
Abstract
Background
The assessment of tuberosity position and union in reverse shoulder arthroplasty (RSA) for complex proximal humerus fractures (PHF) has been carried out by means of routine simple radiographs. To evaluate the interobserver agreement and intraobserver reproducibility of the simple radiograph in comparison to the CT scan.
Methods
The position and consolidation of the tuberosities in 2 radiographic projections and in a CT scan of 32 consecutive patients operated on a RSA for PHF was assessed by 5 observers. Interobserver agreement and intraobserver reproducibility in both imaging tests were also assessed.
Results
The interobserver agreement for the greater tuberosity position was 0.52 in the simple radiograph and 0.45 in the CT scan. For the greater tuberosity union, agreement was moderate in the simple radiograph (0.52), but fair in the CT scan (0.35). For the lesser tuberosity position and union, the agreement was fair in the radiograph and poor in the CT scan.
Conclusion
Only moderate agreement was observed in the assessment of the position and union of the tuberosities in the RSA for PHF in the simple radiograph and no improvement in it was seen for the 2D CT scan.
Introduction
Since the introduction of the reverse shoulder arthroplasty (RSA) for the treatment of degenerative glenohumeral arthropathy secondary to rotator cuff injury, its indications have been extended in the last decade to other pathologies. Mainly, the indications have broadened to include complex acute fractures of the proximal humerus (PHF) in the elderly patient.1–5 The poor results obtained with hemiarthroplasty due to comorbidities, comminution of the tuberosities and poor bone quality that lead to migration, resorption or non-union have contributed to extending its use.6–11 A more reproducible technique and more predictable functional results, theoretically related to a lesser influence of tuberosity consolidation on the functional results of the RSA, has produced a change in the surgical indication.5,12–15
Just as in hemiarthroplasty, consolidation of the tuberosities in the correct position is essential to obtaining good functional results.6,7 This premise presents controversial results in RSA. Some recent publications have reported an improvement in functional results, especially in terms of forward elevation and external rotation if we achieve an anatomical union of the greater tuberosity as well as to an influence on the stability of the prosthesis.16–24 Others have reported that the tuberosity position has no influence on the functional outcomes.10,25–28
The anatomical union rates of the greater tuberosity range from 37% to 84% in the literature,23,26 being assessed in most studies with simple radiography. Few studies use the CT scan to confirm this parameter.17,23,25 To date, no study has analyzed the reliability of this assessment.
The question is whether the radiographic assessment of the tuberosity position and union in the RSA for PHF is reliable and thus useful for the correlation with the functional results as well as which is the most efficient radiological study. As CT scan add cost and radiation exposure to the patient its need must be supported.
The objective of the study was to analyze the reliability of the assessment of the position and union of the tuberosities by means of simple radiography in comparison to 2D CT scan of patients operated on for a complex fracture of the proximal humerus using a RSA.
Material and Methods
A prospective study was carried out that included all the patients who had undergone an RSA for an acute 3- or 4-part PHF, with or without dislocation, from March 2015 to December 2018. Patients older than 65 who had been operated on within 3 weeks of the fracture, with a minimum follow-up of 1 year, were included. Patients with an acute neurovascular injury, fractures with a diaphyseal extension, a pathological fracture, and those with a history of surgery on the affected shoulder were excluded. The inclusion criteria for the study gathered 32 patients. All the patients agreed to participate in the study and signed informed consent. The study was approved by the ethical committee (Ref. # CEIC Pl-19-049).
It consisted of 27 women and 5 men with a mean age of 75.21 years (65-87). Using Neer's classification with plain radiography and preoperative CT scan, 12 were 3-part fractures, 18 were 4-part, and 2 were 4-part fracture-dislocations. The mean follow-up time was 53 months (24-113 months).
