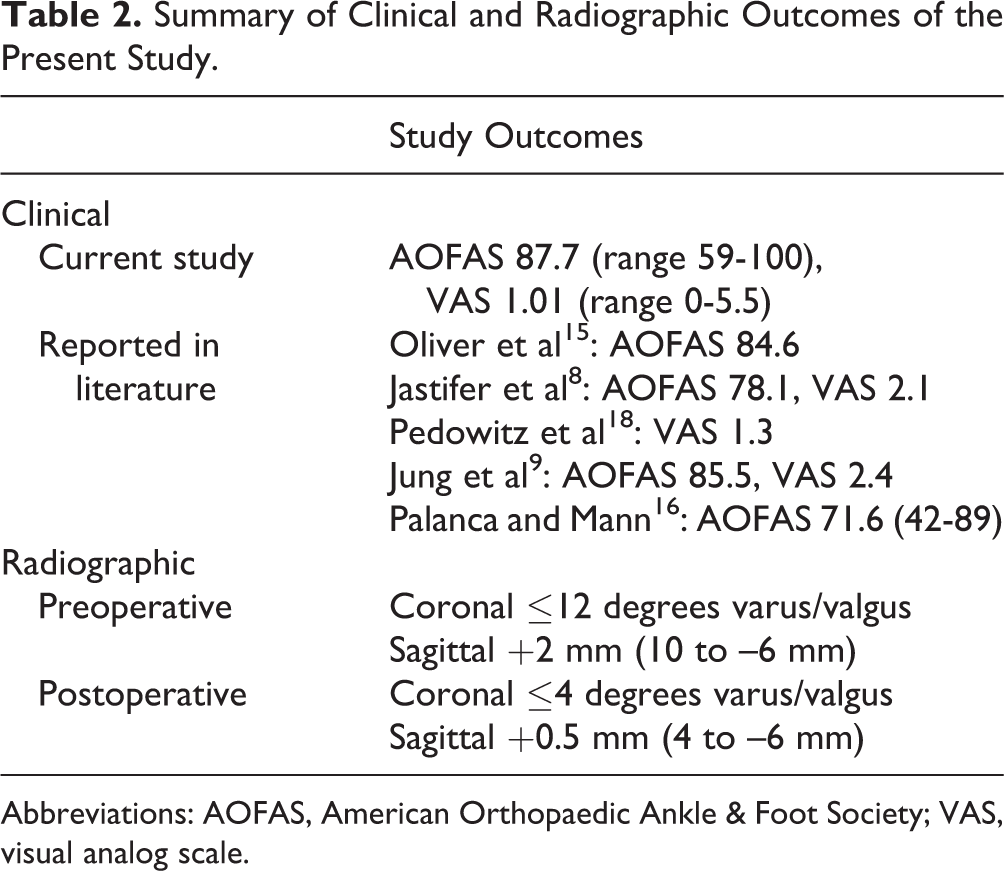
Abbreviations: AOFAS, American Orthopaedic Ankle & Foot Society; VAS, visual analog scale.
Radiographic Outcomes
Radiographic evaluation demonstrated no evidence of malalignment of any of the components. Significant postoperative malalignment was considered to be >5 degrees of valgus or varus, or greater than 10 mm of anterior or posterior translation of the talus from the long axis of the tibia. 1,17 The range of preoperative coronal alignment for the present study was no greater than 12 degrees of varus or valgus preoperatively, and none greater than 4 degrees of varus or valgus postoperatively (Table 2). The average preoperative sagittal alignment was 2 mm of anterior talar translation (range 10 mm anterior to 6 mm posterior translation). Postoperatively, the average sagittal plane alignment was 0.5 mm of talar translation (range 4 to –6 mm). All patients maintained acceptable radiographic alignment at most recent follow-up (Table 2).
Complications
Among the 20 total patients, there were no intraoperative complications. There were no immediate postoperative complications including wound complications, dehiscence or superficial skin infection, or intraoperative nerve injuries. In our series, we had a total of 4 (20%) patients with late complications (>3 months). Three patients (15%) returned to the operating room for a procedure related to their total ankle. All 3 patients had placement of percutaneous medial malleolar screws in a well-aligned TAA at an average of 14 months (range 5-21) postoperatively due to a painful stress riser as previously described. 19 Postprocedure, their pain level was markedly improved. Another patient (5%) had mild asymptomatic anterior subsidence of the tibial component that did not require revision. In addition, none of the patients developed any medical complications such as DVT or required postoperative hospitalizations (Table 3).

