
Abstract
Purpose
To assess the clinical and radiographic outcomes, at a minimum follow-up of 4 years, following HSA using pyrocarbon in patients that had prior open Latarjet.
Methods
The authors retrieved the records of 61 consecutive patients that underwent HSA with a pyrocarbon humeral head at 2 centers between December 2013 and October 2019. Eight patients (9 shoulders) had undergone previous Latarjet procedures without other surgical antecedents. Patients underwent radiological assessment, and clinical assessment including Constant score, Subjective Shoulder Value (SSV), and pain on VAS. Finally, range of motion was assessed, including active forward elevation and external rotation.
Results
The initial cohort of 9 shoulders, comprised 1 woman and 7 men (1 bilateral), aged 52.5 ± 5.2 at their index HSA, which was performed 27.7 ± 9.3 years following their prior Latarjet procedure. One shoulder required conversion to reverse shoulder arthroplasty, 3 years after HSA. The remaining 8 shoulders were assessed at 6.1 ± 1.6 years (range, 4-8) after the index HSA. Glenoid erosion only progressed in 1 shoulder from mild to moderate. The Constant score was 79.6 ± 12.7, pain on VAS was 1.0 ± 2.1, and SSV was 80.0 ± 25.6. The active forward elevation improved from 96°±41° to 151°±29°, and external rotation from 11°±17° to 32°±8°.
Conclusion
Patients that underwent HSA using pyrocarbon heads following prior Latarjet had satisfactory clinical scores, and glenoid erosion only progressed in 1 patient. Furthermore, only 1 patient required conversion to RSA. The clinical relevance is that HSA using pyrocarbon heads is a safe treatment and grants satisfactory clinical outcomes in patients with prior Latarjet.
Level of Evidence
Level III, retrospective comparative study
Introduction
Shoulder instability can be managed using a variety of conservative or surgical treatments, including capsulolabral Bankart repair, remplissage for Hill-Sachs lesions, and Latarjet bone-block procedures.1–3 While surgical treatment could prevent or delay post-instability shoulder osteoarthritis, some cases develop osteoarthritis that may or may not be related to the previous instability or surgery, and ultimately require shoulder arthroplasty.
Performing shoulder arthroplasty can be challenging in cases that had prior bone-block procedures, due to the presence of metallic hardware, the subscapularis split, and altered glenoid morphology. While selecting between anatomic shoulder arthroplasty (TSA) or reverse shoulder arthroplasty (RSA) depends primarily on patient age and rotator cuff status, choosing between total or hemi-shoulder arthroplasty (HSA) depends on patient activity and damage to the glenoid. One study investigated the outcomes of shoulder arthroplasty following Latarjet, and included 19 patients, 7 of which underwent RSA, 9 TSA, and only 3 HSA. 4 For young and functionally active patients with minimal glenoid erosion or deformity, HSA seems to be a suitable bone-preserving option, although the use of metallic heads has been reported to cause glenoid erosion.5–9
To overcome the drawbacks of metallic humeral heads in HSA,5–9 pyrocarbon humeral heads were introduced as an alternative, and demonstrated promising short- and mid-term outcomes.10–13 For over a decade, the senior authors have systematically used pyrocarbon humeral heads when performing HSA, with satisfactory clinical scores and minimal glenoid erosion (REF BLINDED). The purpose of this study was therefore to assess the clinical and radiographic outcomes, at a minimum follow-up of 4 years, following HSA using pyrocarbon in patients that had prior open Latarjet with successful fusion. The hypothesis was that HSA in patients with prior Latarjet grants satisfactory clinical outcomes with minimal complications.
Methods
The authors retrieved the records of 61 consecutive patients that underwent HSA with a pyrocarbon humeral head (Tornier SAS, part of Stryker, Montbonnot, France) at 2 centers between December 2013 and October 2019 (Figure 1). A total of 8 patients (9 shoulders) had undergone previous Latarjet procedures with successful fusion, and no other surgical antecedents. All patients provided informed consent to participate in the study which was approved by the ethical board in advance (IRB BLINDED).

Flowchart.
