
Abstract
Background:
Infection following Achilles tendon surgery is a devastating complication and can be difficult to treat and often leads to poor outcomes. A number of treatments have been described, but there is little information concerning outcomes of these treatments. Our purpose was to evaluate the clinical and functional outcomes of patients who have undergone treatment for an infected Achilles tendon after acute and chronic midsubstance repair.
Methods:
We retrospectively reviewed the medical records of 20 patients who had undergone surgical treatment for an infected Achilles tendon between 2000 and 2016. The mean follow-up time was 21 months (range, 2-68 months). All patients underwent extensive debridement of the tendon with removal of all infected tissue and foreign material. Soft tissue wound coverage was utilized for large wounds that were not amenable to primary or secondary closure. All patients received culture-specific intravenous (IV) antibiotics for 3 to 6 weeks. Postoperatively, the extremity was immobilized in a splint followed by a cast until the wound was healed. The cast was then replaced with a walking boot and the patients were provided a physical therapy program. Functional outcomes were measured using the Foot and Ankle Ability Measure (FAAM) Activity of Daily Living (ADL) scale.
Results:
All wounds had healed at the time of last follow-up. Three patients (15%) required an unplanned return to the operating room for repeat debridement. All patients were able to walk without the use of a gait aid. Five patients (25%) required continued use of a boot or brace during ambulation. Fourteen patients participated in the FAAM ADL survey. There were 6 patients lost to follow-up. The average FAAM score was 87 (range, 71.4-100). At last follow-up, most patients reported their overall function as “normal” or “nearly normal.” Eradication of infection and satisfactory functional results can be attained after radical debridement, wound closure, and administration of culture-specific IV antibiotics.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Achilles tendon rupture is a common injury, and open surgical treatment poses the risk of infection. Tobacco use, steroid use, female sex, and diabetes have been found to increase the risk of wound complications. 4 It is estimated that there is a wound complication rate of 7% to 13% and a deep infection rate of 2% to 4% with open treatment. 6,15 A recent meta-analysis of data obtained from randomized controlled trials reported a deep infection rate of 2.36%. 16 Deep infection is a devastating complication that can lead to delays or alterations in the rehabilitation process and often results in poor clinical outcomes. 14
An infected Achilles tendon is a difficult entity to treat due to the superficial location of the tendon as well as poor tendon vascularity. 6 The goals of treating an infected Achilles tendon include eradicating infection, covering the wound, and restoring function. Multiple treatment options have been described in the literature. 2,5,7,12,13 There is a limited amount of data describing outcomes following these treatments. The purpose of this study is to elucidate the clinical and functional outcomes of patients who have undergone treatment for soft tissue infection after an open repair of an acute or chronic Achilles tendon rupture.
Patients and Methods
After approval from our institutional review board (Mayo Clinic Institutional Review Board ID#: PR16-006899-01), medical records of 32 patients were retrospectively reviewed who had undergone surgical treatment for soft tissue infection after open repair of an acute or chronic Achilles tendon rupture between February 2000 and September 2016 at a single institution. This included patients with chronic Achilles ruptures treated with allograft and flexor hallucis longus (FHL) tendon transfer. Patients who developed infections of the Achilles tendon after surgery for insertional Achilles tendonitis, calcaneal avulsion, or due to nontraumatic ulceration were excluded from the study. Twenty patients met the inclusion criteria for our study.
Within this cohort there were 14 males and 6 females, with an average age of 55 years (range, 18-81 years) at the time of their radical debridement surgery. The average time from the index surgery to the radical debridement at our institution was 10.2 months (range, 1.0-50.4 months). Two patients (10%) were smokers, 4 (20%) were diabetic, and 5 (25%) had a previous steroid injection for Achilles tendonitis. The average BMI at the time of radical debridement surgery was 30.1 (range, 18.5-35.1). Nine patients had right-sided involvement and 11 patients had left-sided involvement. The mean follow-up was 21 months (range, 2-68 months) (Table 1). Sixteen of the 20 patients had undergone primary Achilles tendon repair or reconstruction before presenting to our institution.