Discussion
The results of this study suggest that with proper background and updated training, a community-based orthopedic foot and ankle surgeon with little TAA experience can successfully introduce this procedure into their practice, as patient outcomes and complication rates were comparable to that published by experienced TAA centers. We believe important factors for this success include extensive arthroplasty training during residency, training course specific to the implant, exposure to an experienced TAA surgeon, the use of an orthopedic co-surgeon, and reviewing the expanded literature related to operative technique and patient selection. This is the first study to our knowledge that reports complication rates similar to experienced TAA centers when a qualified surgeon introduces TAA into his or her treatment options for end-stage ankle arthritis.
Historically, the literature has suggested that surgeon experience influences TAA complication rates. Haskell and Mann 4 compared experienced orthopedic foot and ankle surgeons’ complication rates for their initial and subsequent procedures. They reported a 3.1 times higher rate of having a perioperative adverse event and a 3.2 times higher chance of having a perioperative wound problem when less familiar with the procedure. 7 Wood and Deakin 25 reported a decrease of perioperative fractures and wound complications after their first 100 TAAs from 25% and 7% to 13% and 2%, respectively. 13 Lee et al 11 grouped 60 consecutive patients into group A (first 30 TAAs) and group B (second 30 TAAs). They reported a 36.7% complication rate in Group A, and a 16.7% complication rate in group B. More recently, Pangrazzi et al 17 identified a 25% technical error rate in their first 20 patients and an 8.3% rate in their subsequent patients. Saltzman et al 21 compared 3 groups for complications following placement of each surgeon’s first 10 Agility TAAs. The groups were surgeons who observed the implant inventor, surgeons who attended an operative training course, and surgeons who were trained during an orthopedic foot and ankle fellowship. There was no difference noted between the 3 groups. 20 Clement et al 2 published their initial series of 27 patients with an overall perioperative complication rate of 34%, which included 2 intraoperative fractures, 2 component misalignments, and 5 wound complications. Our study cohort had no intraoperative or early postoperative complications, which is lower than that reported in the above studies.
Complications following TAA are well reported in the literature. Glazebrook et al 3 reported an overall average complication rate approaching 12.4% (range 1.3%-32.3%). Wound problems, fractures, nerve injuries, component loosening/subsidence, tendonitis, joint stiffness, implant failure, infection, and DVT have all been described. 7,13,25 Influence of these complications on long-term outcomes can vary, and intervention required for resolution follows the spectrum from minimal and quick to long-standing disability.
The findings of the current study contradict previous reports associating early TAA with a steep learning curve and suboptimal outcomes as a result. Unlike past literature, in the present study there was no evidence of component malalignment, no intraoperative fractures, and no wound complications among the first 20 TAA performed by a single foot and ankle–trained orthopedic surgeon with minimal prior TAA experience.
Reports in the literature identify a reoperation rate between 3% and 33% and early failure rate of 3% to 15% for TAA. 3,8,12,15,17 Three patients (15%) with neutral prosthetic alignment did return to the operating room for placement of medial malleolar screws for a painful stress riser, which resolved their medial pain. This has become a common procedure we now perform intraoperatively since this problem was identified. 19 One patient had subsidence of the tibial component that remained stable and painless. Otherwise, at a minimum of 2 years postoperatively, there were no other complications or evidence for implant failure. These categories of complications are considered minor, and patients are expected to ultimately have no influence of final outcome. 22 In addition, these are comparable to reported complication rates in the literature for more experienced orthopedic surgeons (Table 3).
In addition to the complication rate, the clinical outcomes of the current study are also consistent with those reported in the literature. With a mean AOFAS score of 87.7 (range 59-100) and a mean VAS score of 1.0 (range 0-5.5). Further, all of the patients in our study stated they would have the procedure again and were satisfied with their surgery. Our outcomes are consistent with satisfaction rates and AOFAS and VAS scores reported in the literature (Table 2). 3,8,15 Although AOFAS is not a validated scoring mechanism for TAA, its value to the current study is to allow comparison of our results to those from centers with high-volume TAAs.
