
Abstract
Background:
Conflicting evidence exists regarding the optimal management of acute Achilles tendon ruptures. Operative repair is thought to afford patients a lower risk of rerupture, albeit at a higher overall risk of wound complications.
Methods:
A retrospective chart review of 369 consecutive patients undergoing open repair of acute Achilles tendon ruptures performed by a single foot and ankle fellowship-trained orthopedic surgeon was undertaken. Healing was classified as no complications, complications without prolonging treatment, complications requiring prolonged local treatment, and complications requiring operative intervention. A statistical analysis comparing the rates of complications in this cohort to that reported in the literature was conducted.
Results:
There were a total of 33 (8.94%) wound complications. Compared to the rates reported in the literature, no significant difference was detected (P = .3943; CI 6.24-12.33). However, when the complications not requiring additional treatment or prolonged care were excluded, only 9 wound complications (2.44%) were identified—a significantly lower complication rate than that reported in the literature (P < .0001; CI 1.12-4.58). There were only 2 (0.54%) major complications requiring operative intervention, also a significantly lower rate than in the literature (P < .0001; CI 0.067-1.94).
Conclusion:
In the past, wound-healing complications have been cited as a concern when treating patients operatively. We found that when solely looking at healing complications prolonging the patients’ overall recovery, a significantly lower rate of complications existed compared to that reported in the literature.
Level of Evidence:
Level IV.
Introduction
The overall incidence of acute Achilles tendon rupture has been steadily rising. A recent paper by Nyyssonen et al reported the incidence to have risen from 8.3 per 105 to 14.8 per 105 from 1987 to 1999. 22 The Achilles tendon is now the third most commonly injured tendon, with only the rotator cuff tendons and the knee extensor mechanism more frequently injured among major tendons.13,14 The most frequently affected group for acute Achilles tendon ruptures are male recreational athletes aged 30 to 49 years, with injury occurring during sports participation.4,10,12,17,21,25,28
Despite the relatively common occurrence of acute Achilles tendon ruptures, and the typically healthy patient population, the ideal treatment is still debated. 32 A number of recent meta-analyses have attempted to stratify treatment modalities based on rates of rerupture, clinical function, and overall complications.4,16,18 -21,31 The relatively small sample sizes and conflicting results between studies have resulted in an inability to establish clear guidelines for the treatment of acute Achilles tendon ruptures. 30 Jones et al conducted a Cochrane review and demonstrated that rerupture rates were lowest in patients who underwent operative management. They also showed an increased risk of complications in operatively managed patients albeit a high degree of heterogeneity existed in the pooled results. 8
Few studies have attempted to solely stratify wound complications after the operative treatment of Achilles tendon injuries. Bruggeman et al reported an overall complication rate of 10.4%, with deep infections occurring in 3% of patients. 3 Saxena et al reported similar complication rates of 10%, with 3.2% of patients requiring a second surgery to treat incisional complications. 27 These reports study a heterogeneous patient population with a number of presenting pathologies and varying physiologic states of well-being. We hypothesized that there would be fewer clinically significant wound complications than are reported in the literature in a cohort of Achilles tendon repairs performed by a single high-volume surgeon.
Materials and Methods
Study Design
After obtaining institutional review board approval, a retrospective case-series review was conducted identifying all patients who underwent Achilles tendon repair by Current Procedural Terminology (CPT) code 27650 from a patient database at the investigators’ institution. Only acute Achilles tendon ruptures treated by primary open repair were included in the study. Patients who were deemed to be at high risk for operative complications by the surgeon (peripheral vascular disease with evidence of venous stasis skin changes, poorly controlled diabetes [HbA1C > 7.5], morbid obesity with redundant skin about the ankle, and patients older than 60 who wished to attempt nonoperative treatment modalities) had been managed with nonoperative or percutaneous treatment and were excluded from the study.
