
Abstract
Purpose
To evaluate both the short-term clinical and radiological results of reverse shoulder arthroplasty (RSA) with uncemented locked stem in the management of a proximal humerus fracture (PHFs) in the elderly.
Methods
Retrospective study including 40 consecutive 3–4 part proximal humerus fractures treated with reverse shoulder arthroplasty with a minimum of 24 months follow-up. In all the cases, the greater tuberosity (GT) was reattached with a standardized suture technique and a local horseshoe bone graft. All the patients were assessed at the 24-month follow-up with Constant-Murley Score (CMS) and Visual Analog Score (VAS). Radiographic healing of the greater tuberosity was noted in addition to stem locking screws radiographic changes. Complications and revision rates were reported.
Results
Mean final CMS for this cohort was 80 points. The greater tuberosity healed in the anatomic position in 90% of the cases (N = 36), obtaining an average CMS of 80 in these patients. Healing of the greater tuberosity did not occur in 10% of the cases (N = 4), obtaining an average CMS of 60. All patients scored above 100° in forward elevation with a mean of 140°. Mean active external rotation was 30°. Low-grade scapular notching was reported in <1% of the cases. Major complications were reported in one patient with an acromial fracture. No complications or loosening of stem locking screws were noted. There were no reoperations.
Conclusion
In the elderly population, reverse shoulder arthroplasty utilizing a fracture-specific locking stem, low-profile metaphysis, suture-friendly groove, meticulous suture technique, and local bone grafting allows adequate fixation, variable prosthesis height adjustment, and enhances greater tuberosity healing. This approach yields positive short-term clinical outcomes without complications related to the stem's locking screws.
Level of Evidence
Level IV Retrospective Case Series
Fractures of the proximal humerus stand as the third most prevalent fragility fracture in individuals aged over 60, constituting nearly 30% of upper extremity fractures and following the most common upper extremity fracture in this population, distal radius fractures.1–5 Proximal humerus fractures usually occur after a fall from standing height and mostly affect females, likely due to lower bone quality.6–10 Moreover, the incidence is expected to rise in the following years due to a demographic trend exhibiting an aging population. 6 Most PHFs are nondisplaced, and if displacement occurs, it is minimal and observed in 50%-90% of cases.5,11 Factors such as bone quality, fracture pattern, patient function, and level of independence should be considered when making treatment decisions for complex PHFs. 10 Conservative management is the typical approach for these fractures, resulting in favorable function and positive clinical outcomes.11–14 However, a significant proportion of patients report some degree of disability even after 2 years. Displaced multi-fragmented fractures (Figure 1), on the other hand, still occur in a minority (< 6%) of cases and are associated with poor shoulder function and pain if treated nonoperatively.10,12,15 In response to decreased shoulder function and their effects on the patients’ daily lives, surgeons have explored various surgical options including reverse shoulder arthroplasty. 13 Numerous published case series on RSA as a treatment alternative for these fractures consistently report positive functional outcomes.16–18

X-ray of multi-fragmented proximal humerus fracture.
The use of RSA for managing PHFs is progressively rising.17,19–21 Cazeneneuve and Cristofari 22 have shown that, in contrast to hemiarthroplasty, reverse arthroplasty is less reliant on greater tuberosity healing for achieving favorable functional outcomes. Although traditionally relying on cemented techniques, recent reports have demonstrated comparable results with uncemented press-fit fixation, depending on stem coating for humeral stem fixation and stability. 23 Nonetheless, the use of an uncemented locked stem introduces the capability to stabilize the stem regardless of bone quality. 24
The purpose of this study was to investigate clinical and radiological outcomes, including the rate of greater tuberosity healing, using reverse shoulder arthroplasty uncemented locked stem design in the treatment of complex proximal humerus fractures in 40 patients over 60 years of age at the 2-year follow-up.
Materials and Methods
A total of 40 consecutive female patients aged 67-91 years old (mean age 78) with Neer's 3-4 part proximal humerus fractures were treated with reverse shoulder arthroplasty with uncemented locked stem design (Humelock II, FX Solutions, France). Both comorbidities and demographics were assessed. All patients underwent surgical treatment acutely within one week of injury and had a follow-up of 24 months. Clinical outcomes were evaluated with a Constant score and Visual analog scale. At the 24-month, radiographs were obtained and evaluated for greater tuberosity healing. Lesser tuberosity healing was not evaluated. Possible complications including greater tuberosity displacement, healing of the greater tuberosity, stem loosening, scapular notching, and infections were evaluated. Additionally, a thorough assessment of stem locking screws was performed for loosening or related complications.