We attribute the success of our TAA program to multiple factors. Both proper training and background principles found in orthopedic surgery residency are paramount to the success of initial TAA. This includes the extensive large joint arthroplasty exposure (shoulder, knee, hip) residents obtain during their years of training, including both hands-on training, thus learning important arthroplasty principles. In addition, a hands-on TAA training course or equivalent during residency or fellowship is also important for the surgeon to have a foundation of the procedure and a familiarity of the instrumentation of the specific implant they intend to use. Second, a broad understanding of foot and ankle biomechanics, pathology, and anatomy is critical for proper implant balancing and deformity correction. Finally, the value of a mentor cannot be overstated. An experienced TAA surgeon would be ideal, however, if this is not available, another orthopedic colleague with foot and ankle or arthroplasty experience was found to be extremely helpful. In addition, implant companies may have surgeon mentors available to the inexperienced surgeon. Although an orthopedic foot and ankle specialist co-surgeon was present for all 20 procedures in this study, our anecdotal experience suggests that surgeon’s comfort and confidence with the procedure develops after approximately 10 TAAs. In addition, we started an orthopedic foot and ankle fellowship after initiating our TAA program. Generally, after approximately 10 cases, the fellows appear to understand the nuances of the device and the anatomic consideration of the differences between ankle arthritis presentations. Because of our impression of the importance of these factors for a successful TAA program, they are represented in the hospital privilege requirements at all the hospitals in our community (Table 1).
Perhaps the greatest component of success for our TAA program is the volume of information available at the time of initiation compared to when the initial studies were published. A PubMed search for “Ankle Arthroplasty” identified 456 papers in the 5 years prior to initiating our program (January 2006–December 2010). In the 5 years prior to this (January 2001–December 2005), 223 articles were published. This information added much to our knowledge of TAA regarding patient selection, operative techniques, and identifying/avoiding complications. This speaks to the statement related to the forward progress of medicine that we “stand on the shoulders of giants.”
There are limitations with the current study. The study only evaluated 1 orthopedic surgeon’s experience in the present study. Evaluating a greater number of patients’ outcomes for surgeons who introduced TAA into their practice would have provided more support for our conclusions. Second, being the first independent TAAs performed in the surgeon’s career, indications for patient selection were strict, resulting in mostly healthy individuals with minimal deformity. This obviously increases the odds for successful outcome, and results may have been less favorable with a more difficult patient population. We feel, however, that this is an important concept for any surgeon introducing a new procedure. There were also no preoperative clinical outcomes measured for the patient population in this study, and we used the AOFAS score, which is not validated for TAA outcomes. As a result, there was no baseline for clinical comparison of postoperative outcome values, other than comparing to reported outcomes in other studies in the literature. With that said, historical preoperative scores are consistent in the literature, and the clinical outcomes for this study were comparable with those reported in the literature. Although a validated score, such as the Ankle Osteoarthritis Scale would have provided a better outcome measure of our patient population, it would not have allowed comparison to those studies published from institutions with large volumes of TAA, which primarily reported AOFAS scores.
Conclusion
Introducing new procedures into practice can be intimidating for surgeons. Once procedures are established, a surgeon with the proper background and procedure training may be able to perform the surgery safely with good outcomes. Orthopedic surgeons with a proper background and updated training may be able to perform TAA with good outcomes. A TAA program was developed to define minimum training criteria to perform this procedure in our community. This is the first study to our knowledge reporting complication rates consistent with those reported in the literature for experienced TAA centers, which contrasts previous literature suggesting increased complication rates and worse outcomes when surgeons perform initial TAAs. Utilization of an orthopedic co-surgeon was felt to be instrumental in the success of the program. Based on the results of this study and the much-improved understanding of TAA technique and patient selection, qualified surgeons with little TAA experience or exposure should be able to perform the procedure safely. This is particularly valuable to those community surgeons who are geographically limited to mentorship such as those in developing countries where TAA has not become a standard treatment for endstage ankle arthritis.
Supplemental Material
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420985780 - Early Outcomes and Complications Following Initiation of a Total Ankle Arthroplasty Program
Supplemental Material, sj-pdf-1-fao-10.1177_2473011420985780 for Early Outcomes and Complications Following Initiation of a Total Ankle Arthroplasty Program by Gregory Lundeen, Kaitlin C. Neary, Cody Kaiser and Lyle Jackson in Foot & Ankle Orthopaedics
Footnotes
Acknowledgment
We would like to thank Richard Hayes, MD, for his assistance in developing the total ankle program.
Ethics Approval
The institutional review board exempted approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.