Surgical Technique
All patients underwent a deltopectoral approach and tenodesis of the long head of the biceps. After removal of the humeral head, both tuberosities are provisionally identified and isolated. The glenoid was prepared and the metaglene was placed right next to its lower margin in neutral tilt. The size of the glenosphere was decided depending on the surgeon's preference for each case. In all cases, a cemented medialized reverse prosthesis of the same model (DeltaXtendTM DePuy, Warsaw, Indiana, USA) was put in place in zero-degree retroversion. For the reinsertion of the tuberosities, a configuration was made with 6 non-absorbable sutures (No. 5 Ethibond, Somerville, New Jersey, USA). There were 2 diaphyseal sutures anterior to the bicipital groove that were fixed to the tendon of the infraspinatus and teres minor for reinsertion of the greater tuberosity. Then, 2 posterior diaphyseal sutures to the bicipital groove were fixed to the subscapularis tendon for lesser tuberosity reattachment and there were 2 circumferential sutures between the tuberosities. 29 In all cases, the supraspinatus was resected. No additional graft was used due to the characteristics of the conventional stem used. All the surgeries were performed jointly by 2 shoulder surgeons. Postoperatively, a sling was emplaced for 2 weeks with elbow and pendulum exercises allowed 2 times per day. From 2 to 4 weeks, passive mobilization and self-assisted elevation was performed and the patient began with active movements and rotations from 6 weeks onward. Rehabilitation was carried out in all cases in a group program managed by the hospital's rehabilitation unit.
Radiological Evaluation
Plain radiographs and a CT scan were performed once the patient agreed to participate in the study.
Plain radiographs of the shoulder were taken in the neutral and internal rotation anteroposterior views. CT assessment was performed on the same day with a 2D reconstruction software program (Alma workstation). The radiological study was agreed and supervised by 2 musculoskeletal radiologists.
Once the images were obtained, 5 observers that included 2 orthopedic surgeons specialized in shoulder pathology, 2 radiologists specialized in musculoskeletal pathology, and a fourth-year resident of orthopedic surgery and trauma assessed the position and union of the tuberosities by both means in 2 successive readings at 4 weeks apart. At 3 months, the observers repeated the procedure with the cases in a randomized order. A detailed definition of the variables to be observed is mandatory in reliability studies to minimize misinterpretations. So the variables to be analyzed were previously agreed upon in a joint meeting of all the observers. After that each observer took the readings independently.
In the radiological evaluation, the presence or not of each of the tuberosities, their position, and continuity or not with the diaphysis was determined in each projection.
Simple Radiology
The greater tuberosity was considered to be in an anatomical position if the top was at the level of the epiphysis of the stem or slightly above it at the level of the polyethylene in the anteroposterior view in neutral rotation and it was not visible in internal rotation as defined by Torrens et al 25 (Figure 1(A)). It was considered displaced, when it was raised in neutral rotation, defined in an arbitrary way as 1 cm above the anatomical position and visible in internal rotation and therefore in a posterior situation Figure 1(B). When it was not observed in either of the 2 projections, it was considered resorbed. If there was continuity with the diaphysis in any of the radiological views, the union was considered consolidated.

(A) An anteroposterior radiograph in neutral rotation and internal rotation where the greater tuberosity is seen in an anatomical position and united. The greater tuberosity is seen in the correct position in the neutral rotation view and is not observed in the internal rotation view. (B) Anteroposterior radiograph in neutral rotation and in internal rotation where the greater tuberosity is seen displaced posteriorly and not united.
For the lesser tuberosity, a correct position was considered achieved if it was not visible in the anteroposterior view in neutral rotation and was present in the view in internal rotation. It was out of place when it was observed medially in either of the 2 projections and resorbed when not observed in either view.
There was union if there was continuity with the diaphysis in any of the radiological views.
CT Scan
To assess the CT scan, a multiplanar MPR reconstruction was performed. On the axial plane, the fins of the humeral stem of the prosthetic model used were taken as a reference to determine the position of the tuberosity and control a possible the rotation of the arm during the exam.
Thus, in the axial section, the greater tuberosity was considered to be in an anatomical position if it was in an anterolateral position, that is if the most anterior cortex of the tuberosity was between the anterior fin of the stem and the anterior half of the hemisphere that forms the epiphysis (Figure 2(C) and (D)).