This was a retrospective Level IV case series study conducted by a sports medicine fellowship-trained surgeon. Inclusion criteria were as follows: patients admitted between August 2018 and June 2020, medically stable as per internal medical department and anesthesia department, 3-4 part displaced proximal humerus fractures according to the Neer classification, surgically treated with cementless locked RSA in <7 days since trauma, and a minimum follow-up of 24 months.
Radiologic Analysis
The senior author (A.R.) examined standard x-ray pictures and computed tomography scans (Figure 2) with 3D reconstructions of patients with PHFs (Figure 3) to categorize fractures and collect data. A digital ruler was used to calculate the displacement of the greater tuberosity in the AP view.

Computed Tomography of Neer four-part proximal humerus fracture.
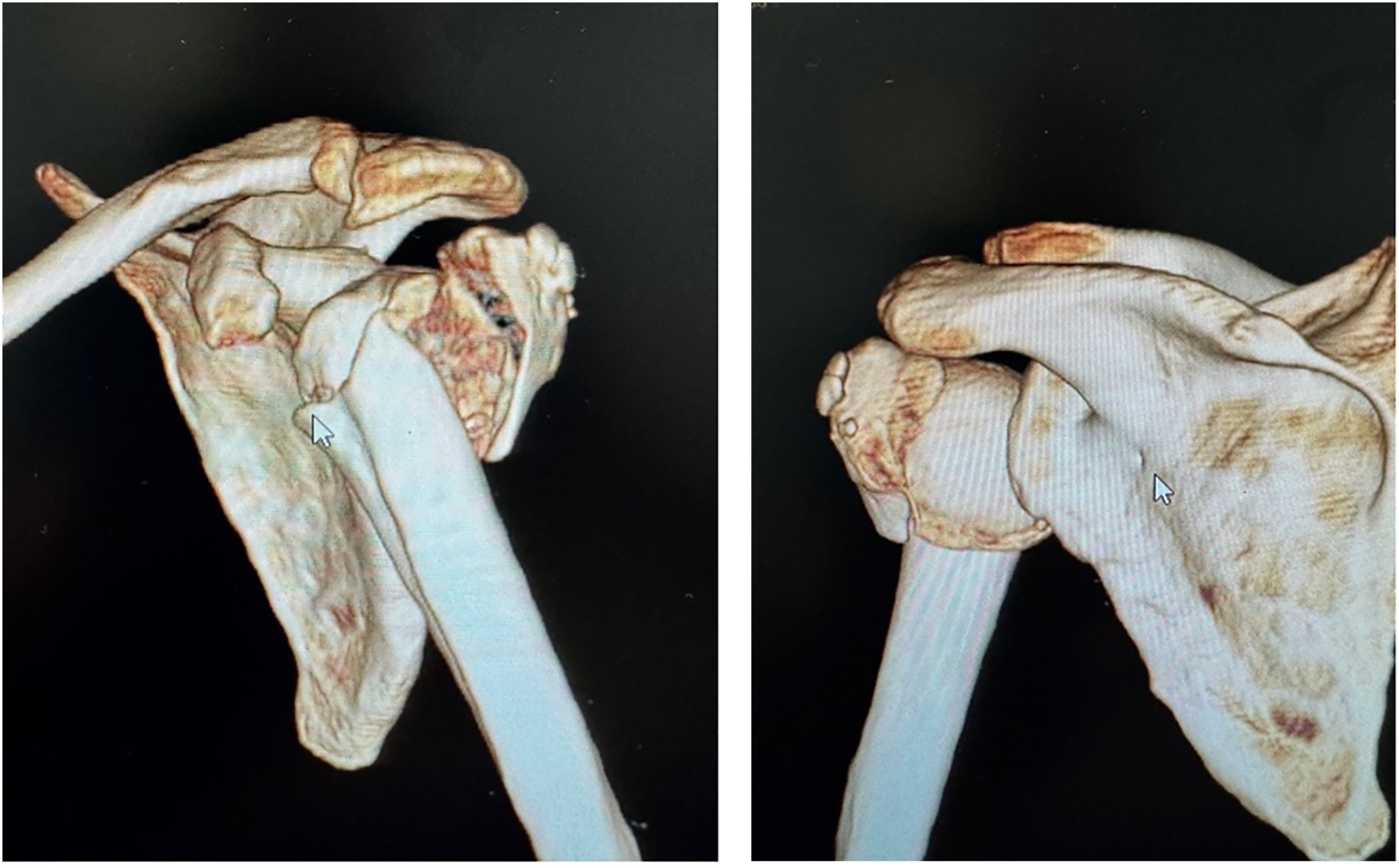
3D reconstruction of Neer four-part proximal humerus fracture.
