
Abstract
Background:
An understudied area of proximal first metatarsal osteotomies is the effect on articular contact properties following the surgeries. Potential long-term risks include altered joint mechanics and possible arthritic progression. A biomechanical comparison of articular characteristics of the proximal opening wedge and Ludloff osteotomies was performed in this study. It was hypothesized that the proximal opening wedge osteotomy (POWO) would lead to greater alterations in articular contact properties along the first ray.
Methods:
Seven paired fresh-frozen below-knee cadaveric limbs with hallux valgus were selected. Specimens in each pair were tested in the intact state and then randomized to receive either a Ludloff or POWO. A 4-mm opening wedge osteotomy was used in all cases. Loading of the flexor hallucis longus was to 100 N using an instrumented tensioner. A 28-N load was added at the distal phalanx to simulate the ground reaction force. First metatarsophalangeal (MTP) and tarsometatarsal (TMT) articular properties were recorded simultaneously using 2 pressure sensors. For each state, a pressure map was generated and contact area, peak pressure, and center of pressure were calculated. Wilcoxon signed-rank test was used to assess statistical significance.
Results:
Average peak pressure was noted to be elevated at the MTP (4.6 vs 6.9 mPa, P = .04) and TMT (3.3 mPa vs 5.1 mPa, P = .30) joints when comparing the Ludloff and the POWO, respectively. Contact area was also noted to be lower in the POWO relative to the Ludloff for the MTP (86.6 vs 69.1 mm2, P = .30) but not the TMT joints (89.1 vs 88.5 mm2, P = .97). There was a slight plantar-lateral and dorsomedial shift in pressure at the MTP and TMT articulations, respectively, of the POWO relative to the Ludloff. A trend toward decreased contact force within the TMT joint was noted following opening wedge osteotomy relative to the intact state (103.8 vs 113.9 N, P = .31), while forces were elevated at the MTP joint (104.3 vs 96.0 N, P = .63), although not statistically significant. Smaller increases in TMT and MTP joint forces were noted following the Ludloff when compared to the intact state (95.6 vs 93.3 N at TMT and 109.2 vs 103.2 N at MTP).
Conclusion:
POWO can potentially change articular contact characteristics along the TMT and MTP articulations of the first ray. This could possibly lead to altered loading patterns and possible long-term damage vs other osteotomies.
Clinical Relevance:
While it is unlikely that the changes observed with the sizes of the osteotomy commonly used would lead to long-term significant clinical consequences, further study with larger group sizes would be beneficial.
Background
Hallux valgus is one of the most common conditions encountered by the foot and ankle surgeon, with an estimated prevalence of 23% to 35%. 11,12,18 For moderate to severe deformities, a proximally based osteotomy is often used to correct them. 12,15,19 -21 Many osteotomy approaches have been developed and applied in the past several decades, such as proximal opening wedge, modified Ludloff, proximal crescentic, and proximal chevron osteotomies. However, complex 3-dimensional hallux valgus raises many concerns regarding these correction techniques, including technical difficulty, control of metatarsal length, elevation, rotation, nonunion, and stability. 5- 7 As a result, controversy exists as to which osteotomy should be used for a specific patient. Proximal opening wedge osteotomy (POWO) was first described in 1923. 8,14,15 It had historically been seldom used due to concerns of reduced stability, potential for nonunion at the osteotomy site, and metatarsal lengthening. 2,4,8,20 More recently, studies evaluating this technique have emerged for its technical ease, reproducibility, and improved stability with a low-profile plate. 14,20,21 In fact, in a prospective, randomized study, surgeons favored the POWO in comparison to a proximal chevron osteotomy. 7
An understudied area with respect to hallux valgus surgery is the effect of osteotomies on articular contact characteristics of the first ray and the potential for altered joint mechanics and arthritic progression over time. A clinical concern of the POWO is the lengthening of the first metatarsal that occurs and its potential to alter articular contact properties. 2,8,15,20 A recent investigation demonstrated that the POWO relative to the scarf did not lead to elevated pressure or force across the metatarsophalangeal (MTP) joint. 8 Alterations are perhaps more likely to occur at the tarsometatarsal (TMT) articulation given the proximity of the proximal osteotomies to this joint. An additional study demonstrated that the use of the proximal TightRope (Arthrex, Naples, FL) is effective in correcting the intermetatarsal (IM) angle but can increase contact pressure along the dorsomedial aspect of the first TMT joint as well. 13
The purpose of this study was to evaluate the articular contact pressure changes at the MTP and TMT joints following a POWO, in contrast to a Ludloff osteotomy that is generally associated with metatarsal shortening. 1,22 It was hypothesized that a POWO would lead to greater increases in contact pressure at the TMT joint than the MTP joint relative to a modified Ludloff osteotomy. The primary outcome of the study was to determine if POWO resulted in a greater increase in contact pressure at the MTP and TMT articulations relative to the Ludloff. A secondary outcome was to determine if there was a shift in the center of pressure at the respective joints following the osteotomies.