Radiological and Clinical Assessment
Patients underwent radiological assessment using anteroposterior x-ray views (external, neutral and internal rotation). Glenoid morphology was preoperatively assessed according to the classification of Walch et al 14 for all patients using computed tomography (CT) scans, which also confirmed absence of anterior subluxation in all cases. Glenoid erosion was postoperatively assessed on plain radiographs according to the Sperling classification (none, mild, moderate, or severe). 9 An independent observer collected the Constant score, 15 Subjective Shoulder Value (SSV), and pain on VAS (0-10). Finally, range of motion was assessed (including active forward elevation, external rotation, and internal rotation) in addition to strength of the internal (using belly press test).
Surgical Technique
All patients were operated under general anesthesia and interscalene block in the beach chair position. The scar of the prior Latarjet procedure was used as a reference to perform the deltopectoral incision (Figure 2), and was widened proximally and distally if necessary (Figure 3), avoiding the axillary fossa to prevent a retractile bridle. The deltopectoral groove is identified in its upper portion in the healthy zone of the Mohrenheim triangle, and the cephalic vein is moved towards the deltoid to protect it.
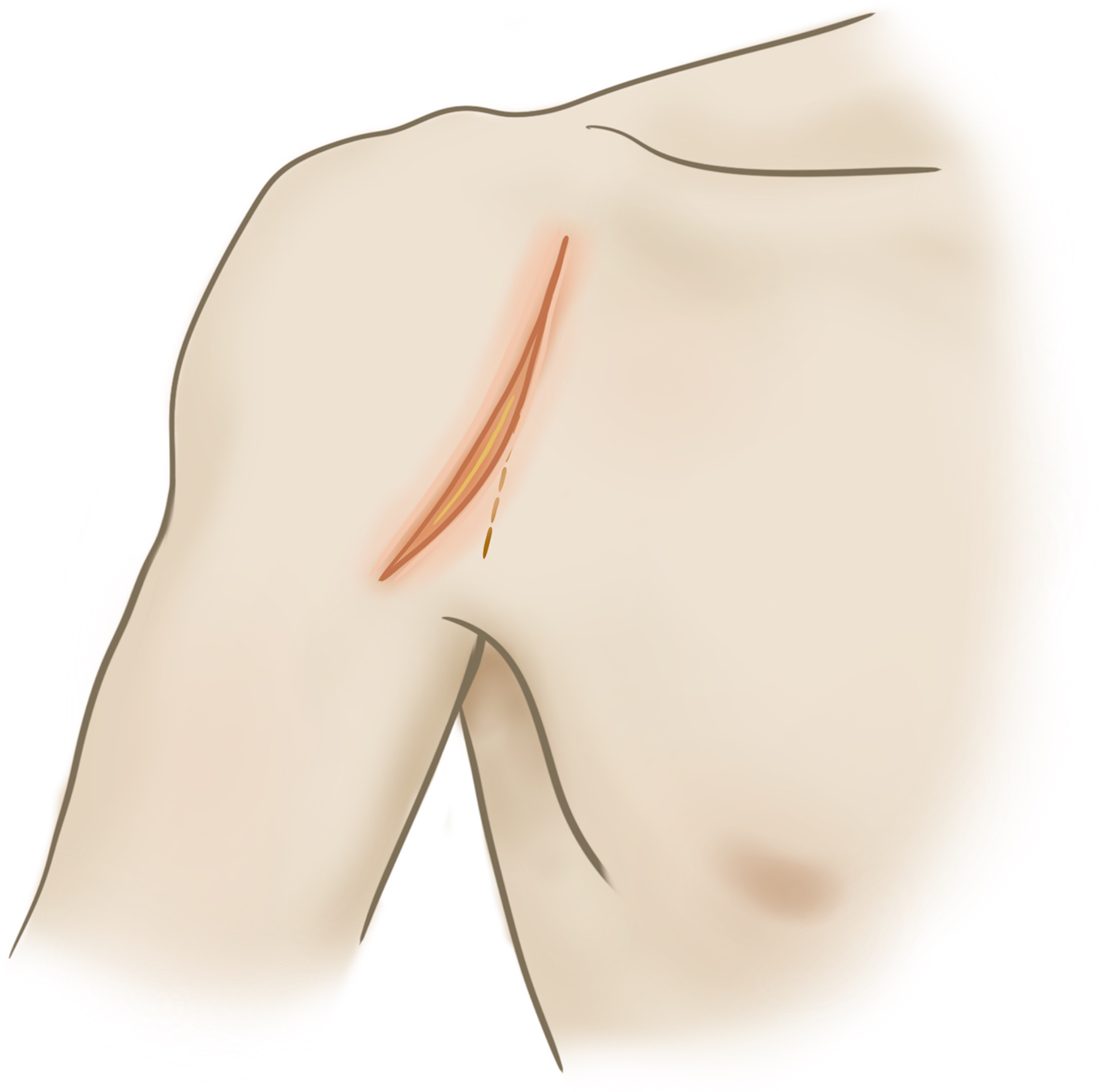
The scar of the prior Latarjet procedure was used as a reference to perform the deltopectoral incision.

