
Abstract

Introduction
Anterior ankle impingement is one of the most common causes of chronic ankle pain especially in athletes such as soccer players and dancers. 15 Anterior ankle impingement is a syndrome characterized by pain elicited by dorsiflexion and may show restriction to active and passive ankle dorsiflexion. Historically, ankle impingement is separated by anatomical location and lesion type. This can be characterized radiographically or intraoperatively as either soft tissue or osseous structures causing impingement. Furthermore, pain in certain anatomical locations can help delineate the pathology. Soft tissue impingement is found typically in the anterolateral aspect, and osseous is typically found anteromedially. 14
The etiology is thought to be due to the chronic repetitive dorsiflexion or inversion seen in athletic movements such as in long-distance running, acceleratory changes in motion, or even plié or demi-plié positions of ballet. 12 This repetitive trauma results in the formation of talotibial osteophytes, which can entrap soft tissue causing pain. 11 In addition, these osteophytes can cause swelling and restriction to the biomechanical motion of the ankle joint. A cadaveric investigation by Talbot et al 10 revealed that spurs were found in the anterolateral talus in 78% of their specimens and also in 80% of the anterolateral portion of the distal tibial margin.
Initial treatment for ankle impingement is typically conservative consisting of rest, shoe modification, over the counter anti-inflammatory medications, and physical therapy. However, if pain persists, intra-articular glucocorticoid injections may be employed. Failure of conservative management leads to arthroscopic or open procedures. There has been adequate data showing satisfactory results with open modalities; however, arthroscopic management is less invasive and has shown a decrease in recovery time. 9 Currently, arthroscopic management is the most popular treatment method of ankle impingement due to safety and efficacy. 15 It has shown to be widely effective with both anterolateral and anteromedial ankle impingement with excellent outcomes and low complication rates. 7,15
Anatomic variants are an important concept in the evaluation and treatment of ankle impingement syndrome. A common variant seen in ankle impingement is the distal fascicle of the anterior inferior tibiofibular ligament or Bassett’s ligament. 13 Furthermore, an accessory ossicle known as os talotibiale can cause anterior impingement. 4
We present the case of a middle-aged man with ankle impingement refractory to previous arthroscopic procedures. Open operative management revealed an anomalous band of the anterior deep deltoid and a medial cam lesion just proximal to the talar neck with an abnormal alpha angle. Our purpose is to alert orthopedic providers about this anatomic variant producing ankle impingement. A search of the literature revealed no previous report of anteromedial ankle impingement in the setting of anterior deep deltoid variant anatomy.
Case Report
A 49-year-old man was seen in clinic for right chronic anteromedial ankle pain. He previously underwent 5 ankle arthroscopies by an outside surgeon without significant pain relief. On examination, tenderness was noted around the anterior aspect of the ankle, with good strength about the ankle, and a negative anterior drawer. A previous rheumatologic workup was negative despite a family history of rheumatologic disease. Radiographs were notable for a subtle cavus foot but otherwise unremarkable.
Despite multiple bracing attempts, the patient continued to have pain, and a bone scan was obtained. This was unremarkable for a source of pain. Subsequently, a CT scan of the right ankle demonstrated no obvious pathology, including a comparison to the asymptomatic contralateral ankle.
The patient presented a year later and while obtaining a lateral radiograph, he was asked to slightly flex the knee with his foot planted on the ground. This reproduced a visible translation of his tibia relative to the foot. Further examination revealed significant anteromedial ankle pain with loaded dorsiflexion, consistent with impingement. A planned open procedure for partial talus excision, with possible calcaneonavicular coalition excision and heel cord lengthening, was discussed, and the patient agreed to proceed.
In the operating room, an anteromedial incision and arthrotomy were used to expose the tibiotalar joint. The synovium was chronically inflamed. A thickened and scarred anterior deep deltoid ligament caused ankle impingement with forced ankle dorsiflexion. This was sharply excised (Figure 1). A cam lesion was noted along the anteromedial talar neck just distal to the articular surface. An osteotome was used to remove this bone.

Intraoperative view of the thickened and scarred anterior deep deltoid ligament, which was sharply excised.
With the excision of the anterior deep deltoid ligament, inflamed synovium, and talar cam lesion, there was no further anteromedial impingement with dorsiflexion. The ankle was stable to anterior drawer and external rotation stress tests under fluoroscopy (Figure 2).

Fluoroscopy images (A-D) show dorsiflexion with impingement of CAM lesion. (D) Fluoroscopy image after CAM lesion excision.
Postoperatively, the patient was weightbearing as tolerated and seen in clinic for suture removal. He underwent physical therapy for range of motion and gait training. At his 12-week follow-up, he reported resolution of impingement symptoms.
Discussion
Our patient presented with persistent symptoms of anteromedial ankle impingement refractory to conservative management and multiple arthroscopies. Intraoperatively, an anomalous band of the anterior deep deltoid and a medial cam lesion just proximal to the talar neck were noted to be the causes of impingement.
A PubMed search on cam lesions of the talus reported only 1 study. Amendola et al 1 reported a prevalence of 34% of cam-type ankle impingement. The authors defined the cam ratio as the sagittal height of the talar neck compared to the talar body on a lateral weightbearing radiograph. They also defined the alpha sign and calculated the alpha angle. First, a circle is superimposed to match the radius of curvature of the tibial plafond. Two additional circles are drawn matching the curvature of the medial and lateral talar dome. An alpha sign exists if the radius of the talar dome exceeds the radius of the anterior portion of the continuation of the talus. To calculate the alpha angle, a vertical line is drawn to bisect the circle. A second line is drawn from the midpoint of the circle “to the anterior point at which the radius is exceeded as part of the normal continuation of the talus” (Figures 3 and 4). 1 These authors also cite a flattened talar dome or a thickened anterior neck just distal to the articular surface as sources of cam-type impingement. Our case is an example of the latter.