Methods
Seven paired fresh-frozen, below-knee cadaveric limbs with hallux valgus were selected. Specimens were screened for prior surgery, trauma, and overt pathology. They were stored in a –10°C freezer and allowed to thaw to room temperature prior to the procedures. The first ray inclusive of the navicular-medial cuneiform articulation was dissected and potted in resin. All skin and subcutaneous tissue were removed to facilitate testing. The flexor hallucis longus (FHL) was dissected and isolated. Testing was conducted in a customized apparatus with the cuneiform pinned to the apparatus and positioned at 10 degrees of declination to simulate forefoot loading during the midstance phase of gait (Figure 1). 9,10 Loading of the FHL was to 100 N using an instrumented tensioner with a load cell (LCCD-1 k; OMEGA Engineering, Norwalk, CT). A 28-N load was added at the distal phalanx to simulate the ground reaction force, stabilizing the hallux such that a static equilibrium could be attained. 9,10 Specimens were tested in the intact state whereby medial capsulotomies of the first ray MTP and TMT articulations were performed. Two sensors (K-Scan 6900; Tekscan, Boston, MA) were inserted into the MTP and TMT joints simultaneously and held by the native constraint of the articulation. Sensors were preconditioned and calibrated similarly. The sensors were calibrated before testing by loading them on a servohydraulic frame (MTS Systems, Eden Prairie, MN) with a 50-N and 100-N load for 30 seconds, using a 2-point calibration technique. 9 No additional suturing or alternate fixation methods were used to avoid damaging the sensors. Upon loading, a pressure map was generated at the respective articulations, and contact area, peak pressure, and center of pressure were calculated. The sensors were subsequently removed prior to performing the osteotomies.

Biomechanical testing setup. Tekscan sensors were inserted into the medial aspect of the metatarsophalangeal and tarsometatarsal articulations simultaneously. A metal pin placed through the medial cuneiform was used to maintain alignment of the first ray during testing.
Surgical Technique
Specimens in each pair were randomized to receive either a Ludloff or POWO (Figure 2). For the Ludloff, an oblique osteotomy of the proximal two-thirds of the metatarsal shaft in a proximal dorsal to distal plantar direction was performed using an oscillating saw. The osteotomy began dorsally 1 cm distal to the first TMT joint, extending in a distal and plantar direction and ending just proximal to the metatarsal-sesamoid articulation. The distal fragment was then rotated 30 degrees and secured with a dorsal Ludloff-specific plating system (MetaFix Ludloff; Merete Technologies, Oakbrook Terrace, IL).

Specimen preparation: Top: Specimen fixed with proximal opening wedge osteotomy; bottom: specimen fixed with Ludloff.
Similar to prior investigations, for the POWO, an oblique osteotomy was performed starting 15 mm distal to the first TMT articulation and angled proximally such that it terminated at the lateral cortex 5 mm from the TMT joint. 3,12,15 Care was taken to preserve the integrity of the lateral cortex. Stacked osteotomes were used to gently open the osteotomy site. Guides were not used for either osteotomy. Fixation was then accomplished with a 4-mm opening wedge plate (MetaFix Opening Wedge Plate; Merete Technologies). Due to budgetary constraints, only a 4-mm osteotomy was performed. It was a midrange osteotomy that is commonly performed to achieve IM deformity correction. 21 It was also felt that this would sufficiently contrast with the Ludloff to assess articular contact properties. Repeat biomechanical testing was then performed as previously described.
Statistical Analysis
As the sample size was limited in this study, a nonparametric method, Wilcoxon signed-rank test, was used to assess statistical significance using SAS software (SAS Institute, Cary, NC). Normality of the data was assessed using the Shapiro-Wilk test. As normality was not consistent across groups of data, the Wilcoxon signed-rank test was used. A 2-sided significance level of .05 was used.
