
Abstract
The core and skin temperature of an infant are essential physiological indicators of the baby’s health and an important reference in the selection of baby clothing. The main idea for this is that parents often wrap their infants in covers and clothing based on their own subjective experience, and infants do not have the ability to express themselves verbally, which is likely to result in over- or under-wrapping, leading to babies feeling too hot or too cold and even causing illness. Accurately predicting and determining infants’ skin and core temperatures at different ambient temperatures is a critical concern in infant clothing research. While the overall skin temperature of infants cannot be understood using traditional body temperature robotic measurements, this article develops a three-dimensional infant thermoregulation model with a geometrical appearance similar to an accurate infant model based on finite element method. Through geometric model construction, cell meshing, boundary condition loading, and user-defined functions program debugging, infants’ body surface and core temperature distribution under different ambient temperatures are calculated. The results were compared with published clinical temperature tests and validated, which were in good agreement with the actual test results and proved the validity of the model calculation. Providing a new method for infant temperature prediction, the findings of this study put forward a scientific reference for infant dressing selection and research on intelligent clothing.
Keywords
Introduction
With the continuous development of computer-aided engineering (CAE) technology, using finite element simulation technology to simulate the human thermal regulation mechanism has become a new technical method to study the heat and moisture transfer between the human body and clothing. 1
The three-dimensional (3D) thermoregulation model of the infant with the finite element method (FEM) can effectively calculate the temperature distribution of the infant’s skin surface. Giving guiding suggestions on the research and development of the infant’s dressing method and clothing, it is of great benefit to push forward research on the infant’s body thermal regulation mechanism in the 3D space.
The FEM is essentially a numerical solution method for differential equations. It divides an originally continuous object into finite elements. These elements are connected through a finite number of nodes and recombined by setting reasonable boundary conditions that can be comprehensively solved. Establishing an infant 3D finite element model involves multiple steps, such as a geometric model, mesh division, working conditions and parameters, and boundary conditions.
While many complex thermal regulation models for adults have appeared now and then, the research on human body thermal regulation has been developing for over 85 years. 2 Currently, research group on the thermoregulation model focus on adults,3,4 and many representative models have emerged, such as the Fiala model, the Tanabe model, and the Gagge model. However, there are relatively few studies on infants.4,5 Fischer 6 used the finite integral method to establish a mathematical model of neonatal body thermal regulation to simulate the neonatal body temperature distribution under non-steady-state conditions. The model regards the human body as a whole, so the research results cannot reflect the characteristics of the infant’s local thermal physiological response. In response to this problem, Ying et al. 7 based their work on the two-node model of Gagge et al. 8 and the multi-node model of Stolwijk and Hardy 9 and successively established a seven-node 7 and nine-node 10 thermal regulation model for premature infants, but there are still significant errors between the predicted value and the measured value at some nodes.
In addition, because of the differences in individual characteristics of infants, Pereira et al. 11 proposed a thermal regulation model that can adjust unique features. Still, the effectiveness of this model has not been verified.
What is different from adults is that the function of the infant’s body thermal regulation center is continuous development. The heat dissipation area of small life is significant, and it is easy to dissipate heat; the role of the baby’s thermoregulation system is to maintain the body’s heat balance. 12 When environmental factors destroy the body’s heat balance or the clothing system is insufficient to support it, the central nervous system will be activated. Then, the skin temperature can be controlled within the normal range through its thermal regulation mechanism. 13
The infant’s body structure and thermo-physiological response system are in a state of development and change from birth to 12 months. According to the different ways of producing heat in the infant’s body in further growth months, 14 the infant’s body structure and thermo-physiological response system are in a state of development and change. Mainly rely on consuming brown fat in the body to produce heat; at 3–6 months of age, the brown fat in the body is gradually exhausted, and the trembling heat production function slowly develops. The two heat production methods of brown fat consumption and muscle tremor work together. 15 After 6 months, babies gradually rely on muscle tremors to produce heat, and their thermal regulation mode is the same as that of adults. 16
Therefore, after 6 months, the infant’s body thermal regulation system can be summarized into two parts: the controlled and active systems. The controlled system includes the infant’s body composition and the heat exchange system between tissues, the body surface, and the external environment. These are responsible for responding to related thermoregulation responses. The active system includes a temperature sensor and a body thermal regulation center accountable for sensing the body’s cold and heat conditions and corresponding adjustment responses.
