
Abstract
Extensive soft tissue defects of the ankle are an uncommon but challenging problem that require a combination of reconstructive options. We report the case of a complex injury involving the skin, lateral ankle ligaments, and peroneal tendons that were anatomically reconstructed. A 15-year-old girl was injured in an automobile accident resulting in extensive soft tissue defects and marked instability of her right ankle. The lower two-thirds of the anterior talofibular ligament (ATFL) had segmental defects, and calcaneofibular ligament (CFL) was completely torn, and both peroneal longus and brevis tendons were severely damaged. Initial debridement was performed on the day on injury. Two weeks after injury, the ATFL and CFL were reconstructed using a semitendinosus autograft and suture tape augmentation. Both peroneal tendons were reconstructed using a gracilis autograft. The skin defect (10 × 10 cm) was covered with an anterolateral thigh flap. After removing a short leg cast at 3 weeks postoperatively, the patient started range of motion exercises without using any brace. Weightbearing was allowed at 4 weeks. At the 24-month follow-up examination, she had returned to her preoperative level of work and sports activities.
Keywords
Introduction
The treatment of extensive soft tissue defects of the ankle resulting from high-energy trauma or tumor resection is challenging. 5,11,14 Tendons and ligaments are essential for normal movement and stability of the ankle, and loss of these tissues requires functional reconstruction. Anatomic reconstruction using a tissue graft to treat chronic lateral ankle instability or peroneus tendon injury has gained popularity and has favorable clinical results. 4,6 -8,13,15 However, reports of treatment for combined defects of lateral ankle ligaments and peroneal tendons are lacking. We report a case of complex defects of the lateral ankle ligaments and peroneal tendons that were anatomically reconstructed using semitendinosus and gracilis autografts.
Case Report
A 15-year-old girl who was hit by a bus was admitted to our hospital. Initial examination revealed extensive skin and soft tissue defects on the lateral side of her right ankle. The talus was visualized through the wound, and the ankle joint showed marked instability (Figure 1A). A comminuted fracture of the distal fibula was revealed by plain radiography and computed tomography (Figure 1B and C). Surgical debridement was performed under general anesthesia. The damaged skin area was resected, resulting in a 10×10-cm defect (Figure 2). A distal fibula bone fragment was resected. The upper one-third of the anterior talofibular ligament (ATFL) remained; however, the lower two-thirds of the ATFL and the calcaneofibular ligament (CFL) was shaven off and disappeared from the distal fibula, along with the lateral part of the capsule. The distal half of the inferior extensor retinaculum remained. The talocrural joint was lax during the stress test and anterior drawer stress test; there was no damage to the articular cartilage on either the tibial or the talar side. Both peroneus longus and brevis tendons were severely crushed with segmental tear, and were resected. Kirschner wires were inserted from the proximal tibia to the talus and calcaneus for temporary fixation (Figure 1D). The wound was covered with a VAC (V.A.C. GranuFoam; KCI, Lane Cove, New South Wales, Australia).

Findings during the initial examination. (A) Initial soft tissue loss was an extensive defect at the lateral side of the lower leg. (B and C) Plain radiography and computed tomography demonstrate a fracture of the distal fibula. (D) Temporary fixation was performed using Kirschner wires at the initial debridement.

Appearance of the wound after initial debridement. The damaged skin area was resected, resulting in a 10×10-cm defect. The tip of the fibula is shown (white line). Both peroneus longus and brevis tendons were severely damaged and resected. The distal stump of the peroneus tendon is indicated (arrow).