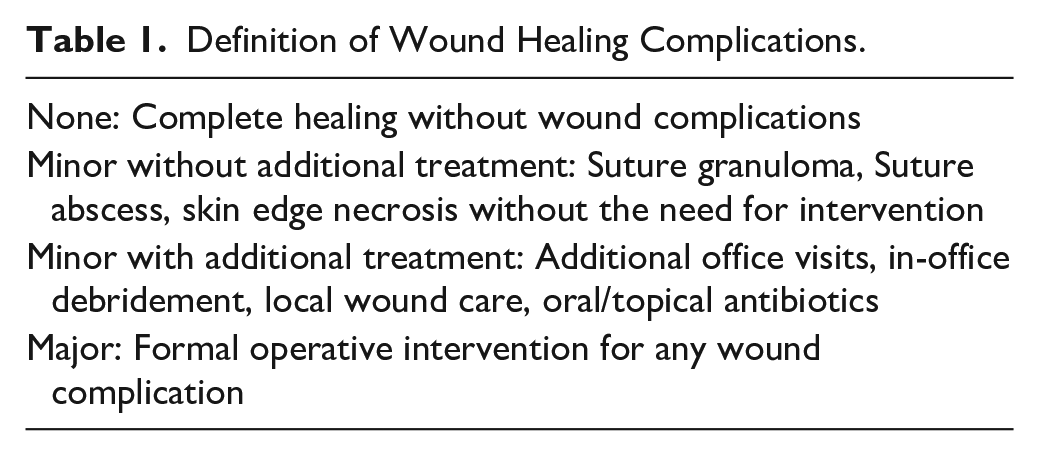
Clinical data from the electronic medical record were reviewed, including the preoperative assessment, operative report, and all postoperative evaluations until the patient was discharged from routine follow-up. Incision-healing complications were classified based on severity (Table 1). The strictest criteria were used so as to capture any patient in whom annotation was made regarding any abnormality noted with the incision, regardless of need for further treatment. Patient demographics were recorded for all patients (age, gender, BMI, tobacco use, diabetes, steroid use, time from injury to surgery, tourniquet time) and were used to identify potential risk factors for incision-healing complications. We additionally assessed if the wound class resulted in prolongation of treatment by delaying time to ambulation, time to starting physical therapy, time to boot discontinuation, or time to discharge.
Definition of Wound Healing Complications.
Operative Technique
A medial paratendinous approach, rather than a direct approach over the posterior aspect of the tendon, was used to minimize tension after closure. Initial incisions were full thickness through and included the fascia overlying the paratenon, The typical incision was 7 cm in length. Skin retraction was minimized, deep tissue retraction was used to limit tension on the skin itself, and only a small portion of tendon was exposed at a time. A midline deep posterior compartment fasciotomy was performed over the flexor hallucis longus muscle belly to decompress the fascia overlying the paratenon. After debridement of the tendon edges, a no. 2 FiberWire was used to run a multiloop Krackow 4-5-locking-knot stitch up the medial and down the lateral aspect of both the proximal and distal ends of the tendon. This was then tied at a resting tension comparable to the contralateral leg. A 2.0 Ethibond suture was then used in a running fashion circumferentially around the tendon repair to debulk the repair site. The fascia layer overlying the paratenon was then closed as a separate layer using a running zipper closure with a no. 0 Vicryl stitch to obtain a good “seal” over the repaired Achilles tendon. Meticulous subcutaneous and skin closure was performed using no. 2.0 Vicryl for subcutaneous closure and staples for skin.
Postoperatively, all patients were splinted in 20 degrees of equinus and made non-weight-bearing for 2 weeks. At 2 weeks, the splint was removed and the patient was placed in an Achilles boot with 3 wedges and allowed to begin weight bearing. One wedge was removed every 2 weeks and the patient was allowed to resume regular shoe wear 10 weeks after surgery. Physical therapy started at 6 weeks after surgery.
