
Abstract
Background:
Bone marrow aspirate (BMA) is used with the putative goal of enhancing healing of injured tissue. The most common sites to harvest BMA are the iliac crest, the tibia, and the calcaneus. Investigators have found that the tibia and calcaneus have fewer progenitor cells than the iliac crest. This retrospective review evaluates the efficacy and safety profile of harvesting BMA from the calcaneus bone. We hypothesized that harvesting BMA from the calcaneus will have high efficacy and safety profile with low complication rates.
Methods:
A retrospective chart review of patients undergoing bone marrow aspiration from the calcaneus bone from January 2019 to October 2022 was performed. The main data points evaluated were patient satisfaction and pain level, follow-up times, quantity of BMA harvested, fusion rates, and complications including nerve damage, infections, and nonunions.
Results:
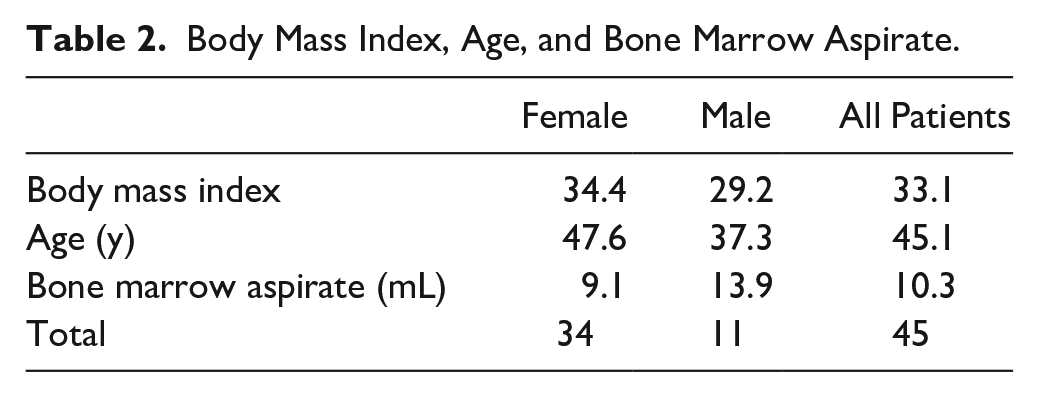
There were 45 (34 female and 11 male) patients who underwent 45 procedures. The average age, BMI, and amount of BMA were 45.1 years (range 23-79), 33.1 (range 19.2-61.3), and 10.3 mL (range 2-40), respectively. There was no pain reported at the final follow-up in 32 patients (71.1%), and there was minimal to no pain in the area of surgery in the remaining 13 patients (28.9%). The 10 cases of fusion successfully healed with combined use of allograft and BMA. The average follow-up time was 12.3 months (range 2.4-33.7). There were no infections, wound complications, or nerve injuries.
Conclusion:
Harvesting BMA from the calcaneus bone is a safe procedure. In this heterogenous series where BMA augmented other surgical strategies, patients had little to no pain and there were no cases of wound complication or iatrogenic neuropraxia after undergoing bone marrow harvest from the calcaneus.
Level of Evidence:
Level IV, case series.
Introduction
Bone marrow aspirate (BMA) is often used with the putative goal of enhancing healing in foot and ankle surgery. It is commonly used in osteochondritis dissecans repair, fusions, and nonunions. 2 Common sources of BMA include the iliac crest, distal tibia, and calcaneus with literature primarily supporting aspiration at the iliac crest because it has been reported to possess the largest number of osteoprogenitor cells.5,6,11 The tibia and calcaneus bones are also used; however, fewer osteoprogenitor cells have been found at these sites. 10
The current literature is not abundant regarding whether the calcaneus is a suitable harvest site for BMA in terms of a variety of outcomes of interest. In particular, there are limited data in the literature evaluating complication rates, patient satisfaction, amount of BMA harvested, and successful surgical outcomes with the use of BMA from the calcaneus. In foot and ankle surgery, harvesting BMA from the calcaneus may prove to be a more convenient site than the iliac crest because it can easily be included in the sterile field and thus allow the procedure to be performed as an adjunct during patients’ primary foot and ankle procedure.7,8 Patients from the study by Raikin et al 13 reported higher satisfaction as well as significantly lower pain after surgery when the tibia or calcaneus was used for harvest BMA instead of the iliac crest. The study by Baumhauer et al 3 evaluated pain levels at different sites for open autologous bone harvesting including the iliac crest, calcaneus, and tibia. They measured pain levels based on different time periods and the only clinically significant result was higher levels of pain at week 3 for the iliac crest group vs the calcaneus and proximal tibia groups. 3 The amount of BMA harvested in multiple sites showed no major differences when comparing the tibia, iliac crest and calcaneus. 3 Studies have showed that the calcaneus site for BMA is associated with high efficacy, low complication profile, and a safe site for BMA harvest.3,13 At our institution, we primarily use calcaneus BMA because of its ease of use in the surgical field and its low complication rate.
