
Abstract
A new study published in the journal Nature Biomedical Engineering1 documents a novel diagnostic technology that exploits topically applied nanotechnology to detect skin tissue biomarkers for diagnosis. This concept is demonstrated by noninvasively imaging connective tissue growth factor (CTGF) mRNA in abnormal scar cells, whole tissue, and animal models.
In this commentary, we highlight the main findings and discuss their implications. Successful implementation in the clinic could give rise to self-applied, biopsy-free diagnostic technology and significantly reduce healthcare burden. Crucially, noninvasive visualization of disease biomarkers, mobile device signal acquisition, and Internet-enabled transmission could significantly transform the diagnosis of skin disease and other superficial tissues.
Introduction
Tissue biopsies are necessary for the accurate diagnosis of skin diseases, but their application is limited by the pain, inconvenience, and morbidity experienced by patients, as well as risks of scarring and infection. Many skin diseases, such as abnormal scars, are typically identified by visual identification of scar lesions. However, a visible scar is already mature, having generated significant neotissue, and is unable to benefit from timely administration of prophylactics.
Recently, we showed that spherical nucleic acid (SNA) NanoFlares—a programmable, nucleic acid nanotechnology—addresses this unmet need by allowing noninvasive identification of abnormal fibroblasts and monitoring of scar development in vivo. 1
NanoFlares, approximately 30 nm in diameter, are topically applied (through excipient emulsions) before transepidermal penetration and intracellular entry. Upon interacting with biomarkers strongly expressed in abnormal scar fibroblasts (i.e., connective tissue growth factor [CTGF] mRNA), complementary reporter flares are displaced from the proximity of gold nanoparticle cores regaining their fluorescence signal.
In the absence of a biomarker (such as in undiseased tissue), NanoFlares are inactive and emission signal remains low. NanoFlares targeting reference genes (i.e., GapDH and noncoding sequences) can be simultaneously employed for signal normalization. Thus, abnormal fibroblasts can be discriminated from undiseased ones by their fluorescence signal. In this process, NanoFlares maintain their detection properties and molecular specificity following transepidermal and intracellular entry. CTGF NanoFlares (along with housekeeping and noncoding genes) are evaluated in solution, cell populations, live mice, rabbit, and ex vivo human skin models. The scheme for topical NanoFlare disease diagnosis is summarized in
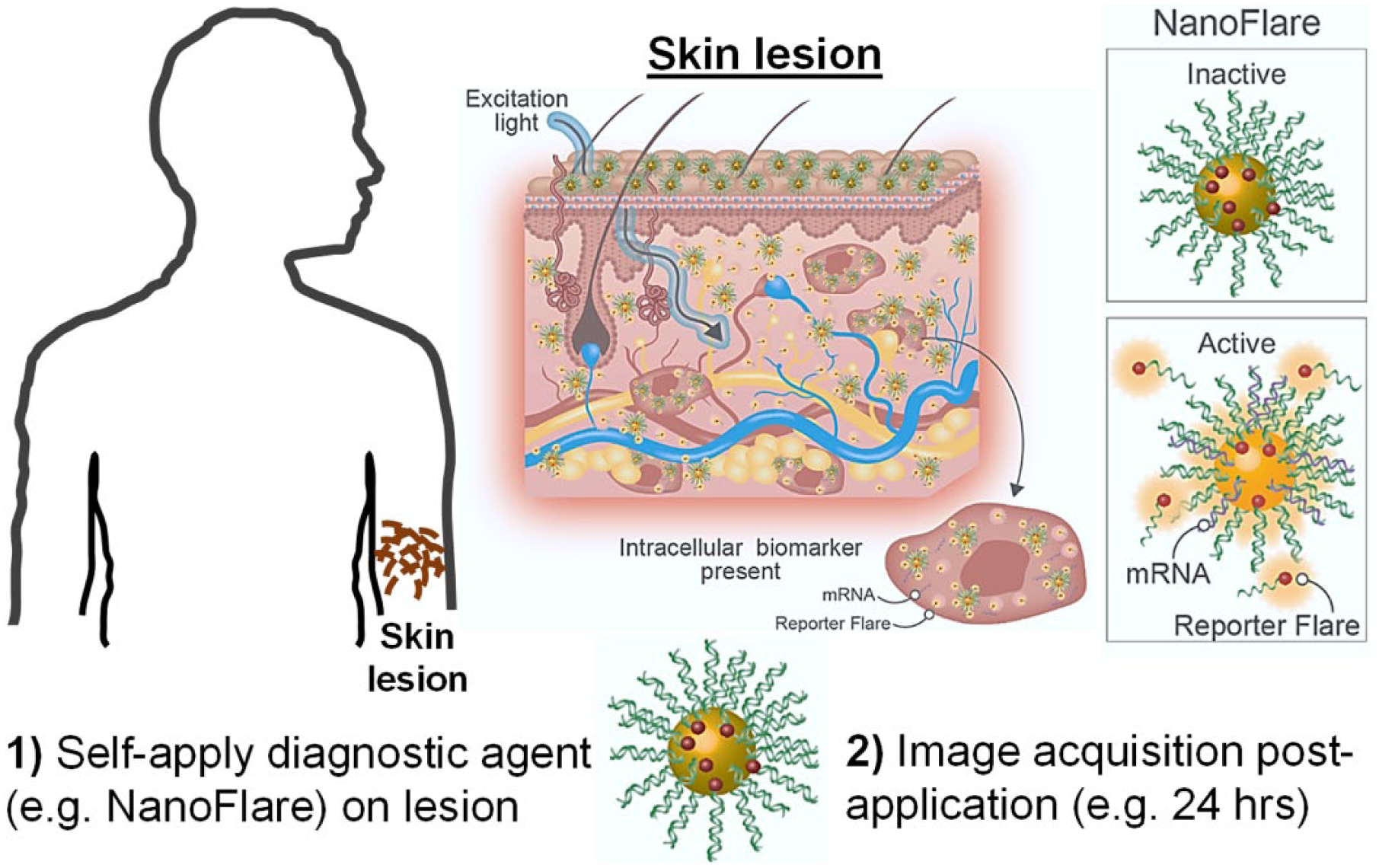
NanoFlares for biopsy-free self-diagnosis. Skin lesions are noninvasively diagnosed by the self-application of suitable diagnostic agents (e.g., NanoFlares). NanoFlares are topically applied on the lesion, which penetrate the skin barrier, interacting with intracellular mRNA biomarkers. In the presence of the target gene (e.g., disease biomarker or other control genes), mRNA interacts with the NanoFlare, dislodging (releasing) the reporter flare. Leaving the proximity of the gold nanoparticle core, a strong fluorescence is generated. Without target gene hybridization, fluorescence signal does not appreciably increase but remains below background levels. In the presence of sufficient disease biomarker, fluorescence signal can be superficially acquired. Portions of this image were originally published in Nature Biomedical Engineering. 1
Transdermal NanoFlare penetration results from their unique nanostructure. They comprise highly packed oligonucleotide strands directionally aligned to cores (comprising a range of different materials, including gold) and even hollow-core nanoparticles. This gives the resultant particles a strong negative surface charge. 3 Although unmodified oligonucleotide molecules do not readily traverse the epidermis, 4 the SNA nanostructure confers passage through skin.1,5 To date, the mechanisms that facilitate transepidermal SNA penetration are unknown. SNAs may utilize either hair follicles or transcellular, paracellular, or other routes to cross the epidermis. Discovering these mechanisms will aid the discovery of novel transdermal materials for therapy and diagnosis.