The following problems can be found by summarizing the prior studies: first, there are relatively few research results on infant thermal regulation models, and the establishment of models remains at the one-dimensional and two-dimensional level, and there is no research on 3D models; second, among existing infant thermal regulation studies, models are mainly for the exploration of newborns and premature infants at the birth stage, and there is a lack of research on the heat regulation system of other growing infants.
This article fully considers the influence of infant geometry on the calculation accuracy of the numerical model of body thermal regulation. Based on the FEM, a continuous 3D infant thermal regulation model is constructed to achieve a non-destructive 3D temperature field in the infant’s body.
Establishment of Infant Finite Element Model
Geometric Model
Using a handheld 3D scanner to scan the infant body warmer, a morphology model of the infant’s outer surface was obtained. The handheld 3D scanner used in this article is the Handy SCAN 3D, developed by Cream Form, which uses triangulation to measure the optical reflective target to determine its position relative to the part and can be operated without the need for a tripod or any external tracking device. Its scanning accuracy is 0.030 mm, the volumetric accuracy is 0.020 ± 0.060 mm/m, the measurement resolution is 0.050 mm, and the measurement rate is 480,000 measurements/s.
To ensure the integrity of the scan results, marking points must be pasted on the surface of the infant warmer before scanning. The marking points are pasted in a uniform and randomly distributed way, and the distance between each marking point is about 5 cm.
Second, the scanned geometry file was imported into the retrograde engineering software. Finally, we obtained the complete infant’s outer surface geometry model through filling holes and geometric surface optimization.
To ensure that the shape of the outer surface of the model is more similar to the actual infant, the connection method of the dummy at each joint is consciously ignored in processing of the model. The geometric model of each joint’s upper and lower parts is connected by a continuous curved surface construction method. The curvature of the connection part is approximated to the average value of the connection interface at the upper and lower joints.
It can be seen from Figure 1 that the complete infant geometric model is different from the infant dummy in the joints, which is similar to the natural infant human body.
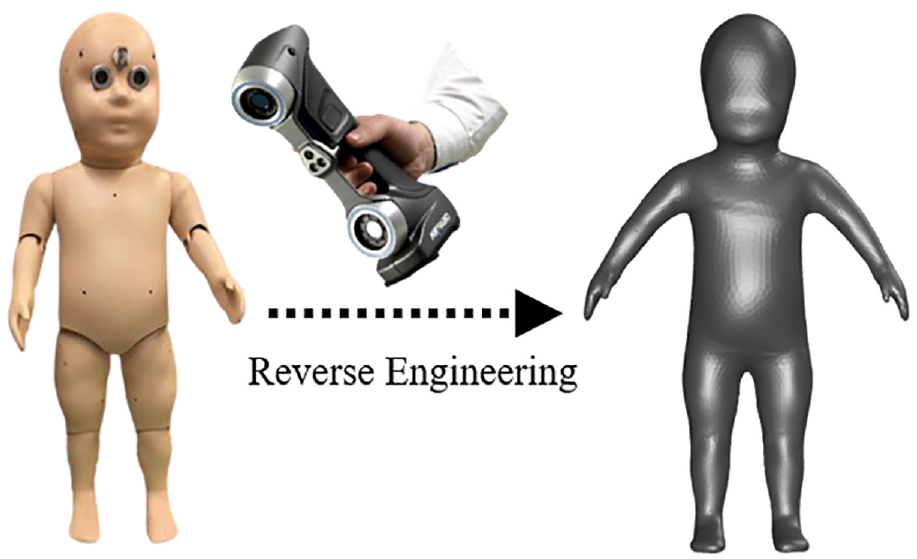
Construction of infant geometric model.
Since there are no norms and standards for infant body measurement methods, this article mainly refers to GB/T 23698-2009 “General requirements for three-dimensional scanning anthropometric methods,” GB/T 22044-2017 “Defined dimensions of anthropometric measurements for infant clothing” and the method proposed by Kwok et al. 17 We measure the size of the infant geometric model constructed in the 3D CAD software. The dimensions of each part of the infant’s body are shown in Table 1.
The size of each part of the infant’s body.