Surgical Treatment
Patients who underwent reverse shoulder arthroplasty received surgery within seven days of their traumatic injury. The procedure adhered to a standardized protocol conducted by the same surgeon across five different centers over a two-year span. Patients were placed under general anesthesia and positioned in a modified beach chair stance. As part of prophylactic measures, systemic antibiotics (intravenous cefazolin, 2g, and Vancomycin, 1g) were administered. Surgical approaches included deltopectoral and superolateral methods, and procedures such as biceps tenotomy or tenodesis to the upper pectoralis major insertion were performed using absorbable sutures. Standard practices involved glenoid exposure, circumferential glenoid capsular release, minimal cartilage reaming, and the fixation of glenoid baseplates with 2-4 locked screws. A size 36 glenosphere was chosen for all cases and secured to the baseplate according to the manufacturer's instructions. To restore humeral height, reference points included the medial calcar and upper edge of the pectoralis major muscle insertions. 25 Retroversion of 20° was reestablished using an alignment rod, and the bicipital groove served as a guide for tuberosity repositioning. Four holes were drilled into the proximal diaphysis with a 2.5-mm drill bit, and four non-absorbable Ethibond #5 sutures were inserted in double strands for vertical fixation. Humeral stems were non-cemented and secured with two screws. Local horseshoe and morselized bone graft from the humeral head were placed at the stem metaphyseal region and between the tuberosities. Standard polyethylene inserts were utilized across all cases. The greater tuberosity was reattached in a horizontal manner using 4-6 non-absorbable Ethibond #5 sutures at the remaining cuff and bone interface, along with two vertical shaft sutures for each tuberosity. The lesser tuberosity underwent a similar repair process, with two additional horizontal sutures applied around the entire construct at the top and bottom of the tuberosities to enhance compression. To prevent excessive tension on the GT, the supraspinatus tendon was resected in all cases.
Following the surgery, all patients were prescribed six weeks of postoperative immobilization using an arm sling. During this period, patients were actively encouraged to engage in wrist and elbow movements. Subsequently, weeks 7 through 12 involved a gradual transition to a combination of passive and active-assisted range of motion exercises, alongside peri-scapular strengthening routines. At week 13, patients commenced a full active range of motion exercises and exercises targeting deltoid strengthening. The assessment of complications encompassed an evaluation for potential issues such as infection, dislocation, tuberosity displacement, hematomas, nerve damage, loosening, and scapular notching.
Results
Complications and Revisions
A major complication was reported in one patient who sustained an acromial stress fracture and was managed nonoperatively with modest clinical results. None of the patients needed revision in this cohort. There were no related complications to the locking screws.
Clinical Results
The 40 patients had a mean age of 78 years. These consisted of 40 females. At the follow-up of 24 months, the mean CMS was 80 points. The greater tuberosity healed in anatomic position in 90% of the cases (N = 36), obtaining an average CMS of 80 in these patients. Healing of the greater tuberosity did not occur in 10% of the cases (N = 4), obtaining an average CMS of 60. The difference in CMS scores between the two groups was significantly different (P < .05). Overall, the mean active anterior elevation reached 142°, the mean active external rotation with the arm at the side was 30°, and the mean internal rotation was L5. Of the 40 patients treated with reverse shoulder arthroplasty for comminuted 3-4 part fractures, 19 were highly satisfied, 10 were satisfied and 1 was not. The VAS scores at 1 year were a mean of 1.5.
Radiologic Results
Healed GT was found in 90% of cases (Figure 4). At 24 months, less than 1% of patients had grade 3-4 scapular notching.

Healed Greater Tuberosity.
