
Abstract
Gelatinous transformation of bone marrow (GTBM) is a complication of various diseases, one of which is anorexia nervosa (AN). We describe a rare case of a 20-year-old man who presented to our clinic with a 3-month history of heel pain without trauma. At presentation, he was noted to have a low body mass index (BMI) of 16.2 kg/m2 and pancytopenia. On magnetic resonance imaging, the left calcaneus showed low intensity on T1-weighted and high intensity on T2-weighted images. Open biopsy was done because we suspected that the lesion was either a lymphoproliferative tumor or a trabecular-type bone metastatic tumor. However, tissue histology of bone samples showed atrophy of fat cells with deposition of gelatinous material and a decreased hematopoietic cell population. Therefore, we made a diagnosis of GTBM, most likely caused by AN. We started treatment with nutritional support, and 6 months later, the hematological parameters returned to normal and BMI improved to 19.4 kg/m2. He was able to return to work and had no left heel pain. This case indicates that foot and ankle surgeons need to be aware of this rare pathology, although it might be difficult to diagnose without biopsy. To our knowledge, very few descriptions of GTBM in the calcaneus have been reported to date.
Gelatinous transformation of bone marrow (GTBM), also referred to as serous fat atrophy of bone marrow, is associated with several underlying conditions, particularly eating disorders such as anorexia nervosa (AN), and other causes of malnutrition or malabsorption such as chronic infection, cachexia from malignant tumors, chronic heart failure, chronic kidney disease, alcoholism, and cytotoxic drugs. 6,9,11,13,14 GTBM is characterized by fat cell atrophy, focal loss of hematopoietic cells with hypocellularity, and deposition of extracellular gelatinous material, which is composed of hyaluronic acid–rich mucopolysaccharide. 2,5
AN is defined as an eating disorder thought to be of psychogenic origin. AN is characterized by an intense fear of gaining weight, a distorted body image, and a refusal to maintain a normal body weight. 1 AN is often associated with hematological abnormalities ranging from mild anemia to severe pancytopenia. 7 About 20% of cases of GTBM may be related to anorexia nervosa or other malnutritional states. 2 In the lower limbs, GTBM is most often found in the distal phalanx of the first toe. 18 However, there have been few reports of GTBM in the calcaneus. 3,17,18
We present a rare case of a 20-year-old man diagnosed with AN who presented with pancytopenia and heel pain due to a GTBM in the calcaneus. An open biopsy was required for definitive diagnosis because it was suspected that the lesion could represent a malignant tumor based on magnetic resonance imaging (MRI) findings. Biopsy results were suggestive of GTBM, which was confirmed by the reversibility of the condition after nutrition support. The patient provided written informed consent for this report to be published.
Case Report
A 20-year-old man, who worked as a helper of seniors, had been noted to have chronic anemia at regular health checkups at his workplace for several years. He visited a local doctor with atraumatic left heel pain when weightbearing for approximately 3 months. Magnetic resonance imaging (MRI) of the left calcaneus showed abnormal intensity change like a kind of tumors, and so he was referred to our university hospital for further examination. Our initial physical examination revealed tenderness over the left calcaneus, with no swelling, warmth, redness, or limitation of movement of the ankle or subtalar joints. The patient took various types of tranquilizers (such as etizolam, alprazolam, diazepam, clonazepam), smoked approximately 40 cigarettes a day, and drank approximately 2500 mL beer a day. He was very fussy with food and often skipped meals because he was afraid of gaining weight. He weighed 52 kg, which at a height of 1.79 m meant that his body mass index (BMI) was 16.2 kg/m2, which is below the normal range.