(A) and (B) Coronal and sagittal CT scan sections, showing the greater tuberosity healed at the level of the epiphysis of the stem or slightly above it at the level of the polyethylene. A: anterior. P: posterior. (C) The fins of the prostheses were used to control the rotation of the arm in the CT scan and identify the position of the tuberosity around the epiphysis of the stem in an axial section. (D) In a more superior axial section, an anterior cortex of the GT between the anterior fin and the anterior hemisphere was considered an anatomic position. If the more anterior cortex was observed posterior to the hemisphere, the GT was considered displaced. A: anterior P: posterior.
A posterolateral position, thus displaced, was also seen if the most anterior cortical was behind the equator of the hemisphere that forms the epiphysis.
Regarding the lesser tuberosity, an anatomical position was seen if it was just in front of the anterior fin or displaced if it was medial.
On the sagittal and coronal planes, the position of the tuberosities was assessed following the same criteria as in the plain radiography and whether or not there was continuity with the diaphysis to determine its consolidation (Figure 2(A) and (B)).
A tuberosity was considered reabsorbed when it was not visible on any plane.
Statistical Analysis
Interobserver agreement was calculated using Fleiss Kappa (K) statistics with 95% confidence intervals (CI). Kappa is a chance-corrected measure of agreement that considers agreement expected by chance alone. A K of 1 indicates perfect agreement, and a K of 0 indicates no more agreement than expected by chance alone. The categorization was performed using the criteria of Landis and Koch. 30 Less than 0.20 represents poor or slight agreement, 0.21 to 0.40 fair agreement, 0.41 to 0.60 moderate agreement, 0.61 to 0.80 good agreement, and 0.81 to 1 excellent agreement. Data analysis was performed in the R software environment (version 4.0.3; R Foundation for Statistical Computing; Vienna, Austria). All tests were 2-sided, assuming an alpha level of 0.05.
Results
The agreement obtained among all the observers was moderate for the position of the greater tuberosity in both tests even though there was a better degree of agreement with plain radiography. For the union of the greater tuberosity, agreement was moderate in the plain radiography and fair in the CT scan. Fair agreement was obtained for the position and consolidation of the lesser tuberosity in the plain radiography. In the CT scan, the agreement for the evaluation of the lesser tuberosity was poor. The results are expressed in Table 1.
Interobserver Kappa Coefficient Obtained for the Position and for the Union of Both Tuberosities in Each Imaging Test.

Abbreviations: GT, greater tuberosity; LT, lesser tuberosity; CI, confidence interval.
By specialties, the radiologists arrived at moderate agreement for the position of the greater tuberosity in the simple radiograph, while the agreement was good among the traumatologists. On the other hand, for the same variable in the CT scan, agreement was good among radiologists but fair among shoulder surgeons.
For the union of the greater tuberosity, the radiologists showed good agreement in both the plain radiography and computerized tomography. On the other hand, agreement was good in CT scan, but fair in simple radiograph among shoulder surgeons.
Agreement in the assessment of the lesser tuberosity was between fair and poor in both tests and in both specialties. Regarding lesser tuberosity union, radiologists obtained good agreement in simple radiography and, in contrast, the traumatologists showed a negligible agreement. The results are summarized in Table 2.
Interobserver Kappa Coefficient Obtained for the Position and for the Union of Each Tuberosity in Each Imaging Test by Specialties, 2 Specialists in Musculoskeletal Radiology, and 2 Trauma Specialists in Shoulder Pathology.