The scar of the prior Latarjet procedure was used as a reference to perform the deltopectoral incision was widened proximally and distally if necessary.
As all patients had prior Latarjet, the anatomical reference of the coracoid process and conjoint tendon no longer exist, and can therefore not provide support for the retractor. Furthermore, the presence of scar tissue on the anterior aspect of the subscapularis could render it dangerous to identify the elements of the brachial plexus and the split of the joint tendon through the subscapularis. The authors therefore advise against removing the screw at this stage of the procedure.
The limits of the subscapularis muscle must be identified before its tenotomy; above the interval of the rotator cuff, which must be open; outside the bicipital groove and below the ligated anterior circumflex pedicle. Partial tenotomy of the upper pectoralis major is performed if necessary to improve exposure of the lower subscapularis.
Tenotomy of the subscapularis is performed vertically in the tendinous zone, leaving a tendinous stump on the lesser tuberosity. The anatomical anterior and inferior limits of the humeral head are exposed. A humeral head retractor is introduced into the glenohumeral joint and the anterior surface of the scapula is gradually exposed to the medial side of the coracoid bone block on the deep surface of the subscapularis, allowing a link-type retractor to be inserted (Figures 4 and 5). To enable removal of the screws used for the prior Latarjet procedure, a complete release of the subscapularis using a tenotomy must be performed, ensuring that all the fibrous tissue is removed.

A humeral head retractor is introduced into the glenohumeral joint and the anterior surface of the scapula is gradually exposed to the medial side of the coracoid bone block on the deep surface of the subscapularis.

At this stage the screws can be carefully removed.
At this stage, the screws of the prior Latarjet are removed, as all metal material must be removed to avoid contact between the metal and the pyrocarbon. If total extraction of all screw remnants is not possible, or if there are any metal remnants in the bone, a total shoulder replacement should be performed.
Once the screws have been removed, the usual technique for HSA can be performed. It is worth noting that, as the pyrocarbon head is designed with 2 mm of lateralization, the humeral head osteotomy must be anatomical, and it is preferable to undersize if in doubt, to avoid a proud prosthesis and/or overstuffing. Regardless the glenoid shape, no additional procedures such as microfracturing or reaming are performed on the glenoid surface or on the labrum; the goal is to enable spontaneous remodeling of the glenoid surface. At the end of the procedure, the subscapularis is repaired using 3 non-absorbable trans-osseous sutures.
For the postoperative rehabilitation, the shoulder is placed using a splint in internal rotation for the first 6 weeks. Self-rehabilitation is performed immediately following surgery, limiting external rotation to avoid damage to the subscapularis sutures.
Statistical Analysis
Descriptive statistics were used to summarize the data. All available patients were included, and therefore a sample size calculation was not performed. For continuous variables, comparisons between groups were performed using t-tests. P values <0.05 were considered significant. Statistical analyses were performed using R, Version 4.1 (R Foundation for Statistical Computing).