Literature Search
We conducted a literature review for all English-language articles assessing the operative management of Achilles tendon injuries. We only included studies that assessed wound complications following open treatment of acute Achilles tendon ruptures. Studies including repair of chronic Achilles tendon ruptures, and percutaneous repairs were not included. We utilized Ovid, Medline, the Cochrane registry of controlled clinical trials, and Google Scholar to identify all available studies. We identified papers in which a specific wound complication rate was reported and when the wound complications were stratified by severity.2,3
Statistical Analysis
All statistical analyses were performed using R: A Language and Environment for Statistical Computing (version 3.1.2, Vienna, Austria). A P value of .05 or less was considered statistically significant for all analyses. Multiple imputation of missing data and multivariate logistic regression were performed using the rms package within R. Simple pairwise comparison of proportions between experimental groups was performed using Fisher exact test, and continuous variables were compared using the Mann-Whitney test. The overall rate of incision-healing complications, the rate of incision-healing complications requiring in-office treatment, and the rate of incision-healing complications requiring operative intervention was compared to that reported in the literature using the binomial test. Based on our literature search, an overall wound complication rate of 10% was used for comparison.3,27
Results
We identified 369 consecutive open repairs of acute Achilles tendon rupture performed by a single foot and ankle fellowship-trained surgeon in a tertiary care setting between August 2000 and May 2014. The study population consisted of 314 males and 55 females. The average age was 41 (range, 20-74) years, and the average BMI was 27.9 (range, 18.6-42.8) (Table 2).
Patient Demographics. a

Multivariate logistic regression analysis was used to predict statistically significant patient factors associated with wound healing complications.
For minor wound issues not requiring additional treatment, there were a total of 33 (8.94%) wound complications identified (Table 3). Twenty-two of these were minor issues noted in the chart for which a single in-office intervention was required (such as debridement of a spitting Vicryl suture). When excluding this group and assessing only wounds that did require additional treatment, 9 wound complications (2.44%) were identified. Only 2 patients of 369 (0.54%) had complications requiring operative intervention.
Wound Complications.
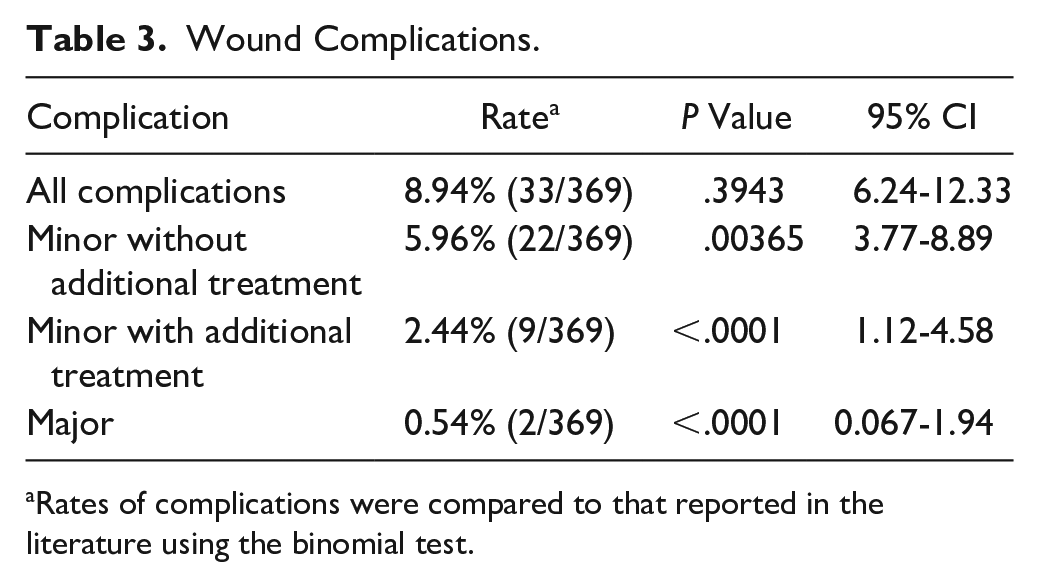
Rates of complications were compared to that reported in the literature using the binomial test.
The first patient was a 49-year-old otherwise healthy male with no known risk factors for delayed wound healing. He fell at home prior to his 6-week follow-up visit, leading to a dehiscence of a 1-cm × 1-cm area of his distal incision. He presented to the office 5 days after the incident. The patient was initially managed with local wound care and oral antibiotics, but subsequently developed purulent drainage. He was taken to the operating room for formal irrigation and debridement. Cultures grew pseudomonas and the patient was treated with 6 weeks of ciprofloxacin orally. The wound healed after 4 weeks, but rehabilitation and ambulation were delayed. The patient was discharged 42 weeks post injury without significant functional deficits.