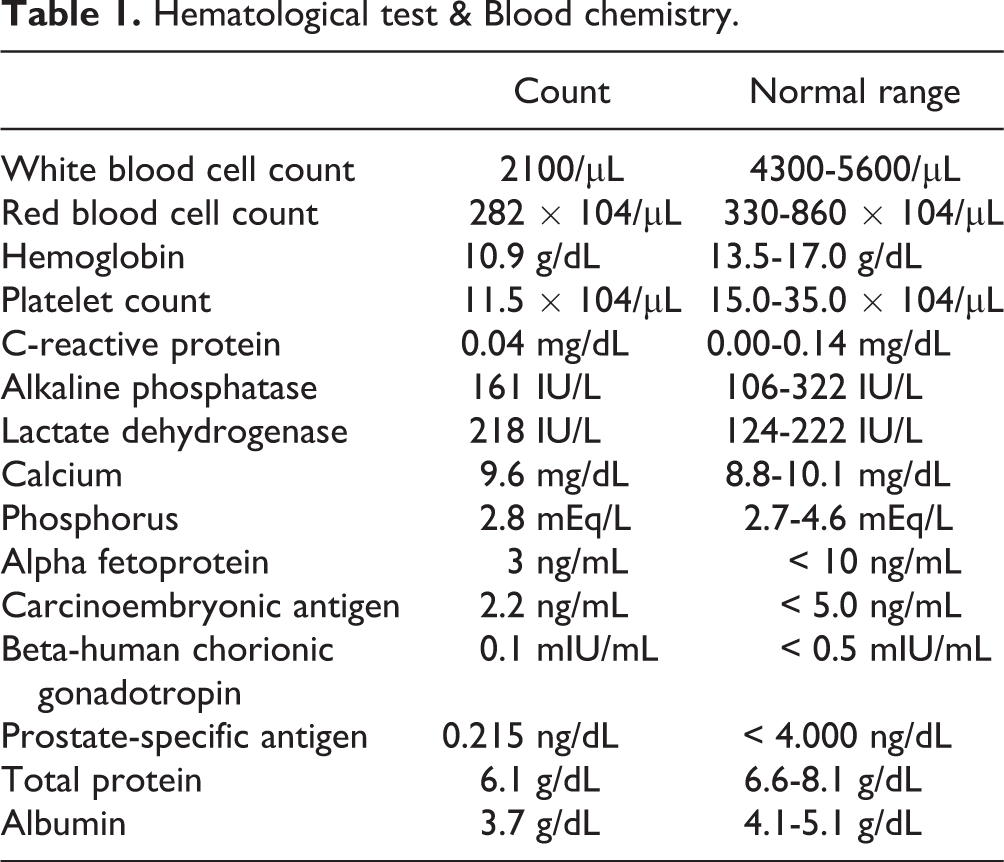
Hematological tests showed pancytopenia (Table 1). X-ray and computed tomography (CT) showed no evidence of destruction of the trabeculae in the left calcaneus (Figure 1 and Figure 2A,B). However, on MRI, the middle to posterior part of the left calcaneus showed low intensity in T1-weighted image, high intensity in T2-weighted image, and high intensity in short-TI inversion recovery (Figure 3A-C). Taking all clinical physical findings into consideration, we suspected that the lesion of the left calcaneus was either a lymphoproliferative tumor, such as leukemia, multiple myeloma, or lymphoma, or a trabecular type bone metastatic tumor, such as small cell carcinoma.
Hematological test & Blood chemistry.

Lateral x-ray shows no trabecular bone destruction.