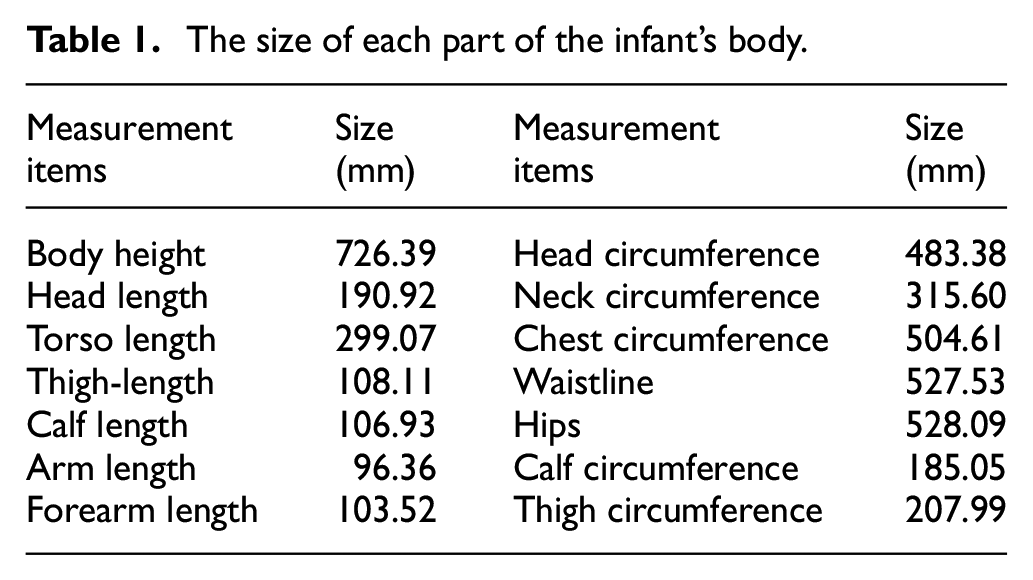
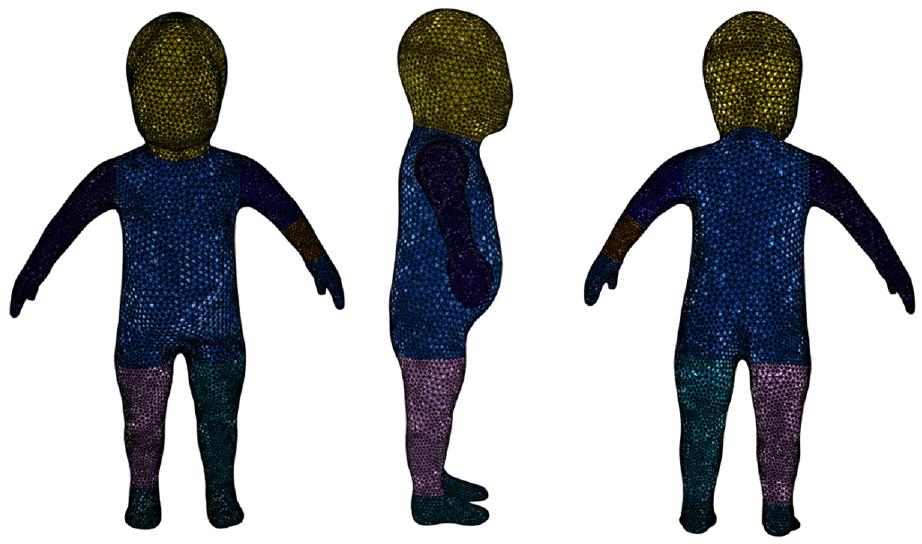
By analyzing the geometric model of the infant’s structure and comparing with the adult body, it can be found that the infant’s head accounts for a more significant proportion of the whole body, while the limbs a smaller proportion as they are shorter, especially the hands and feet. In addition, there are differences in the morphological structure of internal tissues and organs in various parts of the human body. 18 To ensure the accuracy of the calculation of the model, after obtaining the geometric model of the infant’s outer surface, the model is divided into body segments according to the physiological structure of the infant’s body anatomy. The geometric model is divided into 12 trunk segments, which are the head, trunk, upper arm (2), lower arm (2), hand (2), leg (2), and foot (2). The result of infant body segmentation is shown in Figure 2.
The result of infant body segmentation.