The second patient was a 48-year-old man, without risk factors for wound healing. At his 2-week follow-up visit, he was noted to have a stitch abscess from a spitting Vicryl suture within the distal third of his incision. This was debrided in the office and local care and oral antibiotics initiated. He returned 1 week later with increasing erythema and purulent drainage and was taken for formal debridement in the operating room. Intraoperative cultures grew methicillin-sensitive Staphylococcus aureus (MSSA) and he was managed with 6 weeks of intravenous daptomycin because of a penicillin allergy. His wound subsequently healed with local wound care and he was discharged after 22 weeks without functional deficits. These 2 patients required significantly longer follow-up (32.3 weeks) than the average for the remaining cohort in the study of 14.2 weeks (P < .05).
The 22 patients with wound issues not requiring additional treatment and the 9 requiring local care and/or oral antibiotics, had an average delay in starting physical therapy of 10.5 days, and an average postoperative treatment duration of 16.1 weeks, which was not significantly longer than the average of the cohort without wound issues of 14.2 weeks (P = .127). Several types of wound complications presented, which included suture granulomas, skin edge necrosis, and blisters (Table 4).
Wound Complications by Type.

One additional patient suffered a major, but non-wound-related, complication during this time period requiring a return to the operating room. This was a 350-lb professional football player who fell onto his leg while out of his protective boot 3 weeks following his operative repair, sustaining a repeat rupture requiring additional operative repair. This was the only rerupture within this patient cohort.
There were no cases of sural nerve injury or clinically significant scar dysesthesia found within the study cohort. Fourteen patients (3.8%) were noted to have thickened keloid scars (all in African American patients), but none of these required additional treatment nor affected rehabilitation protocol or time to discharge.
Discussion
Concern for wound complications following operative repair of primary Achilles tendon ruptures is a major factor in the decision between operative and nonoperative treatment. Management of infections of the Achilles tendon is complex. The superficial nature of the Achilles tendon makes primary closure or the use of local small flaps difficult. Additionally, the anatomy of the distal third of the lower extremity, which includes the relatively avascular surface of the tendon where a clearly definable paratenon/fascia layer is not present, excessive soft tissue edema, and poor local perfusion, all contribute to poor wound healing potential.5,26 Treatments ranging from simple local wound care, antibiotics, negative pressure therapy, skin grafting, deep debridement, and flap coverage have all been utilized with varying degrees of success.6,9,26
Operative repair has generally been favored over nonoperative treatment in regard to rerupture rates,4,7,17,19,21 but postoperative complications other than rerupture have been reported to be as high as 34%.11,17 Studies have consistently found wound complication rates between 7% and 13%, with a deep infection rate of 2% to 5%.1,3,5,27 However, these studies often failed to define what constituted a wound complication and also failed to distinguish acute versus chronic rupture treatment. Additionally, although the pooled data collected in meta-analyses can overcome limitations with sample sizes with relatively uncommon outcomes, a disadvantage of these studies includes the heterogeneity of the individual papers used and the low number of patients treated by single surgeons.15,29 Furthermore, there has been consistent data from other areas of orthopedics that suggests higher-volume surgeons have fewer complications, which could be another potential factor in the lower rate of wound complications observed in this study. 2
Our study classified wound-healing complications into 4 groups based on severity in an attempt to define rates of clinically impactful wound issues. These groups included none, minor without any prolonged treatment, minor with prolonged in-office treatment, and major requiring a return to the operating room. Including even the minor wound issues not requiring additional treatment, we found an overall wound complication rate of 8.94%, which was comparable to the rates reported in the literature (P = .3943; CI 6.24-12.33). However, when only including clinically significant wound healing issues, only 2.44% of patients required additional in-office treatment with local wound care and either oral or topical antibiotics. When comparing this rate to the rates reported in the literature (∼10%), a statistically significant lower complication rate was detected (P < .0001; CI 1.12-4.58). Only 2 patients (0.54%) required a formal debridement in the operating room. When comparing our major complication rate to the deep infection rate reported in the literature (∼3%), our rate of 0.54% was also statistically significantly lower than previous reports (P = .001946; CI 0.067-1.94). The wound complications requiring treatment were significantly less than the composite wound complication rates reported in the literature. This suggests that clinically significant wound complications after primary acute Achilles tendon repair are not as prevalent as previously described.