Results
Compared to intact specimens (Table 1), the Ludloff osteotomy slightly decreased the average peak pressure in both MTP (4.9 vs 4.6 mPa, P = .90) and TMT (3.5 vs 3.3 mPa, P = .92) joints but was not significant. It also slightly increased the contact area at both joints (84.1 vs 86.6 mm2 at MTP and 85.3 vs 89.1 mm2 at TMT) and contact force (103.8 vs 109.2 N at MTP and 93.3 vs 95.6 N at TMT) but was not significant as well. POWO, on the other hand, increased the average peak pressure in both MTP (4.8 vs 6.9 mPa, P = .10) and TMT (4.9 vs 5.1 mPa, P = .64) joints, decreased contact area (73.3 vs 69.1 mm2 at MTP and 93.3 vs 88.5 mm2 at TMT), and mixed contact force (96.0 vs 104.3 N at MTP and 113.9 vs 103.8 N at TMT), but none was significant.
First MTP and TMT Contact Measurement Results.a
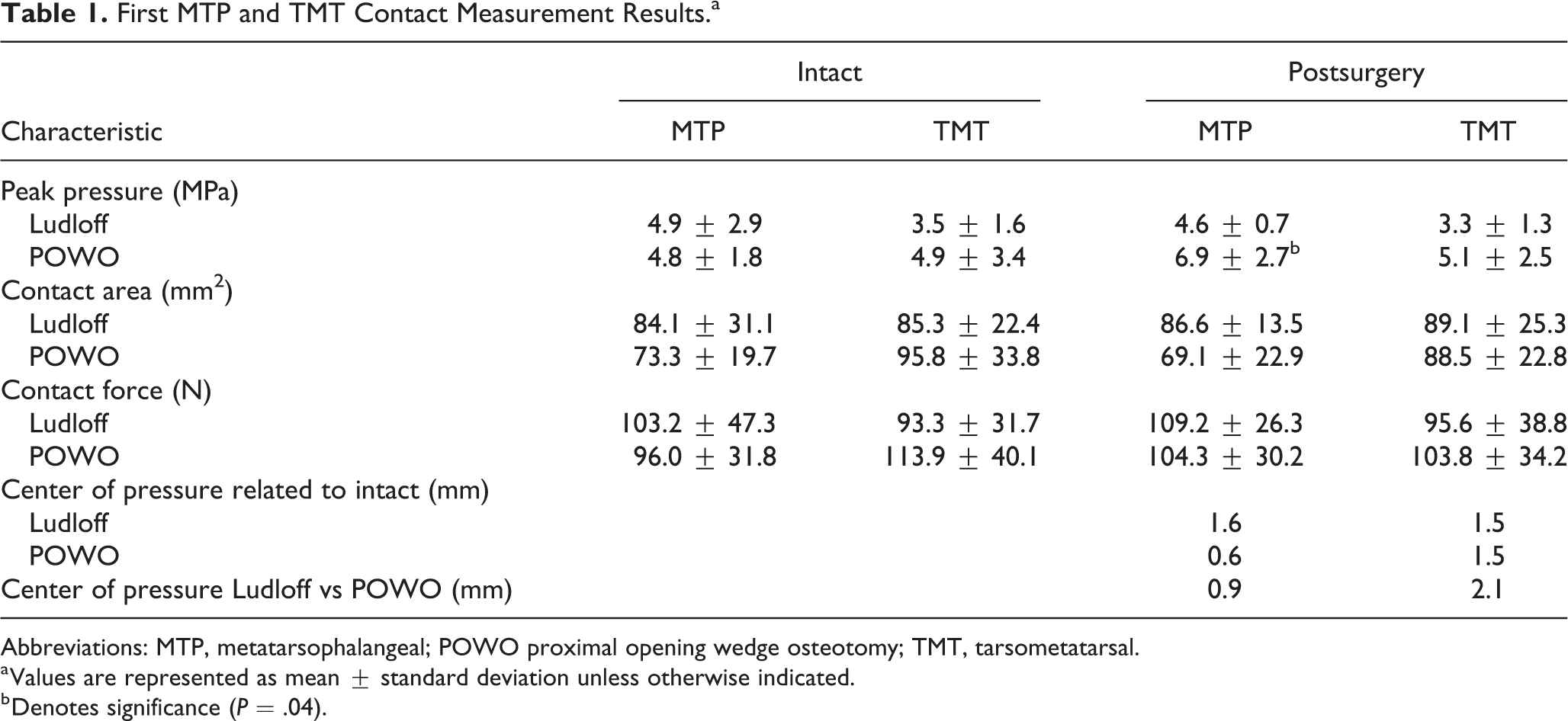
Abbreviations: MTP, metatarsophalangeal; POWO proximal opening wedge osteotomy; TMT, tarsometatarsal.
a Values are represented as mean ± standard deviation unless otherwise indicated.
b Denotes significance (P = .04).