Mesh Model
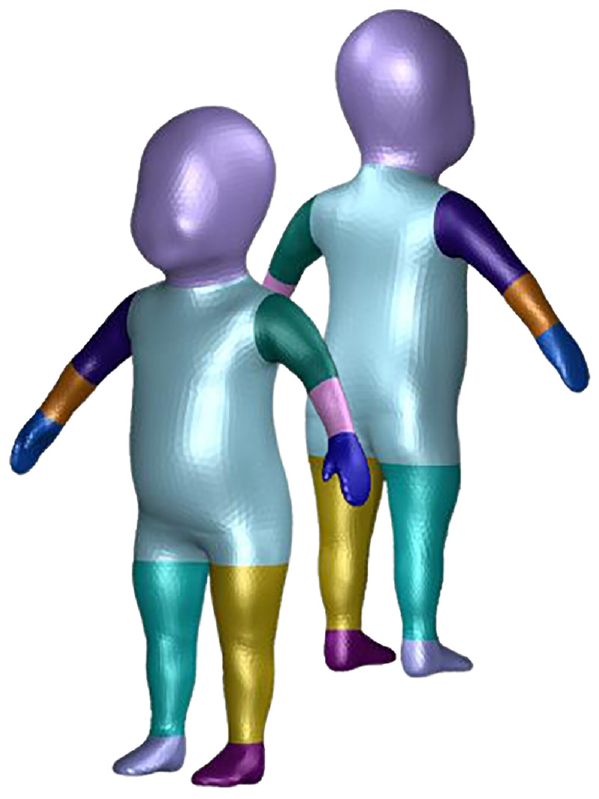
A high-quality finite element model is the basis of finite element calculation. The mesh division is the most critical step in building a finite element model, which directly affects the accuracy of subsequent numerical calculation and analysis results. The division of the finite element mesh should consider both the accurate description of the geometric shape of each object and the detailed description of the deformation gradient. In this article, the surface mesh is divided on the outer surface of the model and inside the model as well, so as to ensure the effective convergence of the calculation results of the body surface temperature.
First, the free meshing technology is used to separate the surface mesh of the model to form a triangular or quadrilateral mesh on the surface of the infant geometric model. With number of 27,496, this grid scale can ensure the balance between accuracy of the infant’s appearance and calculation time consumption.
Based on the principles to reduce the model’s scale, meshes are of different sizes in the infant’s body parts. The meshes are encrypted in areas with significant changes in curvature, such as underarms and crotch bottom, hands, and feet, while sparse in areas of relatively small changes in curvature, such as the front, chest, back, and the other regions. The inspection of the surface mesh quality shows that the maximum skewness of all surface meshes is approximately equal to 0.75, and the result of the infant surface meshing is shown in Figure 3.
Infant surface meshing.
Second, the volume mesh is divided into each section of the model. When dividing, each model section is regarded as an independent solid threshold. There are hexahedral structured grids and tetrahedral grids in the Cartesian coordinate system. Figure 4 shows the results of the body meshing of the infant’s body.
Infant inside volume mesh.
Finite Element Model
This article used the Fluent software platform from the ANSYS-Workbench 2020 (ANSYS, USA) multi-physics simulation platform for the calculations, where the parameters and formulas of the mathematical model are entered through the user-defined functions (UDF) of the Fluent software.
The ambient temperature in the simulation was set at 23°, and the ambient humidity was set at 55%. This experimental condition is consistent with the actual physical experiment conducted by Researcher Garcia-Souto et al. 19 The setting of the simulation conditions is conducive to predicting the accuracy of the simulation results in the later stage.
According to the human body heat balance theory (formula 1), the 3D form of each Pennes equation is brought into each calculation unit through UDFs of development platform. The equation is calculated in each unit’s x, y, and z directions. The equation can be expressed as the following type:


The left side of the equation represents the non-steady-state internal energy, and the first term on the right side of the equation describes the heat transfer of power within the tissue. In the calculation, it is assumed that the human tissue is a variety of peer materials. S is the human body’s heat storage rate, W/m2. M is the human body’s metabolic rate, W/m2. W is the mechanical work done by the human body, W/m2. E is the heat taken away by sweat evaporation and exhaled water vapor, W/m2. R is the radiant heat transfer between the outer surface of the human body and the surrounding surface, W/m2. C is the convective heat transfer between the outer surface of the human body and the environment, W/m2.