A number of studies have further analyzed complications and outcomes of operative versus nonoperative treatment of acute Achilles tendon ruptures.* A meta-analysis by Jiang et al, which included 10 randomized controlled trials with 894 patients, found that operative repair was superior to nonoperative treatment with a lower risk of rerupture (P = .002) and a shorter time for sick leave (P = .009), but was inferior with respect to complication risks (26.60% [112/421] vs. 7.19% [31/431]). 7 When complications were subcategorized, they found a significantly higher complication rate in the operative group for scar adhesion, superficial infection, and sensibility disturbance. However, they found no difference between groups with regard to deep infection (P = .22). Conversely, a systematic review of 7 trials with 677 patients by Wilkins et al found a significantly higher incidence of deep infections for patients treated operatively (P = .0113). 30
Although nonoperative treatment avoids the risk of wound healing complications, there are other potential complications that are equally common. A study by Metz et al compared mini-open repair versus nonoperative treatment using functional bracing with immediate weightbearing for acute Achilles tendon ruptures. 17 They found skin-related complications (eg, fungal infections, pressure sores, superficial wound infection, scar adhesions, and blisters) to be higher in the nonoperative group, making up 42% (5/12) of operative complications and 62% (13/20) of nonoperative complications. This demonstrates that conservative casting or bracing poses a risk for skin complications as well.
The role of patient factors in influencing healing potential has been well documented.3,24,26,27 Pajala et al found age more than 60 years, tobacco use, corticosteroid therapy, diabetes, surgery delayed by more than 7 days, and the presence of pain in the tendon before the accident to be risk factors associated with wound healing issues. 24 Another study from Nyyssonen et al determined that surgery that is delayed by more than 15 days and an operative procedure involving tendon reconstruction significantly increased the risk of infection postoperatively. 23 Bruggeman et al found tobacco use, steroid use, and female sex to all be associated with wound complications. 3
We believe that the judicious selection of optimal operative candidates is likely related to our low overall rate of wound complications as well as the inability to detect a statistical significance in the positive predictive value of patient factors as they relate to wound complications. This study included only acute primary ruptures, suggesting an active study population. There were only 6 diabetics and 1 patient taking corticosteroids involved in the study. There were 34 (9.2%) tobacco users. Of all patient-specific factors related to the 33 patients with wound healing complications, only 2 from the minor without prolonged treatment group were tobacco users. The remaining 31 patients did not have any relevant risk factors, including history of diabetes, smoking, or corticosteroid use. Combined with careful patient selection prior to surgery for acute Achilles tendon ruptures, significant wound healing complications are rare.
Additionally, unlike Nyyssonen et al, 23 we did not find an association between timing of surgery and wound healing complications with our average time of repair (8.9 days post injury) not being significantly associated with wound issues (P = .21). In fact, the average time of surgery post injury for our 33 wound healing issues was 7.36 days, less than the cohort average, suggesting that proper patient selection and operative technique may be more important factors.
There are a number of limitations in this study. The retrospective nature of the study did not allow us to visualize the incisions with wound healing issues. However, the office notes for each of the patients specifically mention the incision and its level of healing at each office visit. There is also the possibility that patients with complications sought follow-up at an outside institution. This is a low possibility given that all patients were followed until they were able to be discharged from our practice with a return visit on an as-needed basis. Other than incision healing sequelae and length of postoperative treatment, no patient centered outcomes were measured for this study to determine the overall effect of the complications. There is also the chance that selection bias may influence our results as the majority of our population that was selected for operative management was without significant comorbidities.
In conclusion, these findings suggest that clinically significant wound healing issues (those that alter the standard postoperative course) after primary Achilles tendon repair are not as prevalent as previously described. Major wound complications, in particular, appear to be more infrequent than noted in the literature, with deep infections making up only a half percent within our patient population. This information can be used in counseling patients on operative versus nonoperative management for acute Achilles tendon ruptures.
Footnotes
This article was originally published as: Bishop ME, Comer CD, Kane JM, Maltenfort MG, Raikin SM. Open repair of acute Achilles tendon ruptures: is the incidence of clinically significant wound complications overestimated? Foot Ankle Orthop. 2017 Apr 7;2(2):2473011417699834. doi:10.1177/2473011417699834.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.