The purpose of this study was to document patient outcomes, complication rates, amount harvested, and surgical outcomes including revision rates with the use of calcaneal-derived BMA as a surgical augment for healing. We hypothesize that using the calcaneus for harvest produces adequate amounts of BMA and favorable patient satisfaction and pain reduction, low complication rates, and low pain scores.
Methods
Data of patients who underwent BMA from the calcaneus between January 2019 and October 2022 by a single surgeon were retrospectively collected in this institutional review board–approved study. Inclusion criteria involved patients older than 18 years old undergoing foot and ankle surgery during the study period with a minimum follow-up of 2 months. Exclusion criteria involved patients <18 years old and undergoing surgery outside of the time range of the study. The harvesting of BMA from the calcaneus and the usage in patients was selected per the surgeon’s preference. The main data points evaluated were patient-reported satisfaction and pain level, follow-up times, amount of BMA harvested, fusion rate, and complications including nerve damage, infections, and nonunion. Fusion and nonunion rates were evaluated using radiographic images and clinical analysis.
In this study, BMA harvest from the calcaneus was performed as previously described in accordance with the standard operative procedures. 15 There were no secondary sites for harvesting BMA and all were unilateral. BMA was harvested from the lateral calcaneus with a BMA kit (Stryker, Kalamazoo, MI). A 10-mL syringe was used to improve the generation of mesenchymal stem cell (MSC) harvest. 9 In the few cases where less than 5 mL of BMA were obtained, no extra attempts to harvest BMA were performed. Most patients received BMA mixed with one of the 3 allograft options: BIO (Stryker, Kalamazoo, MI), 4 DBM (Ignite; Wright Medical Group, Memphis, TN), and BioCartilage (Arthrex, Naples, FL).
Surgical Procedures and Allograft Usage
BMA was used in arthroscopic osteochondral dissecans (OCD) repair in 3 ways. For lesions less than 1 × 1 cm, after microfracture was performed the BMA was injected into the ankle joint and then the portals were closed. If the lesion was greater than 1 × 1 cm but less than 5 mm deep then the OCD was augmented with allograft cartilage extracellular matrix (BioCartilage; Arthrex, Naples, FL). The BMA was mixed with the BioCartilage (Arthrex, Naples, FL) and then placed in the defect, and fibrin glue was used to secure the repair. If the lesion was greater than 1 × 1 cm and the depth was greater than 5 mm, the OCD was augmented with BioCartilage (Arthrex, Naples, FL) and allograft bone (AlloSync; Arthrex, Naples, FL) The defect was first filled with the bone graft (AlloSync; Arthrex, Naples, FL); then the BMA was mixed with the BioCartilage (Arthrex, Naples, FL) and then placed in the defect on top of the bone graft, and fibrin glue was used to secure the repair.
BMA was used in most fifth metatarsal repairs (9 of 10). Prior to insertion of the Jones fracture screw, BMA was mixed with demineralized bone matrix (Ignite; Wright Medical Group, Memphis, TN). This was then injected into the medullary canal of the fifth metatarsal and the Jones fracture screw was then placed. For the navicular chronic stress fracture nonunion, the BMA was mixed with allograft bone (Bio4; Stryker, Kalamazoo, MI) and placed in the defect prior to hardware placement. BMA was not concentrated during this preparation process.
All tendon cases that used BMA were for surgical repair of non-insertional Achilles tendinopathy. A 2-cm incision was made over the area of tendinopathy. The tendon was longitudinally spilt and debrided, and a gastrocnemius recession was performed through a separate proximal incision. The tendon was then repaired back together, and BMA was injected into the repair site. The usage and type of allografts as well as the type of surgery are in Table 1.
Type of Surgery and Allograft.

Abbreviations: AlloSync, AlloSync Arthrex; Bio cartilage, BIO Stryker; DBM, Ignite Wright Medical Group NV; MTP, metatarsophalangeal; OCD, osteochondral dissecans; ORIF, open reduction internal fixation.