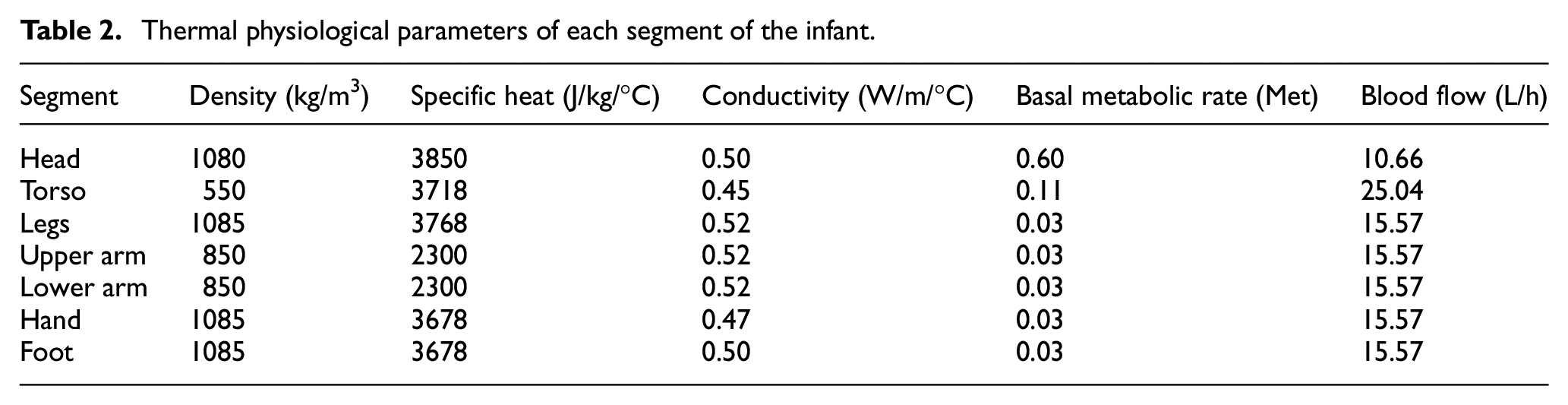
The physiological parameters for each part of the infant are obtained through a literature review.4,7,11,20 Since the thermal physiological parameters for older infants are relatively few and incomplete, this article first conducts a literature survey on development of the tissues and organs of older infants. Based on the research results, approximate thermo-physiological parameters are selected from the published literature for calculation as shown in Table 2.4,7,11,20 It is worth noting that, in the most advanced processing, the temperature of each area is concentrated to a single value.
Thermal physiological parameters of each segment of the infant.
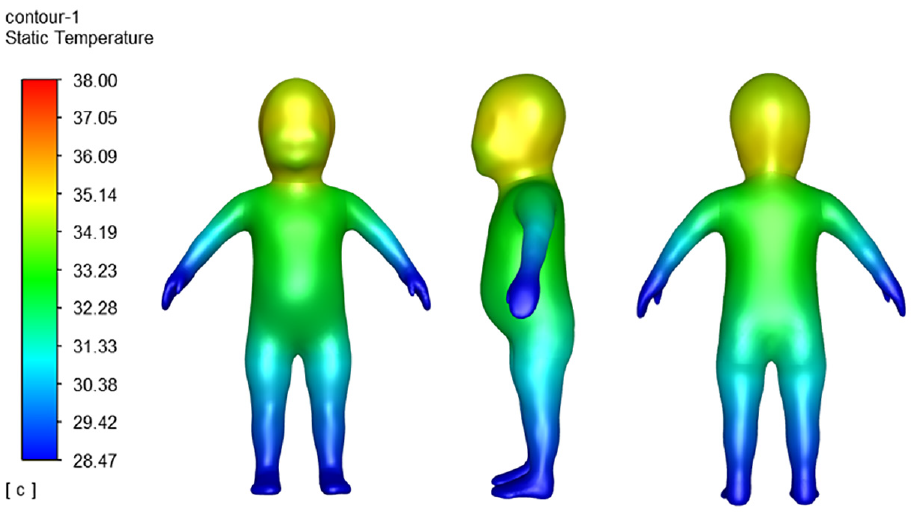
Skin temperature calculation result.
Before calculation, it is necessary to calibrate the contact surface between each section in advance and set them as a single contact surface, so as to ensure that the grids on both sides of the surfaces are independent and the calculation is continuous and concurrent.
Calculation Results and Model Verification
Calculation Results
The cloud chart shows that the body surface temperature of the hands and feet is the lowest. The body surface temperature of the forehead is the highest, followed by the torso. The temperature of the toes is the lowest, and the effective temperature of most extremities is 29.02°C.