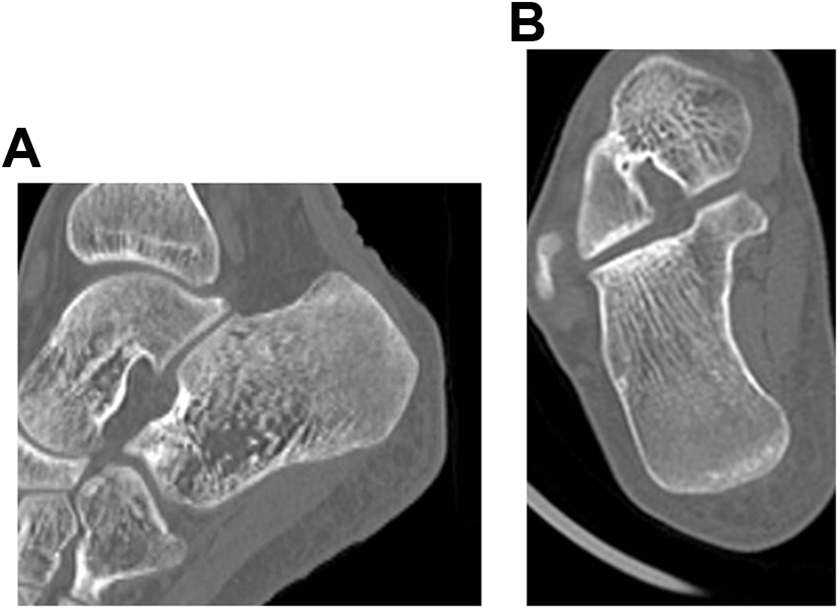
Sagittal (A) and coronal (B) computed tomography images showing no trabecular bone destruction.
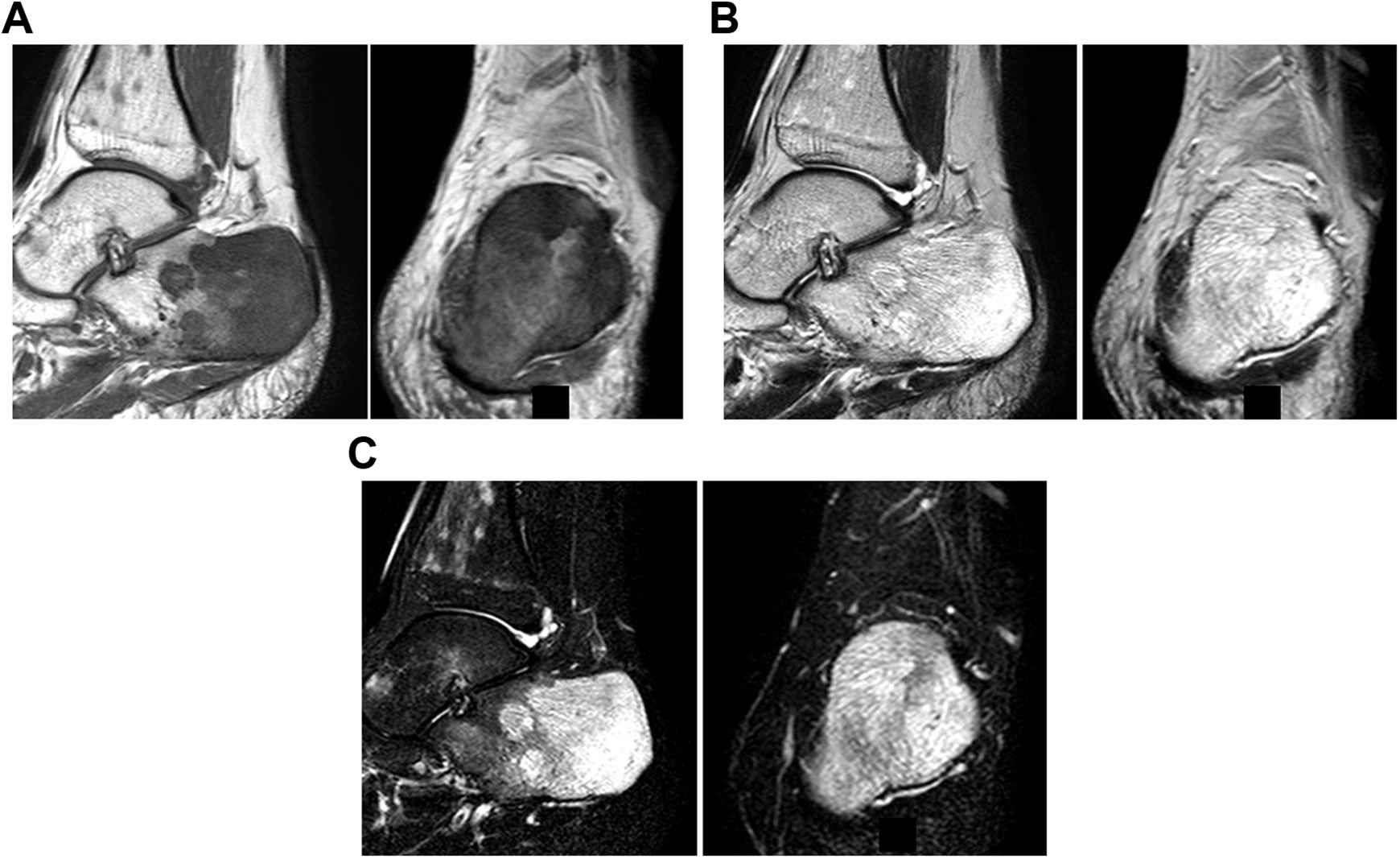
Magnetic resonance images of the left calcaneus, (A) sagittal or coronal T1-weighted images demonstrating abnormal hypointense signal of the visualized bone marrow. (B) Sagittal or coronal T2-weighted images demonstrating abnormal hyperintense signal of the visualized bone marrow. (C) Sagittal or coronal short-TI inversion recovery images demonstrating abnormal hyperintense signal of the visualized bone marrow.
He was admitted to our hospital for surgery, and we performed an open biopsy via a lateral approach to obtain sufficient calcaneal bone for histological examination. Surprisingly, histological