Results
Forty-five patients (34 female, 11 male) underwent calcaneus BMA harvest during their surgical procedures (28 right and 17 left foot; Table 2). Among all patients, 14 reported being tobacco users. All the patients underwent their procedures on an outpatient basis and the surgeries performed are in Table 3. The average follow-up time was 12.3 months (range 2.4-33.7). There were no infections, nerve injuries, or wound complications at the harvest site among all patients. Fusion rate was evaluated using radiographic images and clinical evaluation. Pain scores reported by patients revealed that 32 patients (71.1%) had no pain after surgery and 13 patients (28.9%) reported little to no pain after surgery. All patients reported satisfaction with their surgery. All 10 arthrodesis cases healed.
Body Mass Index, Age, and Bone Marrow Aspirate.
Surgeries Performed.

Discussion
BMA is being utilized in foot and ankle surgery with the intent to improve surgical outcomes. In this single-surgeon retrospective review, we analyzed its clinical utility to supplement several foot and ankle procedures. 8 Our study shows strong results including high satisfaction rates, minimal to no pain levels around the surgical area, and no cases of wound and nerve complications. All patients who had fusions successfully fused when mixed with BMA and allograft. Previous studies found that injection of BMA in patients with tibial nonunion resulted in a union rate of 89%. 9 In a case series of patients with tibial nonunion undergoing autologous bone marrow, 82% of patients had union at 6 months, and 66% of this group had improvement in pain intensity and more than 5 years of improvement in quality-adjusted life years. 4
Risks and complications from harvesting BMA must be considered when performing the procedure. This study had no patients with wound complications or fractures at the location of the BMA harvest at final follow up. Our study had no patients with nerve injuries, infections, or wound complications around the incision area. In a review including 63 hospitals with more than 19 000 procedures in the United Kingdom involving open biopsy of the iliac crest, the adverse event rate was 0.08%. 1 In a more recent review including bone marrow aspiration of the iliac crest from 2017 to 2019, 9 of 233 patients (0.4%) suffered from procedural complications. 12 Roukis et al 14 conducted a multisite observational cohort that reported no nerve injury, infections, or fractures on 548 procedures of bone marrow aspiration below the knee.
Patient outcomes are an essential factor to consider when deciding which site to use for harvesting BMA. Daigre et al 7 prospectively studied 40 patients who underwent bone marrow aspiration from the calcaneus bone and found that on average over a 12-week follow-up period, mean visual analog scale (VAS) pain scores were significantly higher in the calcaneus compared with the distal tibia or iliac crest. However, this same study indicated that the increased pain scores found in the calcaneus group was likely confounded by a high number of hindfoot/ankle surgeries performed in the ipsilateral foot. 7 Baumhauer et al reported that among their cohort of open autologous bone marrow harvests, the worse and longest-lasting pain at 52 weeks was at the calcaneus site. This reflected 20% of their calcaneus site group. 3 The results from our study showed data very different from the previous studies, with 71.1% of patients reporting no pain around the surgical area at the final follow-up and the other 28.9% of patients reporting mild to no pain around the surgical area at the final follow-up. Our results align more with the study by Raikin et al, 13 which showed 100% satisfaction rate, low complication rates, and low levels for BMA harvest at the calcaneus and tibia.
Our study has several limitations such as lack of a control group or matched patients who did not have BMA, sample size, average times for follow-up, the nature of being a retrospective study, and heterogeneity among conditions and surgical procedures included. Additionally, we understand when looking at fusion there are many variables to factor, some selection bias may have occurred, and we would generally prefer to use Iliac crest BMA to treat nonunions. Because of the nature of this retrospective study and lack of a control group, we are unable to conclude any quantitative measure of effectiveness. Nevertheless, the current study reports no complications and 100% patient satisfaction following surgery with calcaneus BMA use; the majority (71.1%) of patients reported no pain at follow-up from the harvest site. Further prospective randomized studies will need to be done to see if BMA from various sites does have an effect on fusion outcomes. Because there is not a vast amount of data on BMA from the calcaneus, this study can help guide future larger studies to continue increasing the data on this topic. This study provides support for use of calcaneus BMA as a surgical augment for the types of cases we performed.
Conclusion
Harvesting BMA from the calcaneus bone used as a surgical treatment augment in this heterogenous retrospective case series was found to be a safe and efficacious procedure. This study showed good results among patients, including little to no pain and no cases of wound complication or iatrogenic neuropraxia after undergoing bone marrow harvest from the calcaneus along with their indicated surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231194056 – Supplemental material for Outcomes and Complications After Bone Marrow Aspirate Harvest From the Calcaneus
Supplemental material, sj-pdf-1-fao-10.1177_24730114231194056 for Outcomes and Complications After Bone Marrow Aspirate Harvest From the Calcaneus by Rodrigo Encinas, Tammy Phillips, Sarah Hall, J. Benjamin Jackson and Tyler Gonzalez in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
IRB application was completed, and the study was exempt. Project title [1950074-1]
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.