Results
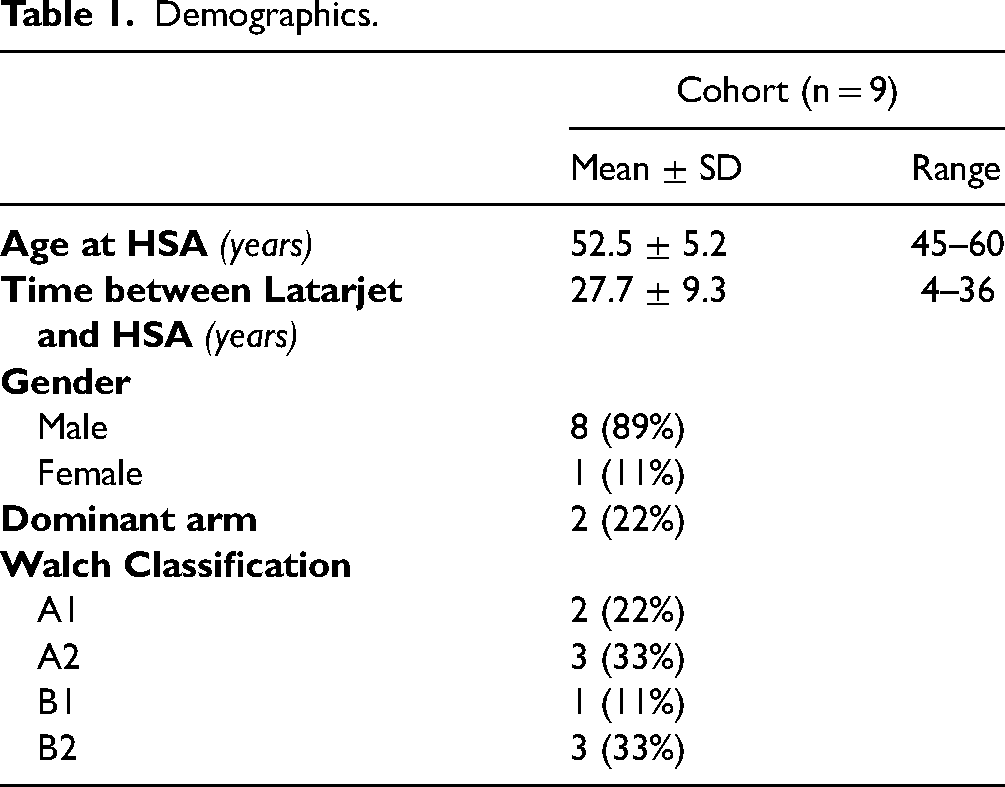
The initial cohort of 9 shoulders, comprised 1 woman and 7 men (1 bilateral), aged 52.5 ± 5.2 (range, 45 to 60) at their index HSA, which was performed 27.7 ± 9.3 years following their prior Latarjet procedure (range, 4 to 36) (Table 1). The Walch glenoid morphology was A1 in 2 shoulders, A2 in 3 shoulders, B1 in 1 shoulders, and B2 in 3 shoulders. One shoulder required conversion to RSA (Figure 6), 3 years after HSA, due to persistent pain and discomfort which did not improve with physiotherapy, balneotherapy or infiltrations. The reasons for persistent pain and discomfort could not be identified, as the authors ruled out any infection, rotator cuff tear, or other structural lesions.

Radiographs of the patient that required revision; a) Last follow-up with the pyrocarbon HSA; b) After conversion from HSA to RSA.
Demographics.
The remaining 8 shoulders were assessed at 6.1 ± 1.6 years (range, 4-8) after the index HSA. The glenoid erosion progressed from mild to moderate in 1 shoulder, while it did not change in the other 7 shoulders (Table 2; Figure 7)). The Constant score was 79.6 ± 12.7, pain on VAS was 1.0 ± 2.1, and SSV was 80.0 ± 25.6 (Table 3). It is worth noting that 7 patients had satisfactory clinical outcomes, with Constant scores between 70 and 88, SSV between 70 and 100, and pain on VAS between 0 and 2. Only 1 patient had poor clinical outcomes with Constant scores of 51, SSV of 20, and pain on VAS of 6, but this patient was unwilling to undergo further assessment or treatment. The active forward elevation improved from 96°±41° to 151°±29°, and external rotation from 11°±17° to 32°±8°. Internal rotation was at L5 in 1 patient, T10 in 2 patients, and T12 in 5 patients.

Radiographs of patient with pyrocarbon HSA after Latarjet.
Glenoid wear.