findings showed hypocellularity associated with accumulation of a gelatinous extracellular matrix in the bone marrow and a marked reduction of hematopoietic cells with no destruction of bone trabeculae (Figure 4). These features were consistent with GTBM. Considering these histological and physical findings combined with the history, we made a formal diagnosis of GTBM caused by an eating disorder, specifically, malnutrition associated with AN, based on a psychiatric evaluation.
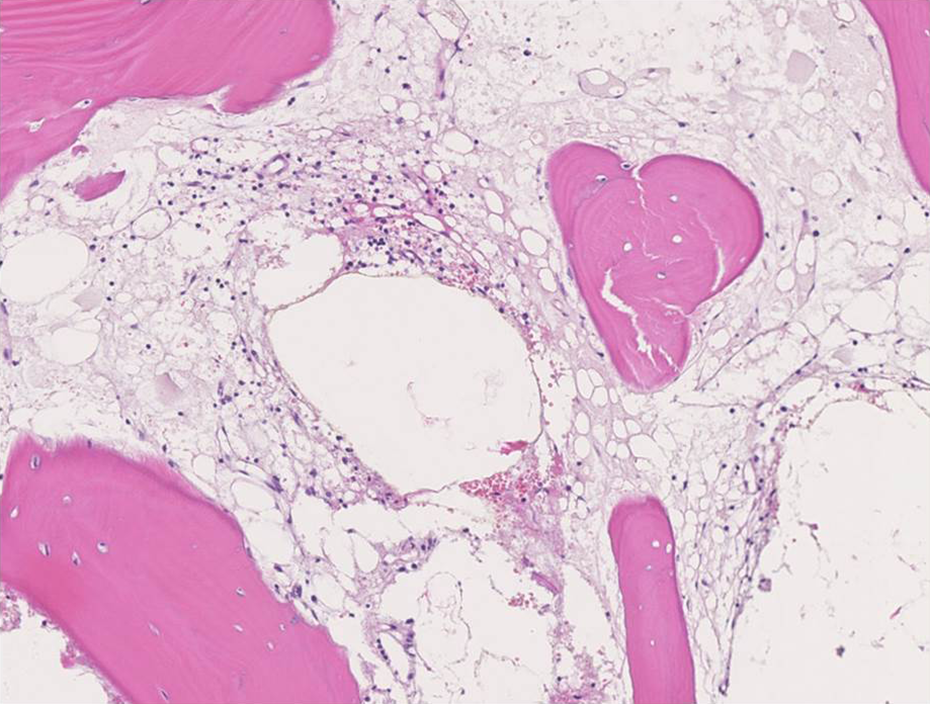
Hematoxylin-eosin stain image of the calcaneus obtained by open bone biopsy. Infiltration by gelatinous substance, fat atrophy, and marrow hypocellularity. These features are consistent with gelatinous transformation of bone marrow.