When comparing the Ludloff and POWO, average peak pressure was noted to be elevated after POWO at the MTP (4.6 vs 6.9 mPa, P = .04) and TMT (3.3 vs 5.1 mPa, P = .30) joints, respectively (Table 1). Contact area was also noted to be lower in the POWO relative to the Ludloff states for the MTP (86. 6 vs 69.1 mm2, P = .30) but not TMT joints (89.1 vs 88.5 mm2, P = .97). POWO had higher contact force at the TMT (103.8 vs 95.6 N, P = .78) than Ludloff but not at the MTP (104.3 vs 109.2 N, P = .68).
After the Ludloff osteotomy, the center of pressure at the MTP joint moved 1.6 mm lateral and plantar (1.1 mm lateral, P = .27, and 1.2 mm plantar, P = .32) and at the TMT moved 1.5 mm medial and dorsal (0.2 mm medial, P = .99, and 1.5 mm dorsal, P = .12) relative to the intact state. After the POWO, the center of pressure at the MTP joint moved 0.6 mm medial and plantar (0.4 mm medial, P = .56, and 0.4 mm plantar, P = .83) and at the TMT moved 1.5 mm lateral and dorsal (1.1 mm lateral, P = .23, and 1.0 mm dorsal, P = .27) (Table 1). When comparing the center of pressure changes of the POWO vs Ludloff, POWO moved 0.9 mm plantar-lateral (MTP, 0.2 mm lateral, P = .93, and 0.9 mm plantar, P = .36) and 2.1 mm dorsomedial (TMT, 2.0 mm medial, P = .09, and 0.6 mm dorsal, P = .74) relative to Ludloff (Figure 3A,B and Figure 4A,B). Overall, there was noted to be a slight plantar-lateral and dorsomedial shift in pressure at the MTP and TMT articulations, respectively, of the opening wedge relative to the Ludloff.

Contact pressure distribution of metatarsophalangeal and tarsometatarsal joints (A, B) before and (C, D) after opening wedge osteotomy. A star indicates the center of contact. Lighter colors demonstrate higher areas of pressure.

Contact pressure distribution of metatarsophalangeal and tarsometatarsal joints (A, B) before and (C, D) after Ludloff osteotomy. A star indicates the center of contact. Lighter colors demonstrate higher areas of pressure.
Discussion
The operative treatment of hallux valgus remains a challenging and controversial topic, given its complexity and the myriad procedures employed to address it. POWO has been used as a means of correcting hallux valgus due to its ease and reproducibility with the advent of low-profile plates for fixation. Glazebrook et al, 7 in a randomized study, demonstrated its clinical favorability, noting that surgeons preferred it relative to the proximal chevron osteotomy as it was felt to be less technically demanding. However, a potential concern, due to metatarsal lengthening associated with this procedure, is the effect on articular contact characteristics along the TMT and MTP articulations. 2,3,8,21 This could possibly lead to altered loading patterns vs other osteotomies. Siekmann et al 21 proposed the utilization of an isometric double osteotomy correction of the first ray consisting of a proximal opening and distal closing wedge osteotomy due to a clinical concern of arthritis at the MTP joint. In a study of 32 patients with approximately 5-year follow-up, the procedure was effective in achieving improved radiographic and clinical outcomes without the development of osteoarthritis.
The results of this study demonstrated that peak pressure is significantly elevated at the MTP but not at the TMT articulation when considering the POWO relative to the Ludloff, partially validating our hypothesis. One could also infer that with greater osteotomy sizes, there would be a larger increase in MTP peak pressures. While the increase in peak pressure observed at the TMT joint was not significant, it is also possible that with larger osteotomy sizes used, a significant increase would occur. It is also conceivable that the MTP joint is more sensitive to biomechanical changes owing to its greater mobility relative to the TMT articulation. However, it is suspected that for the most commonly employed opening wedge osteotomies (3-5 mm), 21 alterations in articular contact characteristics are small in nature and unlikely to lead to significant long-term pathology. Similar observations were noted with respect to the insignificant differences seen in contact area and force. It is possible, however, that larger osteotomies would lead to greater changes in articular contact properties and increase the potential for long-term arthritic changes. In a separate biomechanical study, Kia et al 8 demonstrated that while the opening wedge osteotomy led to elevated contact pressure and force across the MTP joint relative to the scarf osteotomy, the results were not significant. The study itself was also limited by small group sizes.