Summary of Baseline Characteristics.

Fourteen patients sustained injury to the Achilles tendon during activity: walking/hiking (10 patients), volleyball (1 patient), basketball (1 patient), running (1 patient), and jumping (1 patient). Six patients sustained injuries due to trauma: fall (4 patient), gunshot wound (1 patient), and laceration (1 patient). Sixteen patients underwent open primary repair of an acute Achilles tendon rupture with nonabsorbable sutures. Four patients with chronic Achilles tendon tears underwent reconstruction of the tendon: flexor hallucis longus (FHL) transfer + V-Y advancement (1 patient), hamstring autograft augmentation (1 patient), bovine substitute augmentation (1 patient), and V-Y advancement (1 patient). Prior to our radical debridement for infection, the patients had undergone an average of 2.1 (range, 1-5 procedures) surgical procedures, which include 11 patients who had undergone a debridement procedure for infection. Three patients had undergone free or local flap coverage at an outside institution. These 3 patients required soft tissue coverage as a result of nonhealing wounds after primary repair of an acute Achilles tendon rupture.
All patients underwent radical debridement of the infected Achilles tendon. The devitalized and infected tissue was removed until healthy tissue was exposed at the margins. All foreign materials (eg, nonabsorbable suture) from previous surgeries were removed. Of the 11 patients who had undergone previous debridement, there was retained foreign material found in 9 patients (suture material: 8 patients; shrapnel: 1 patient).
Intraoperative cultures were taken at the time of the debridement in all cases. A 1-stage debridement and primary closure was performed on 5 of the 20 patients (25%). Four patients (20%) underwent 2 debridement procedures prior to primary closure. Four patients (20%) underwent debridement and vacuum-assisted wound closure. One patient (5%) underwent debridement followed by split-thickness skin grafting. Four patients (20%) required local soft tissue flaps for coverage: reverse sural artery flap (3 patients) and posterior tibial perforator flap (1 patient). Two patients (10%) required coverage with a free flap: an anterolateral thigh free flap (1 patient) and a gracilis free flap with split-thickness skin grafting (1 patient) (Table 2). Only 1 patient (5%) underwent delayed Achilles tendon reconstruction after clearance of the infection.
Wound Coverage.

Postoperatively, the patients received culture-specific intravenous antibiotics for 3 to 6 weeks (mean duration of intravenous antibiotics, 34 days). All patients were immobilized in a short leg splint with the foot in neutral to slight plantar flexion. The wound was evaluated 48 to 72 hours after the final surgery, and the patient was placed into a short-leg cast if the wound appeared to be healing adequately. Patients were nonweightbearing for the duration of the cast. The cast remained in place until the wound healed, usually 4 to 8 weeks. Patients were then transitioned into a removable walking boot with gradual return to activities and were provided a physical therapy program focused on strengthening.
Functional outcomes were measured using the Foot and Ankle Ability Measure (FAAM) Activity of Daily Living (ADL) scale. To obtain the FAAM ADL score, we contacted the patients either by phone or mailed survey. Fourteen of the 20 patients (70%) participated in the FAAM ADL survey. The mean time from final surgery to participating in the FAAM survey was 6.6 years (range, 8 months–15 years). Of those who did not participate, 3 were deceased and 3 were lost to follow-up. The mean age of those who had deceased was 74 years (range, 65-85 years), with the mean time from the final Achilles surgery to death being 9.3 years (range, 4-16 years). None of these deaths were related to the Achilles tendon infection or surgery.
Results
At the time of latest follow-up, all wounds had gone on to heal (Figure 1). Three of the 20 patients (15%) required an unplanned return to the operating room for a repeat debridement procedure. Two of these cases were due to persistent deep infection. The other patient required debridement due to superficial necrosis of the gracilis free flap.

(A) Infected Achilles tendon (B) treated with debridement and (C) reverse sural artery pedicled flap (D) with complete healing of wound.