Thirteen days after the initial debridement, a second surgery was performed. Under general anesthesia, the patient was placed in the semilateral position and a thigh tourniquet (250 mmHg) was applied. The gracilis tendon and semitendinosus tendon were harvested using a tendon stripper. First, we reconstructed the ATFL and CFL using a semitendinosus graft. 6 Two parallel bone tunnels with a diameter of 3.5 mm were made at the footprints of the ATFL and CFL attachment sites of the distal fibula. The semitendinosus graft was passed through one bone tunnel in an anterior-to-posterior direction and through another tunnel in a posterior-to-anterior direction using a passing wire (Figure 3A and B). Another bone tunnel was made at the CFL footprint site in the calcaneus, and the distal end of the graft was inserted in the tunnel. Then, it was firmly fixed using a 4.75-mm interference screw (PEEK SwiveLock C; Arthrex Inc, Naples, FL). Additionally, a suture anchor (3.5 mm; Corkscrew FT; Arthrex Inc) was placed at the CFL footprint site of the calcaneus to reinforce the attachment site of the reconstructed CFL. Then, two perpendicular bone tunnels, merging in the talar neck, were made at the anterior border of the talar body. The proximal portion of the graft (ATFL) was passed through the tunnels, posteriorly to anteriorly, and then overlaid on itself (Figure 3B). With the ankle in 0 degrees of dorsiflexion and slight eversion, the proximal end of the graft was sutured on itself using nonabsorbable No. 2 FiberWire (Arthrex Inc.). After suturing the remnant of the ATFL on the graft, suture tape augmentation (InternalBrace; Arthrex Inc.) was performed. A 3.4-mm tunnel was made in the distal fibula, superior to the ATFL insertion, followed by 4.75 mm of tape. Another 3.4-mm tunnel was made in the talar neck, slightly distal to the graft tunnel. With the ankle in a neutral position, 3.5- and 4.75-mm suture anchors (PEEK SwiveLock; Arthrex Inc.) were loaded with suture tape (FiberTape; Arthrex Inc.) overlaying the reconstructed ATFL. To avoid overtensioning, a small hemostat was placed underneath the suture tape when inserting suture anchors. The inferior extensor retinaculum was then mobilized proximally and sutured onto the remaining fibular periosteum and ATFL with 3-0 Vicryl. Stability of the ankle was confirmed using anterior drawer and talar tilt tests. After reconstruction, the range of motion was maintained (dorsiflexion, 10 degrees; plantarflexion, 40 degrees).
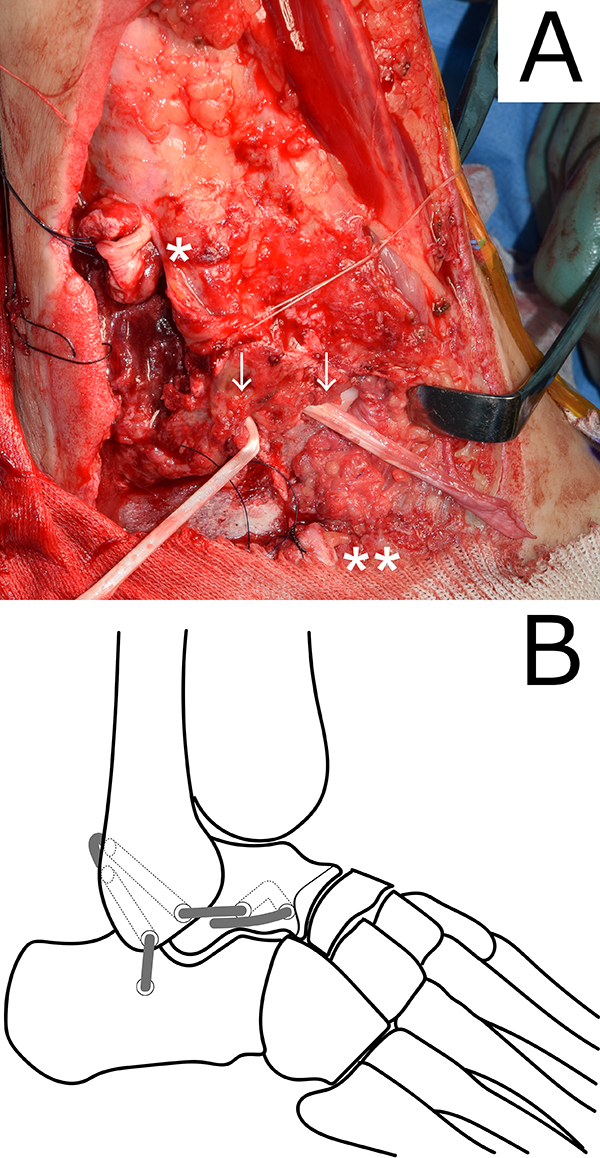
Reconstruction of lateral ankle ligaments. (A) Two bone tunnels were made on the distal fibula, and the semitendinosus tendon graft (arrows) was passed through the tunnels. The proximal (*) and distal (**) stumps of the peroneus tendons are indicated. (B) Schematic diagram of anterior talofibular ligament and calcaneofibular ligament reconstruction using the semitendinosus tendon graft.
Then, we reconstructed both the peroneus longus and brevis tendons. Two gracilis tendon grafts were prepared, and the proximal stumps of the peroneus tendons were sutured to the grafts with 3-0 Prolene using a Pulvertaft weave. While maintaining the foot in a neutral position, additional Pulvertaft weave suturing was performed between the distal stumps and grafts (Figure 4). The peroneal tendon sheath was repaired, and normal excursion of both peroneal tendons was confirmed. Finally, an 8×20-cm anterolateral thigh flap was harvested as a fasciocutaneous flap with subcutaneous perforators. The perforators were connected with anterior tibial vessels, and the wound was closed (Figure 5).