Lateral view of an ankle with standard measure of the alpha angle of the medial and lateral talar domes.
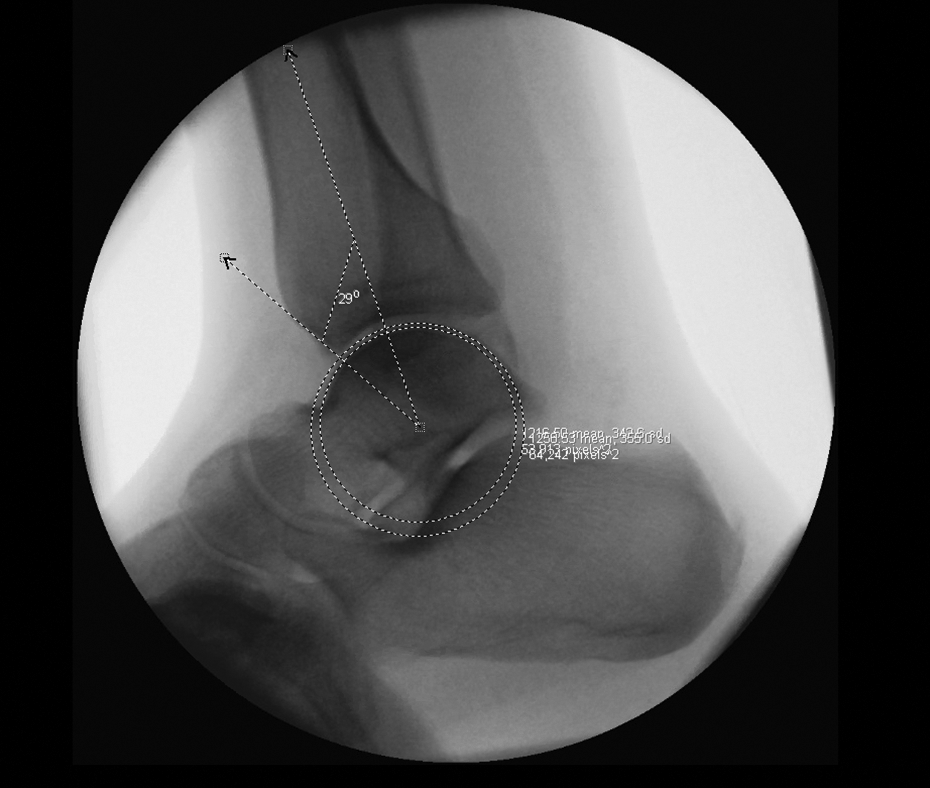
Lateral view of our patient’s ankle with measurement of the alpha angle of the medial and lateral talar domes.
Boss and Hintermann identified 5 main ligaments compromising the deltoid complex. 2 The deep anterior tibiotalar ligament was present in 6 of 12 specimens. 2 In contrast, Milner and Soames 6 found the deep anterior tibiotalar ligament in just 4 of 40 specimens. A recent article by Panchani et al 8 identified 8 bands of the deltoid ligament, but a deep anterior tibiotalar ligament was not named. An anatomical study by Campbell et al 3 identified 13 of 14 (93%) specimens with a deep anterior tibiotalar ligament (Figures 5 and 6).

Gross dissection of the deep layer of the deltoid ligament of a left ankle. Two ligamentous bands composed the deep layer in this specimen and include the deep anterior and posterior tibiotalar ligaments.

Illustration of the medial view of the deep deltoid ligament in a left ankle showing the anatomic attachment sites of the deep anterior and posterior tibiotalar ligaments.
Considerable variance exists with the deltoid complex. We believe that our patient had a band most similar to the deep anterior tibiotalar ligament in the studies by Milner et al, Boss and Hintermann, and Campbell et al originally defined this ligament citing its origin as the anterior colliculus and intercollicular groove of the medial malleolus and insertion on the medial surface of the talus just distal to the anterior part of the medial articular facet. 5 This description highlights the proximity to a potential cam lesion on the anteromedial talus, which could then result in impingement of this ligament.
In conclusion, osseous structures of the anterior rim of the tibia remain the most common causes of anteromedial impingement and soft tissue structures for anterolateral impingement. 14 However, it may be advantageous to evaluate for less common causes of impingement because of variant anatomy in patients with symptoms refractory to conservative and arthroscopic management. Open treatment may be required to appreciate a combined cam lesion and deep deltoid impingement, especially in cases with previous arthroscopic treatment. Recognizing and appropriately treating these uncommon sources of ankle impingement could improve patient outcomes.
Supplemental Material
Supplemental Material, FAO977427-ICMJE - Anteromedial Ankle Impingement Due to a Talar Cam Lesion and Anterior Deep Deltoid Ligament With Variant Anatomy: A Case Report
Supplemental Material, FAO977427-ICMJE for Anteromedial Ankle Impingement Due to a Talar Cam Lesion and Anterior Deep Deltoid Ligament With Variant Anatomy: A Case Report by Scott R. Glenzer, Grayson A. Domingue and Mark D. Perry in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Ethical approval was not sought for the present study because it was not applicable nor necessary to our case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.