Eleven patients had a single pathogen identified from cultures: Pseudomonas aeruginosa (5 patients), Staphylococcus aureus (3 patients), Staphylococcus epidermidis (2 patients), and Streptococcus anginosus (1 patient). Cultures from 8 patients were polymicrobial. No bacterial growth was observed in 1 patient (Table 3).
Culture Results.

All patients were able to walk without the use of a gait aid (ie, crutch or cane). Five of the 20 patients (25%) continued to require an ankle foot orthosis for ambulation. Fourteen patients participated in the FAAM ADL survey with a mean time from final surgery to participating in the FAAM survey of 6.6 years (range, 8 months–15 years). The average score was 86.6% (range, 71.4%-100%). Participants in the survey rated their current overall level of function as normal (21.3%), nearly normal (64.3%), and abnormal (14.3%) (Table 4).
Functional Outcomes.
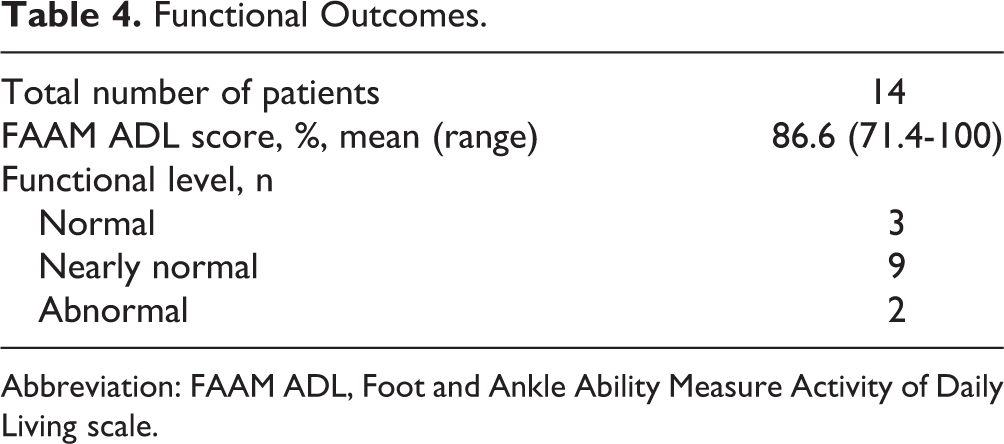
Abbreviation: FAAM ADL, Foot and Ankle Ability Measure Activity of Daily Living scale.
Discussion
Deep infection of the Achilles tendon is a devastating complication following the treatment of an acute or chronic Achilles tendon rupture. Previous studies have reported the deep infection rate to be between 2% and 4%. 6,15 Infections of the Achilles tendon alter the rehabilitation process, necessitate a return to the operating room, and have been shown to lead to poor outcomes. 14 Treatment goals include eradicating the infection, covering the wound, and then restoring function.
There have been multiple studies regarding the treatment for postoperative Achilles tendon infection. 2,3,5,7,12,13 Despite the numerous reports, there is no clear consensus regarding the optimal treatment protocol. However, most would agree that an initial step in treatment is a radical debridement of all infected, devitalized, or foreign material. 2,7 One study 9 reported suture reactions and deep infection surrounding nonabsorbable suture used for Achilles tendon repair, and therefore all the material should be removed to eradicate the infection. Prior to presenting at our institution, 11 patients with chronically infected wounds had previously undergone a debridement procedure. Intraoperatively retained foreign material was found in 9 of these patients during radical debridement. When retained foreign material is suspected in a chronically infected Achilles tendon, ultrasonographic evaluation can be used prior to debridement to try to identify and locate the material. Depending on the extent of infection, multiple debridement procedures may be necessary. In addition to a thorough debridement, cultures should be taken at the time of surgery and all patients should receive culture specific antibiotics for a period of 3 to 6 weeks depending on the type of pathogen and involvement of the calcaneus. Infectious disease specialists can be used to help guide the antibiotic therapy. In this study, 40% of the patients had a polymicrobial infection followed by P aeruginosa (25%) and S aureus (15%). Additionally, the postoperative protocol included immobilization with the foot in slight plantar flexion to reduce shear stresses on the wound. Patients were immobilized and kept nonweightbearing until the wounds had completely healed, which was usually between 4 and 8 weeks.