The temperature distribution inside the infant model can be obtained by segmenting the infant finite element model along the central sagittal plane. The calculation result is shown in Figure 6. From the distribution result of the temperature field cloud map, it can be seen that the average temperature of the infant’s forehead is higher than that of the torso, and the highest temperature area appears on the forehead.
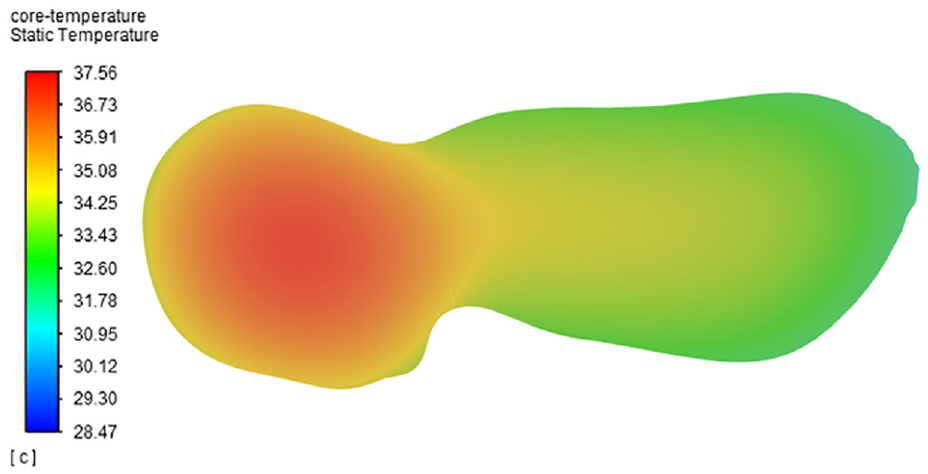
Core temperature calculation result.
Amid little research data on infants’ body temperature, the verification of the model, unlike adults, is a difficult part of this article. In addition, to fully guarantee safety in actual measurement, the test was carried out in a dressed state, and the dressing method of the baby took account of the guardian’s advice, so the test result is different from the infant’s naked body surface temperature.
Compared to the validation of adult human models, there are fewer data from experimental studies on infant temperature measurement, considering that the immune system of infants is not yet well developed, and also considering the many external factors that interfere with the testing of infants, the testing methods and test points are not the same among scholars. This is one of the reasons for the discrepancy between the model calculations and the actual published test data. To verify the accuracy of the calculation results of the constructed model, this article consciously sets the environmental conditions in the simulation to be consistent with the ecological requirements in the actual experiment by Garcia-Souto 19 and Tourula 21 before the simulation calculation.
Furthermore, in the validation of the model, as the authors only stated the temperature measurement area, but not the specific temperature measurement sites, in this study, the average of the three sites near the center of the area was calculated based on the temperature measurement area provided by Garcia-Souto and Marjo Tourula, and was finally calculated and contrastive analyzed with its results.
The temperature measurement points are chosen as the same position in the study of Garcia-Souto and Marjo Tourula for data extraction. Garcia-Souto’s infant body temperature experiment consists of two parts: core and skin temperature, and is characterized by a large number of temperature measurement points and well-thought-out test conditions. A total of 14 points were tested for skin temperature, including the center of the forehead, chest, elbow, thigh, abdomen, front and back of the thigh, front and back of the calf, upper back, and lower back. For the core temperature, the authors also indicated that the infant’s core temperature is easily interfered with by the sleeping position and whether the infant is awake or not, so the infant’s forehead, axilla, and cochlea temperatures were selected as the core temperature for the awake state. In order to further illustrate the validity of the model’s calculations and to compare them with the results of Marjo Tourula’s experimental tests, the author chose the infant’s head, chest, lower arms and back of the hands as the test points for skin temperature measurements.
As the simulation results are presented in cloud plots, the temperature values at five points in the target area were selected for averaging to better correspond to the actual experimental results. The position of the red dots in the graph indicates the mean value, and the error line indicates the standard deviation (SD) of the selected values in the target area. The comparison between the model calculation results and the experimental test results is shown in Figures 7 and 8.