The changes in the center of pressure are interesting to note. Relative to the intact state, the Ludloff caused a plantar-lateral and dorsomedial shift at the MTP and TMT articulations, respectively, which is feasible given the orientation of the osteotomy. For the POWO, the changes observed in the center of pressure are likely related to its inherent geometry. As it has a medially based wedge, it would be expected for the center of pressure to translate laterally at the TMT, although it was slight. There was a similar plantar shift in pressure at the MTP joint for both the Ludloff and POWO relative to the intact state. When comparing the POWO relative to the Ludloff, there was a plantar-lateral and dorsomedial shift in the center of pressure. It is difficult to draw a meaningful conclusion from this as only 1 osteotomy size was tested and the results are insignificant, although one could surmise that the geometry of the opening wedge and its lengthening of the metatarsal would lead to these changes. In a similar biomechanical model, Kim et al 9 demonstrated a plantar shift in the center of pressure at the MTP joint following a Moberg osteotomy, which would be expected given its geometry. In a separate study, the placement of a proximal suspensory fixation device (TightRope; Arthex, Naples, FL) to reduce the IM 1 to 2 angle of hallux valgus led to a shift in pressure to the superomedial quadrant, demonstrating that correction of the IM 1 to 2 angle can lead to alterations in contact pressure. 13 Center of pressure measurements were not reported in the Kia et al 8 study.
This study has several limitations. Extrapolation of biomechanical studies to the clinical setting is difficult because they are inherently a simplification of a complex process. The model chosen in this investigation was felt to be a reasonable simulation and has been validated in prior studies. 9,10,13 It is, however, different from other studies that have evaluated articular properties within the hallux MTP joint. Kia et al 8 and Schneider et al 17 used a dorsiflexion load at the hallux of 50 N that was felt to mimic loads observed during walking. We felt that loading of the FHL during midstance phase of gait would accurately gauge articular contact properties at the MTP and TMT joints. Given the variability in the literature, it is a subject that deserves additional study. Perhaps most important, the testing apparatus as it was designed precluded the use of the entire foot, and as such, only the first ray was used in testing. The soft tissue attachments of the metatarsals are important in stabilizing the first ray, and their removal affects the clinical applicability of the results. The sensors themselves also add a level of variability in the way they are positioned in the specimen. Care was taken to maintain the proper orientation of the sensors both before and after the osteotomies were performed. The same investigator was responsible for the insertion of them during the intact and osteotomized states. The sensors were not sutured in place or secured other than by the native constraint of the articulation to avoid potential damage of the sensors and is similar to how they have been employed in prior studies. 9,16 However this inherent variability can introduce error when evaluating center of pressure in a biomechanical model. Furthermore, the effects of a concurrent distal osteotomy were not analyzed. The study itself was also underpowered at 59% to detect a difference between the 2 osteotomies due to the limited number of specimens tested. While there was a significant increase in the MTP peak pressure following POWO, a sample size of 21 specimens per group would be required to reach 80% based upon the peak pressure difference at the TMT articulation. Unfortunately, due to budgetary constraints, we were unable to acquire additional specimens to strengthen the study. Similarly, only 1 size of opening wedge osteotomy was tested, and it would have been beneficial to test larger sizes to determine if elevated articular pressure and forces would be observed.
In conclusion, we found that the POWO leads to greater alterations in contact pressures within the first MTP but not the TMT articulation relative to the Ludloff osteotomies. While it is unlikely that the changes observed with the sizes of the osteotomy commonly used would lead to long-term significant consequences, further study with larger group sizes is required to determine if this could lead to adverse effects.
Supplemental Material
Supplemental Material, FAO874051-ICMJE - Biomechanical Comparison of the Influences of 2 Proximal Metatarsal Osteotomies on First Ray Articular Contact Characteristics
Supplemental Material, FAO874051-ICMJE for Biomechanical Comparison of the Influences of 2 Proximal Metatarsal Osteotomies on First Ray Articular Contact Characteristics by Sudheer C. Reddy, Jihui Li, Daniel J. Cuttica and Mark Thiess in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sudheer C. Reddy, MD, Jihui Li, PhD, and Daniel J. Cuttica, DO, report grants from Merete, Inc, during the conduct of the study. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.