Pre- and post-operative clinical scores.

Discussion
The most important findings of this study were that at a follow-up of 6.1 ± 1.6 years, patients that underwent HSA using pyrocarbon heads following prior Latarjet had satisfactory clinical scores, and glenoid erosion only progressed in 1 patient. Furthermore, only 1 patient required conversion to RSA. The clinical relevance of these findings is that HSA using pyrocarbon heads is a safe treatment and grants satisfactory clinical outcomes in patients with prior Latarjet.
A study by Willemot et al 4 investigated the outcomes of RSA, TSA, and HSA in 19 patients that had previous Bristow or Latarjet procedures. Willemot et al found that of the 3 patients that underwent HSA, 2 of which required conversion to TSA due to glenoid erosion (66.6%). This rate of conversion due to glenoid erosion is high compared to the present study in which only 1 of the 8 shoulders had progression of glenoid erosion (12.5%). The main difference between Willemot et al and the present study is the material of the humeral heads, where the former used metallic heads, and the latter used pyrocarbon which is known to have very little wear, and causes minimal glenoid erosion.10,12,16
The surgical technique to perform HSA using pyrocarbon heads in patients with prior Latarjet does require slight adjustments. The deltopectoral incision required for HSA does not correspond to the incision made for an open Latarjet procedure. Therefore, to perform HSA, the existing incision is either enlarged without crossing the axillary sulcus to prevent bridles, or a more lateral incision is made. Furthermore, during the surgery it is essential to be aware of the potential problems with the screws used for Latarjet. Previous studies have reported rupture of the screw heads, but luckily in the present study this problem was not encountered. Finally, it is worth noting that it is of utmost importance that the screws have to be removed before implanting the pyrocarbon humeral heads, as it could cause scratch or crack the pyrocarbon.
Recently, a study by Garret et al 16 investigated the outcomes of pyrocarbon head in HSA at 5–7 years follow-up, in patients mostly free from surgical antecedents, and found postoperative Constant scores of 80.8, pain on VAS of 0.8, and SSV of 82.8. The outcomes reported by Garret et al are comparable to the outcomes of the present study in which every patient had prior open Latarjet, which demonstrates that the outcomes are similar in patients with no antecedents, versus those with antecedents. Direct comparative studies should be performed to confirm these findings.
This study has several limitations that should be taken into account when interpreting the results. Although the only other study on HSA following prior Latarjet included only 3 patients, the present study also investigated a small cohort of only 8 patients (9 shoulders), making it difficult to draw firm conclusions of the effect of the treatment. Furthermore, the small cohort did not allow for regression analyses to investigate factors that could be related to the clinical outcomes. Finally, this was a case series with no control group, which does not allow direct comparison with patients that underwent HSA using metallic heads.
At a follow-up of 6.1 ± 1.6 years, patients that underwent HSA using pyrocarbon heads following prior Latarjet had satisfactory clinical scores, and glenoid erosion only progressed in 1 patient. Furthermore, only 1 patient required conversion to RSA. The clinical relevance of these findings is that HSA using pyrocarbon heads is a safe treatment and grants satisfactory clinical outcomes in patients with prior Latarjet, but long-term studies are required to confirm its efficacy.
Footnotes
Acknowledgments
The authors are grateful to Alexandre Clair for the illustrations he created. Floris van Rooij and Mo Saffarini are part of the ReSurg working group.
Authors’ Contributions
LL Study design, data collection, interpretation of findings and manuscript editing.
JG Study design, data collection, interpretation of findings and manuscript editing.
FVR Methodology, Data curation, Formal analysis, Statistical analysis, Manuscript writing.
MS Methodology, Data curation, Formal analysis, Manuscript writing.
AG Procurement of funding, Study design, data collection, interpretation of findings and manuscript editing.
All authors approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All patients provided informed consent for the analysis and use of their data, and the institutional review board of the GCS Ramsay Santé for Education and Research (Paris, France) approved this study in advance (IRB #: COS-RGDS-2023-11-001-GODENECHE-A).
Funding
The authors are grateful to “GCS Ramsay Santé pour l’Enseignement et la Recherche” for funding the statistical analysis and manuscript preparation for this study.