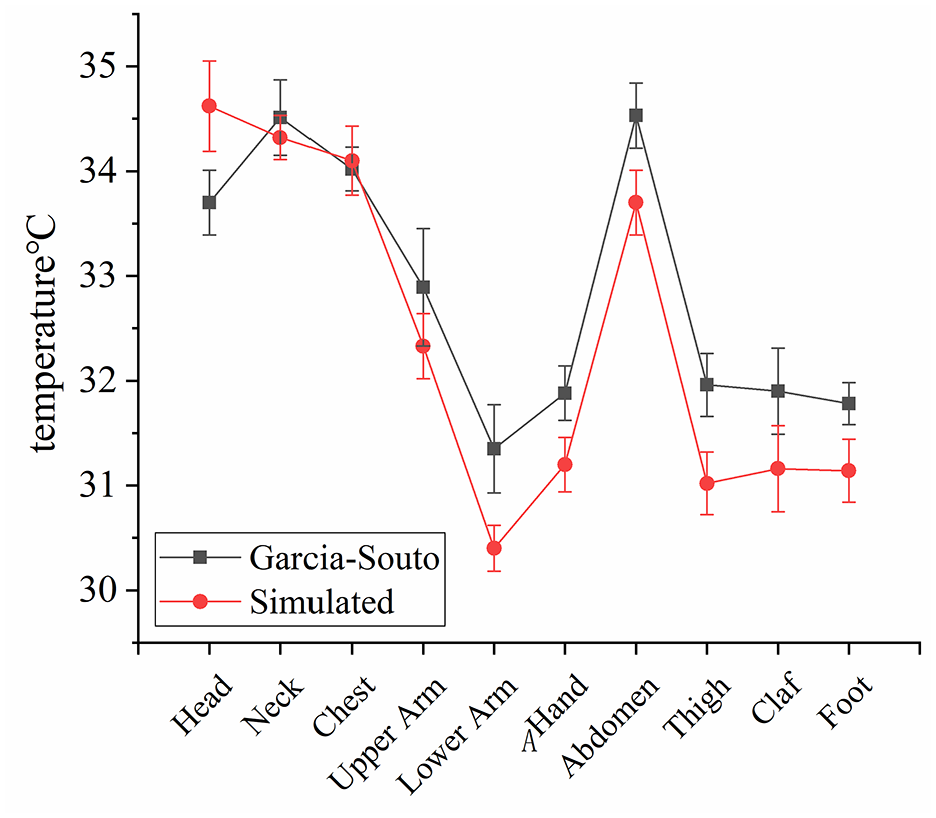
Comparison between the model calculation results and Garcia-Souto experimental test results.
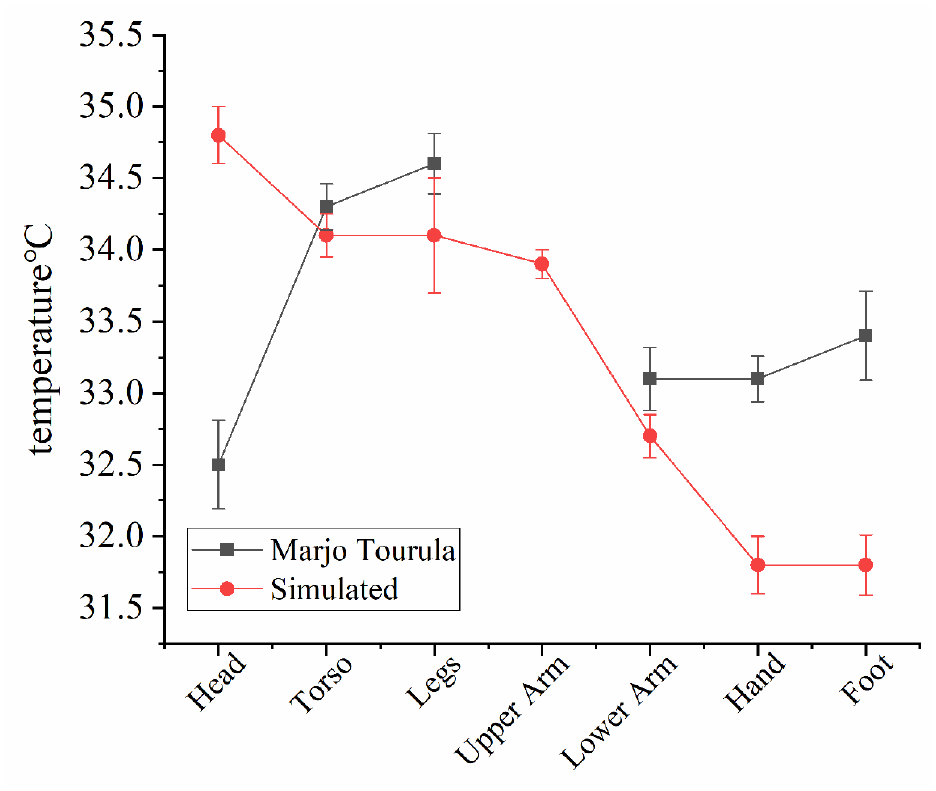
Comparison between the model calculation results and Marjo Tourula’s experimental test results.