Reconstruction of both peroneal tendons. Both the peroneus longus and brevis tendons were reconstructed using gracilis tendon grafts. The superior peroneal retinaculum was repaired (arrowhead) to prevent dislocation of the tendons. The bone tunnel on the calcaneus for calcaneofibular ligament reconstruction is shown (*). The arrow indicates suture tape augmentation overlaying a reconstructed anterior talofibular ligament.

Coverage of the wound with the anterolateral thigh flap at 5 months after surgery.
Postoperatively, the patient was fitted with a short leg splint. After 3 weeks, the splint was removed, and the ankle was completely free of immobilization, without any brace used. Physical therapy including proprioceptive training and active range of motion training was started. At 4 weeks, full weightbearing was permitted, and the patient returned to school. At final follow-up, two years after surgery, the patient returned to her preoperative level of work and sports activities, with no pain, no instability, and no loss of range of motion in her right ankle.
Discussion
Various reconstructive procedures are available for the treatment of extensive soft tissue injuries of the ankle. 5,11,14 Depending on the extent of the remaining normal tissue, surgeons should choose the most appropriate procedures. To achieve full functional recovery, it is important to stabilize the ankle without limiting the range of motion. In this case, we chose to perform anatomic reconstruction for both lateral ankle ligaments and peroneus tendons because of the risk of ankle instability and hindfoot imbalance.
Although anatomic reconstruction of both the ATFL and CFL with a semitendinosus allograft reportedly leads to successful clinical outcomes for patients with chronic ankle instability, there is concern about the initial stability and the risk of reinjury. 4,6 Suture tape augmentation demonstrated 50% higher strength compared with the native ATFL in a cadaveric study; therefore, re-rupture of the reconstructed ligament before healing could be avoided in case of a sudden postoperative re-injury. 2 To enhance the initial stability, we also performed suture tape augmentation. 16 Suture tape augmentation of the ATFL also allows early postoperative mobilization of the ankle, which is advantageous to the recovery of the reconstructed peroneal tendons. Because overtightening of the tape can cause an inversion deficit, the ankle should be in a neutral position when tape augmentation is performed. 16
Injuries of both the peroneus longus and brevis tendons are uncommon, and only a few case series have been reported. 10,12,13,15 Chronic rupture of both peroneal tendons has been reconstructed using a Hunter rod with flexor hallucis longus tendon or tensor fascia lata. 13,15 Tendon graft or tendon transfer has been suggested when both the longus and brevis tendons are nonfunctional. 10 Thus far, only two cases of reconstruction of both tendons using a tendon graft with satisfactory results have been reported. 7,8 Reconstruction of peroneal longus tendon using a tendon graft with peroneal brevis-to-longus tenodesis may be a treatment option in the present situation. Using a cadaver model, tendon graft reconstruction has been reported to restore normal peroneus brevis tension; however, tenodesis of the peroneus longus tendon has not. 9 We chose to reconstruct both peroneus longus and brevis tendons and aimed to minimize potential alterations in hindfoot balance.
Various graft choices have been reported for tissue augmentation, including autografts and allografts. 3,4,8,13,15 Because allografts are not available in Japan, both semitendinosus and gracilis tendons were harvested. Although there is concern about donor site morbidity, few differences have been reported in the recovery of hamstring strength regardless of whether one hamstring tendon or two hamstring tendons were harvested. 1 Our patient showed good recovery of ankle function without any donor site pain or dysfunction.
Conclusion
We report a case of a complex injury involving the skin, lateral ankle ligaments, and peroneal tendons, which was anatomically reconstructed. At the 24-month follow-up examination, the patient had returned to her preoperative level of work and sports activities, with no instability or loss of range of motion in her right ankle. The ATFL and CFL were reconstructed by semitendinosus autograft and suture tape augmentation, which enhanced the initial stability and accelerated early rehabilitation. Both peroneal tendons were reconstructed using a gracilis autograft, successfully avoiding alterations in hindfoot balance.
Supplemental Material
Supplemental Material, FAO794677-ICMJE - Anatomic Reconstruction of Lateral Ankle Ligaments and Both Peroneus Tendons After Open Fracture Dislocation of the Ankle: A Case Report
Supplemental Material, FAO794677-ICMJE for Anatomic Reconstruction of Lateral Ankle Ligaments and Both Peroneus Tendons After Open Fracture Dislocation of the Ankle: A Case Report by Ryuta Sakurai, Jun-ichi Fukushi, Hideki Mizu-uchi, Masuo Hanada, Kenta Momii, and Yasuharu Nakashima in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This study was supported by Japan Society for the Promotion of Science KAKENHI (grant number: 26462301).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.