Discussion
As indicated by Court-Brown et al, 6 the incidence of fractures in the proximal humerus is anticipated to rise in the upcoming years among older individuals. This demographic faces a range of challenges, including reduced bone quality, tuberosity fractures, complications associated with surgical interventions, subsequent complications of fractures, and the impact of the patient's cognitive condition during the recovery phase.26–28 Recent trends in the management of complex humeral fractures, particularly in elderly patients, have observed an increased preference for reverse shoulder arthroplasty. 19 Furthermore, if the trauma case involves a more intricate Neer 3-4 part fracture, RSA is recommended. 29
This retrospective case series involving 40 female patients analyzed the clinical and radiographic outcomes on Neer 3–4–part fractures treated with RSA using an uncemented locked stem. At the short-term follow-up, lasting 24 months, it revealed a favorable correlation between greater tuberosity suture repair, bone grafting, and enhanced functional outcomes with improved external rotation with the use of fracture-specific locking stem.
It has been suggested that RSA should be the primary treatment approach for individuals aged 65 and above, due to its improved clinical reliability in contrast to hemiarthroplasty and its potential to expedite recovery in this specific population.20,30–33 RSA has traditionally been employed in cases of fractures with tuberosity excision and it has been linked to suboptimal healing due to ineffective compression when using non-fracture-specific stems with a bulky metaphysis.29,34–36 However, absence of tuberosities can reduce the stabilizing effect of the rotator cuff and deltoid on the reverse construct. 37 Gallinet et al 38 were among the first to highlight a change in outcomes when salvaging of the tuberosities was pursued. Concordantly, this case series reported an 90% healing rate for the greater tuberosity, attributed to the use of a specialized uncemented fracture stem with proximal coating, a low-profile metaphysis, a suture-friendly groove, a meticulous suture technique, and the use of local bone graft (Figure 5). Moreover, to enhance the likelihood of healing without raising the risk of stiffness, it was advised to immobilize the affected area with a sling for 6 weeks. 39

Locked stem reverse total shoulder arthroplasty.
The achieved active range of motion following prosthesis fixation and healing has enabled the resumption of daily activities for all patients. Despite reports of complication rates reaching up to 21% in reverse shoulder arthroplasty when use as a treatment method for proximal humeral fractures, this cohort exhibits a notably lower complication rate of 2.5%. 22 This improvement can be attributed to advancements in technique, technological developments, the exponential growth of knowledge in recent years, and a reduced risk of infection and prosthesis instability.40,41 The latter is due to the healing of greater tuberosity, the decreased rate of proximal bone loss, and tuberosity salvage in the studied population.42,43 Although proximal bone loss, including nonhealing or excision of the tuberosity, increases the risk of prosthesis instability and infections, no evidence of such an association was found in this cohort. 43 While periprosthetic infection after reverse shoulder arthroplasty was not observed in this series, up to a 24% incidence has been reported in patients with complex humeral fractures treated with RSA and a 4% incidence using locking plate fixation.44,45 Nonetheless, complication rates in this cohort remained low, and scapular notching was negligible at one year. Lastly, despite age being identified as an independent risk factor for complications after reverse shoulder replacement, it did not pose a problem in this cohort. 16
The locking system can be beneficial when stem fixation is compromised by bone quality or anatomy, or when press-fit fixation is not feasible due to diaphyseal instability. 46 As established by Jorge-Mora et al, 47 extramedullary nailing of the stem facilitated easy adjustments during surgery and enhanced prosthesis stability. This system eliminated the need for cement, reducing the likelihood of cement-associated complications, and allowed trial reductions to achieve optimal humeral height, and range of motion.
Mean active anterior elevation reached 142°, mean active external rotation with the arm at the side was 30°, and mean internal rotation was L5. The greater tuberosity healing group exhibited increased external rotation, a mean of 18 degrees more than the non-healing group. Furthermore, patients with greater tuberosity healing had better overall outcomes compared to those with unsuccessful healing. The mean LSA and DSA, initially reported in primary cases, correlated with function, and in cases where the greater tuberosity healed, both were within parameters associated with good shoulder function. 48
This study may pose certain limitations as it is considered a retrospective
Conclusion
Reverse shoulder arthroplasty improves clinical outcomes in the elderly population with proximal humerus fractures. Every effort to conserve the tuberosity and ensure its healing should be attempted, including utilizing a strong suture technique and local bone grafting, as it positively influences clinical outcomes and external rotation. The use of an uncemented locked stem demonstrated safety and reliability for this procedure. 49
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.