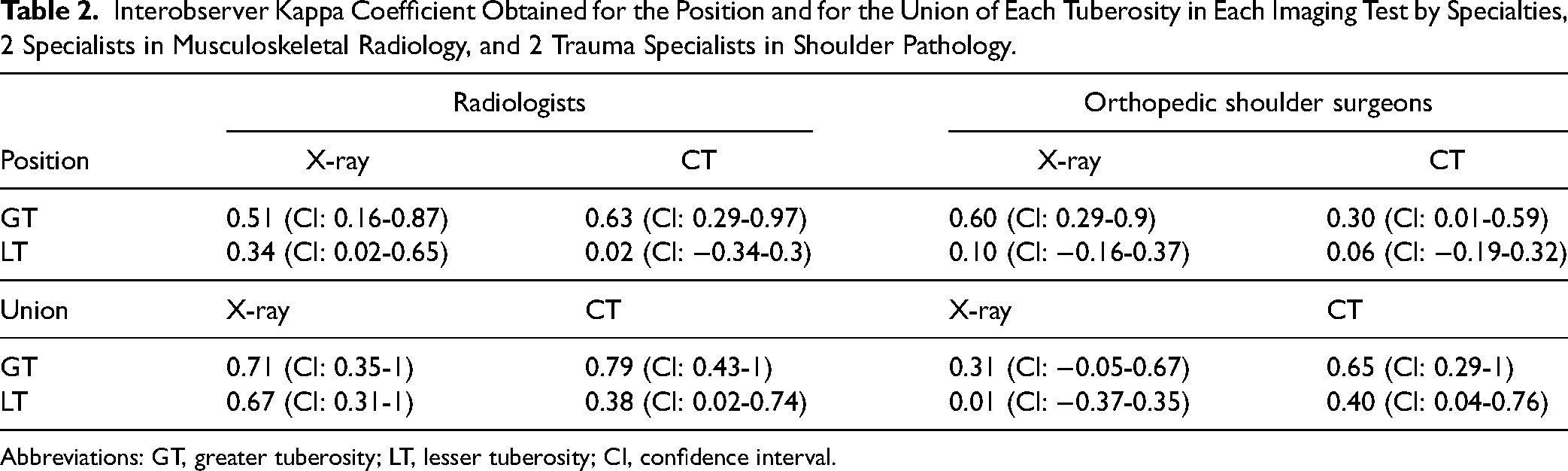
Abbreviations: GT, greater tuberosity; LT, lesser tuberosity; CI, confidence interval.
Intra-observer agreement was better for the position of the greater tuberosity in plain radiography than in computed tomography, regardless of the specialty. The results are summarized in Table 3.
Intraobserver Kappa Coefficient for the Position and Union of Each Tuberosity in Both Imaging Tests.

Abbreviations: GT, greater tuberosity; LT, lesser tuberosity; O, observer.
Discussion
Various publications have analyzed the influence of the position and union of the tuberosities on the functional results of the RSA in complex PHF. Due to the ability of RSA to provide functionality in patients with a defect in the rotator cuff, it has been understood that the reinsertion and subsequent union in an anatomical position of the tuberosities in FHP had less clinical relevance than in hemiarthroplasty.5,10,11,15,26,31
Although the effect on the stability of the prosthesis has been demonstrated in the series were no repair or excision of the tuberosities was performed,5,16,21 the influence on the functional results has not yet been determined.
In many published works on the subject, simple radiography is the technique of choice to assess the position and union of the tuberosities and correlate it with the functional results.
Our work proposes to assess whether the imaging tests used are reliable and can be used to study the correlation with the functional results. To date, the parameters have not been analyzed.
Only moderate agreement was obtained with the simple X-ray assessment. Therefore, this presents questions. Why is it that we only see moderate agreement and is the correlation we make with the functional results reliable?
There is great variability in the radiographic views used and the criteria to assess the anatomical or non-anatomical location of the tuberosities. Boileau et al 23 used routine anteroposterior and lateral views. Grubhofer 19 used standardized anteroposterior, axillary, and scapular lateral radiographs while Ohl et al 16 relied on one single anteroposterior view in the neutral position. Garofalo et al 22 used 4 different views, 2 true anteroposterior projections in internal rotation and in external rotation, the axillary projection and the Y of the scapula. Thus, the variability of images used can influence the results reported in the different studies, and there is a lack of consensus in the literature on which are the best radiographic views to use. As demonstrated in the intraobserver agreements obtained, the anteroposterior views in neutral and in internal rotation are reproducible for the position and union of the greater tuberosity. The anteroposterior projection in internal rotation is easy to perform and manage and we believe that it makes for better visualization of the proximal humerus than the outlet due to less overlap of the scapula.