Soft tissue coverage following debridement is dictated by the size of the wound. There has been a wide range of treatment options described in the literature. 1 –3,5,7,8,10,11,13 Some authors have described a technique in which infections of the Achilles tendon were managed first by radical debridement followed by serial debridement and eventual soft tissue healing by secondary intention. 7 Others have performed a debridement followed by vacuum-assisted closure and eventual skin grafting over the wound. 13 If the size of the defect is not amenable to closure via primary or secondary intention, there are various local or free soft tissue flap options available. 2,5,12 These, however, can be technically difficult, have increased operative time, and have increased morbidity to both the recipient and donor sites. During our study period, all wounds had healed after utilizing various techniques.
The potential for significant functional deficits has been a concern following treatment of postoperative Achilles infections. One study compared outcomes between patients treated for rerupture and deep infection follow primary Achilles tendon repair and found that the deep infection group did not perform as well on strength testing and were restricted in their ability to participate in sports. 14 A separate study found good functional results in 3 of 4 patients following free flap coverage for Achilles tendon wounds and reported similar range of motion compared to the contralateral side. 12 Similarly, other authors reported results following combined free tissue transfer and tendon augmentation in 4 patients and found 3 with excellent clinic outcomes and 1 with a good outcome. 1 In a study previously described, 13 of 15 patients had complete resection of the tendon followed by gradual closure of the wound. 7 They reported satisfactory functional outcomes, with 9 patients able to stand on 1 foot and 2 patients able to return to sport following surgery. Another study evaluated the treatment of 15 patients with Achilles tendon infection after tendon repair. 2 The patients underwent a 1-stage radical debridement followed by primary closure. All patients were immobilized for 2 weeks followed by application of a custom walking brace, only allowing plantar flexion for 4 weeks. At latest follow-up, 10 patients were able to perform single-limb heel raise, and 11 patients returned to their preinjury recreational activity. In our study, most patients rated their overall function as “normal” or “nearly normal” during the FAAM ADL scoring.
Our study has several limitations. Foremost, this is a retrospective review and is therefore subject to the weaknesses inherent to that particular study design. Because of this being a rare complication, there are a small number of patients and no control group was used. This is a study from a single institution and therefore is subject to referral bias. The FAAM scores were obtained by standardized phone survey. Because of the length of the study period, there were patients lost to follow-up and were unable to complete the FAAM ADL portion of the study. In addition, our study included multiple surgeons performing the procedures. The amount of tendon debrided was not clearly documented in several cases, making it difficult to know the amount of remaining Achilles tendon following the radical debridement procedure. In spite of these obvious limitations, we believe this study is important to help characterize the functional outcomes of patients who have undergone treatment for an infected Achilles tendon.
Conclusion
In conclusion, infections of the Achilles tendon following surgical repair or reconstruction are a devastating complication. All patients require a radical debridement of infected or necrotic tissue, and all foreign material such as retained sutures must be removed. This may require multiple surgical debridements and soft tissue reconstruction. Wound coverage is dependent on size of the defect following the debridement procedure. All patients should receive culture-specific antibiotics for a period of 3 to 6 weeks. If needed, tendon reconstruction can be considered after the infection has been cleared and the wound has healed. We found that satisfactory functional results can be attained after radical debridement and wound closure.
Supplemental Material
Supplemental Material, FAO846943-ICMJE - Outcomes Following Treatment of the Infected Achilles Tendon
Supplemental Material, FAO846943-ICMJE for Outcomes Following Treatment of the Infected Achilles Tendon by Mark W. Bowers, Norman S. Turner, Daniel B. Ryssman and Steven L. Moran in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.