As shown in Figure 7, on the whole, the calculated results of the body surface temperature of each part of the infant’s body are consistent with the experimental results, and there are partial deviations. Researchers carried out physics experiments in the condition babies are dressed, which is an essential reason for data bias. Partially, the calculation result of the model on the forehead is higher than the actual test error upper limit, and the calculation results of the other parts are slightly lower than or consistent with the test results. Especially in the chest and upper arms, the calculated results are equivalent to the average of the test results. The calculated results on the parts that are far away from the limbs, such as hands, feet, lower arms, and calves, are all lower than the average of the test results. Especially the hands and feet, in the actual wrapped test condition, have a higher body surface temperature, which cannot objectively characterize the actual nude temperature in these area. The actual temperature should be lower than the test temperature, which further explains the accuracy of the calculated results of the model.
To better represent the infant model’s internal temperature distribution and further demonstrate the calculated results of the core temperature of the model, the calculated model was divided into two parts through the sagittal plane. The results of the calculation are shown in Figure 6. According to Garcia-Souto’s 20 research, infant core temperature is influenced by factors such as sleep position and whether or not they are awake. Therefore, the infant’s core temperature must be expressed through more comprehensive data. The central region of the forehead, the axillary region and the region near the rectum were selected for data extraction. Three temperature points were chosen for each region. The core temperature of the infant model was expressed as the average temperature value of the above mentioned points of all regions. The calculation result is 36.63°C (SD = 0.82°C). To further illustrate the model’s validity, the results were compared with those of the study of Garcia-Souto, 20 in which the infant’s core temperature was 36.59°C (SD = 1.70°C). Nevertheless, this study shows the temperature distribution inside the infant model in the form of a cloud chart so that you can observe the core temperatures of the infant model according to your own experience. Calculating the core temperature of the infant model described in this article is only a reference method.
As shown in Figure 8, compared with the test result of Marjo Tourula, the calculation result of this article has a more significant forehead temperature deviation. And except for the forehead, the test temperature of other parts is only higher than or similar to the simulated temperature. This may be because the baby wears clothing in the actual measurement and has accumulated heat inside the clothing when the baby wears it for a long time.
Conclusion
This article establishes a full-scale continuous 3D infant body thermal regulation model based on the FEM. The model includes 12 segments, and each trunk is assigned a response to the thermal physiological parameters of the person. The construction of this model takes into account physiological mechanisms such as blood perfusion, respiration, and metabolism. In addition, the model’s physiological parameters and environmental conditions can be modified to realize the extended application of the model under different ecological conditions. The development of the 3D infant thermal regulation model provides a more realistic and accurate representation of the temperature distribution of infants.
Different from the traditional model of infant body thermal regulation based on the node method, the model established in this article can directly observe the distribution of the infant’s body surface temperature from three dimensions and, at the same time, can obtain the temperature of any position on the infant’s body by establishing a profile method.
This article only verifies the calculation results under one environmental condition. From the perspective of the technical path, as long as the correct thermo-physiological parameters are selected, the model can be extended to a broader range of environmental conditions. However, the calculation results under other environmental conditions are still in progress. Experimental verification will be further discussed in follow-up research. The calculation results of the model can provide a reference for the design of the heat insulation of the infant’s bedding and can also provide a theoretical basis for the creation of the infant’s intelligent temperature-regulating clothing.
An infant thermoregulation model is an effective tool for calculating infant skin temperature distribution. This method can provide a reference for the warm design of baby clothing and avoid physical diseases caused by wearing too much or too little. In addition, the research results can provide a basis for the design of a baby’s temperature-adjusting clothing. By calculating the baby’s skin temperature distribution at different ambient temperatures, different temperature adjustment modes can be designed to ensure the baby’s thermal comfort.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the financial support from the Fundamental Research Funds for the Central Universities (grant no. 2232022G-08) and the International Cooperation Fund of Science and Technology Commission of Shanghai Municipality (grant no. 21130750100).