The patient recovered and was discharged, and we immediately referred him to a metabolic physician at our hospital. The physician provided nutrition support for him. Caloric intake increased to approximately 2000 calories/d. Moreover, his habit of smoking cigarettes per day decreased to approximately 10 and beer consumption per day fell to approximately 400 mL. After 6 months of sufficient nutrition, the pancytopenia had resolved. Moreover, he weighed 62 kg and was in apparent good health. The left heel pain had disappeared, and he returned to work. At the 1-year follow-up visit, the patient had remained asymptomatic without recurrence.
Discussion
This report details the presentation of a 20-year-old man with histologically confirmed GTBM in the calcaneus in the setting of underlying AN. According to Tavassoli et al 16 and Lambert et al, 10 this transformation occurs following a paradoxical increase in the fat fraction of the bone marrow due to an increase in the number of adipocytes as hematopoietic tissue disappears early in weight loss. Subsequently, marrow-fat stores are used for catabolic activity, and adipose tissue then collapses and is replaced by gelatinous material as seen in GTBM.
One study reported that GTBM was observed in 30 (79%) distal phalanges of the first toe, 26 (68%) proximal phalanges, 23 (61%) first metatarsal bones, 16 (42%) first cuneiforms, 14 (37%) tarsal navicular bones, 23 (61%) talus bones, 18 (47%) tibias, and 12 (32%) femurs in all GTBMs. 18 However, GTBM in the calcaneus was very rare. To our knowledge, there have been 6 cases in 3 studies reporting GTBM in the calcaneus to date (Table 2). 3,17,18
Reported Cases of GTBM in the Calcaneus in the Literature.
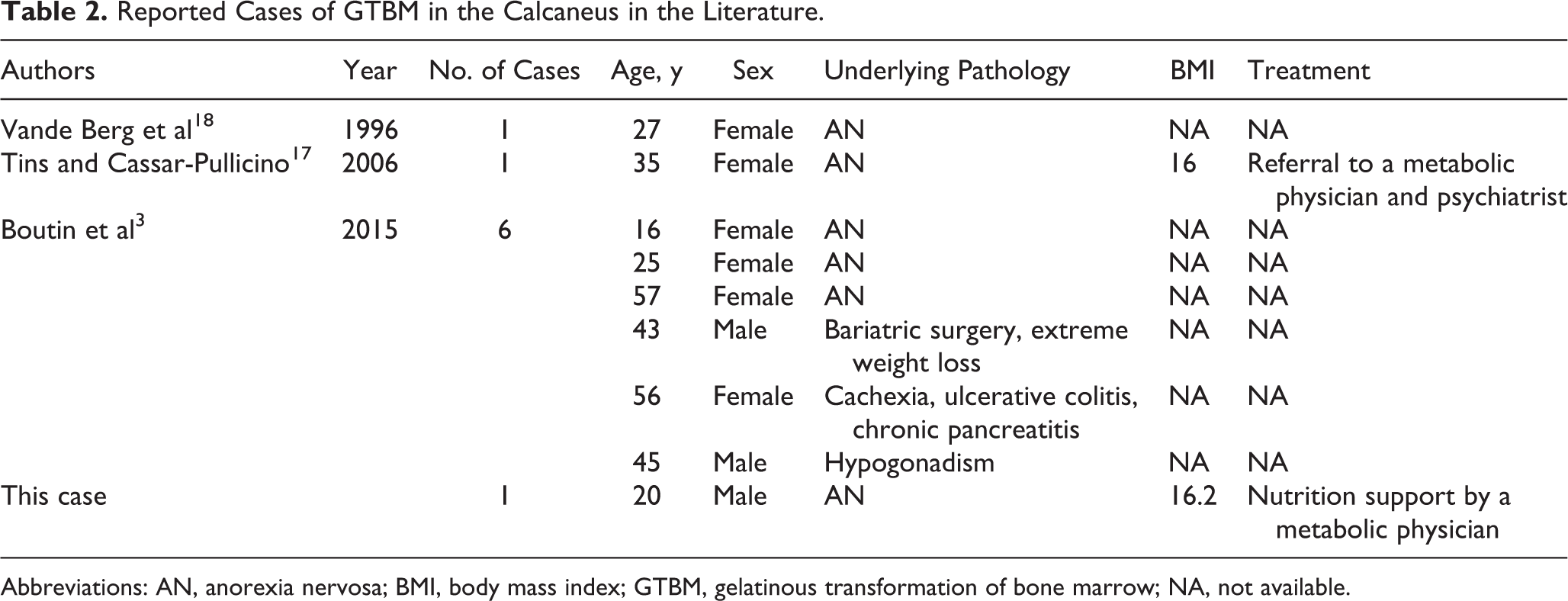
Abbreviations: AN, anorexia nervosa; BMI, body mass index; GTBM, gelatinous transformation of bone marrow; NA, not available.
MRI of the affected calcaneus of this present case showed low signal intensity signal on T1-weighted and high signal intensity on T2-weighted images. Similarly, lymphoproliferative tumors, such as leukemia, multiple myeloma, and lymphoma, ordinarily show low signal intensity in bone marrow on T1-weighted and high signal intensity in bone marrow images. 8 Metastases of some tumors, such as small cell carcinoma, which grow between trabeculae within marrow without causing gross trabecular or cortical destruction, also typically show low signal intensity on T1-weighted and high signal intensity on T2-weighted images in bone marrow images. 