Some authors assume that CT is the gold standard to assess whether the position in plain radiography is reliable.17,23,25 However, to date, the reliability of the CT scan for this assessment has not been analyzed either.
Boileau et al 23 assessed the position and consolidation of the tuberosities in routine postoperative control views and did a CT scan to confirm union in part of their patients. In the same sense, Torrens et al 25 did a CT scan in cases in which the tuberosity was displaced in plain radiography to locate its position. Recently, Gunst et al 17 assessed the influence of the tuberosities healing with CT scan and routine radiographs. The lower agreement values obtained with CT scan in our study reflect difficulties in the observation and interpretation of the fragments of the tuberosities in the images. Thus, the observation of the tuberosity fragment, especially when there is comminution, is not as easy as previously supposed. In our results, simple radiography has greater reliability than 2D CT scan in assessing the position and union of the greater tuberosity.
Another aspect to discuss is which criteria to consider in determining an anatomical or a displaced tuberosity. There is lack of consensus in the literature. Gallinet et al 21 has arbitrarily defined what is considered an anatomical position of the tuberosities following the criteria of Boileau et al 23 in the hemiarthroplasty. Ohl et al 16 take visualization on the lateral part of the stem or a maximum of 5 mm below it to be anatomical. Torrens et al 25 arbitrarily determined it to be anatomical when the greater tuberosity was at the level of the epiphysis of the humeral stem or at the level of the polyethylene in a medialized model, the definition used in our study. Thus, in addition to defining what the best imaging test is, a consensus is necessary as to what we consider an anatomical consolidation of the tuberosities to be able to analyze and homogenize our results. When we interpret the results, we must bear in mind that the tuberosity cannot be placed in its original position due to the biomechanics of the prosthesis, especially in medialized models. Therefore, the criteria would probably be different in medialized and lateralized models. Further studies will be necessary to better assess the tuberosity position in each model.
Regarding the lesser tuberosity, no previous work specifies how to perform the position assessment in either plain radiography or computerized tomography. The fair or slight agreement reached in all the related variables indicates great difficulty in their visualization and interpretation in both tests. It is probably due to size, previous comminution, and location that significantly complicate the assessment. Therefore, we advise to be cautious when we determine what influence the repair has on the results.
There are no previous reliability studies in the literature in this field. This fact does not make a comparison of our results possible. We know from studies carried out with Neer's classification that the use of CT along with the simple radiograph does not increase the agreement between observers in most of the published works.32–34
In some studies, it was suggested that the observer's experience can influence agreement. 32 Therefore, different experienced observers participated in our study. Also, prior training in the assessment variables was done to improve the agreement as demonstrated by Brorson et al. 35
Due to the results obtained, musculoskeletal radiology specialists obtained better degrees of agreement than shoulder surgeons, especially in the 2D CT scan. One of the difficulties involved in carrying out a radiological reading study is the influence that what one believes has happened, in anatomopathological terms, may have on the observer. It may induce one to make an interpretation rather than an observation. This would explain the differences between musculoskeletal radiology specialists and shoulder surgeons.
To our knowledge, this is the first study that analyzes the reliability of the assessment of the position and union of the tuberosities in the RSA for a PHF. Our main strengths are the controlled radiographic view execution, the comparison with the 2D CT scan, the different level of experience of the observers, and the consensus about the anatomical and displaced position reached previously among the observers. The number of patients included could be a limitation as the minimum number of patients included in reliability studies needs to know the prevalence of the event under study.
Conclusions
Only moderate agreement was obtained for the position and union of the greater tuberosity in the RSA for PHF with the simple radiography, thus its influence and correlation with the functional results obtained must be taken in caution. The assessment with a 2D CT scan does not improve the reliability thus it not seem to be more useful to assess this correlation. Given the poor agreement obtained in the evaluation of the lesser tuberosity in both tests, the functional results in relation to the position and consolidation of the lesser tuberosity are not reliable. A standardized radiological projection and a consensus about the anatomical position of the tuberosities would be desirable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Hospital Germans Trias i Pujol ethical commitee with the number REF CEI pl19-049.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.