Transdermal delivery can also be enhanced through other means. Alternatively, we employed microneedles to generate microchannels to deliver molecular probes for detecting the fibroblast activation protein (FAP)-α (~1 kDa) biomarker in whole human skin models. 6 Employing transdermal delivery methods could facilitate a greater range of molecular probes being used for in situ biomarker detection.
Point-of-Care Clinical Disease Diagnosis
NanoFlares have been successfully used for biomarker detection in dissociated cells. 2 However, this is the first instance that NanoFlares have penetrated skin or tissue barriers and detected biomarkers before noninvasively detected in vivo. This work suggests the possibility of real-time, noninvasive mRNA biomarker detection without the need for skin biopsies.
Unlike tissue biopsies that only take a single snapshot of the disease state, NanoFlares may be able to track the effects of therapeutic administration. They may even allow disease monitoring in real time and accurately gauge in vivo response through longitudinal imaging. Thus, disease progression could be monitored by superficially collecting probe signals without tissue removal. Real-time disease monitoring may provide significant benefits over tissue biopsy diagnosis.
Conceptually, this nanodiagnostic process is a significant departure from biopsy-based clinical diagnostics. It possesses the following benefits:
These attributes of topically applied molecular diagnosis agents facilitate the intriguing concept of skin disease diagnosis and monitoring at point of care. For clinical implementation, other practical considerations also need to be addressed, such as safety and biocompatibility (NanoFlare in vivo clearance), which have been addressed in Yeo et al. 1
Looking forward, this technology may even combine with smartphone spectrophotometry for regular (e.g., daily) self-diagnosis. This will protect the patient’s privacy while ensuring timely disease interception with therapeutics. With successful clinical translation, accurate diagnosis can be performed while significantly decreasing the overall healthcare burden.
Diagnosis and Imaging
Disease biomarker signals may be acquired in either centralized or distributed locations self-performed by patients. Ideally, the entire diagnostic process could be fully self-performed. This may consist of nanoparticle self-application and acquisition of biomarker signals using Internet-enabled mobile devices (e.g., a smartphone with externally mounted optical filters). The acquired signals could be transmitted to healthcare personnel for remote assessment and diagnosis. The robustness of the acquisition process can be improved by multiplexing detection probes for signal normalization.
However, this strategy may be limited by nonstandard acquisition parameters that potentially influence signal strength as well as other types of procedural noncompliance. Instead, standardizing the diagnostic process at a single location would incur inconvenience but ensure standardization between different instances of signal acquisitions (e.g., height of device from skin surface).
In-depth exploration of these issues in comparison with traditional biopsies could lead to the eventual realization of a biopsy-free diagnosis process employing topically applied nanoparticles.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Christian Wiraja, Professor Amy Paller, and Professor Chad Mirkin for working together on the original study hence contributing to the development of these ideas.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.