8 Because these findings were consistent with this case, open biopsy could not be avoided to distinguish GTBM from lymphoproliferative tumors or trabecular-type bone. It is important for foot and ankle surgeons to be aware of GTBM as a possibility in the differential diagnosis when they encounter patients with AN and these MRI findings in the calcaneus.
Treatment for GTBM is based on treating the underlying disease. However, treatment is primarily improvement of the patient’s state of malnutrition by nutritional support if AN is present. 4 There was a report that the recovery of neutropenia in AN with GTBM was obtained with granulocyte -colony-stimulating factor (G-CSF) to stimulate proliferation of granulocytic precursors. 12 In our case, the improvement of the patient’s health and condition was obtained without the need for G-CSF. The nutritional support was sufficient, and the improvement of patient’s health condition was reversible with appropriate food intake. 15 However, careful follow-up is necessary because the natural history of AN includes frequent relapse, 4 and AN will often require psychiatric treatment, especially when it is recalcitrant.
One limitation of this report is the short follow-up period. Although his symptoms have not recurred as of the latest follow-up visit 1 year after surgery, further follow-up is necessary. Furthermore, it is difficult to differentiate whether the GTBM was secondary to AN or malnourishment that was related to alcoholism. Also, it is possible that his heel pain came from an insufficiency fracture of the calcaneus whose bone marrow changes on MRI may have been masked by the GTBM.
In conclusion, we report the rare case of a 20-year-old man with GTBM in the calcaneus and AN who was successfully treated with nutritional support. Foot and ankle surgeons should be aware of this rare pathology, although it might be difficult to distinguish from some tumors on MRI, and therefore biopsy may be necessary even if this diagnosis is suspected.
Supplemental Material
Supplemental Material, FAO780325-ICMJE - Gelatinous Transformation of Bone Marrow in the Calcaneus, Diagnosed by Open Bone Biopsy in a Patient With Anorexia Nervosa
Supplemental Material, FAO780325-ICMJE for Gelatinous Transformation of Bone Marrow in the Calcaneus, Diagnosed by Open Bone Biopsy in a Patient With Anorexia Nervosa by Ichiro Tonogai, Daiki Nakajima, Ryo Miyagi, and Koichi Sairyo in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.