
Abstract
Introduction
The most common surgical options for geriatric proximal humerus fractures are open reduction and internal fixation (ORIF), hemiarthroplasty (HA), and reverse total shoulder arthroplasty. We used a longitudinal inpatient discharge database to determine the cumulative incidence of conversion to arthroplasty after ORIF of geriatric proximal humerus fractures. The rates of short-term complications and all-cause reoperation were also compared.
Patients and Methods
All patients 65 or older who sustained a proximal humerus fracture and underwent either ORIF, HA, or shoulder arthroplasty (SA) as an inpatient from 2000 through 2017 were identified. Survival analysis was performed with ORIF conversion to arthroplasty and all-cause reoperation as the endpoints of interest. Rates of 30-day readmission and short-term complications were compared. Trends in procedure choice and outcomes over the study period were analyzed.
Results
A total of 27 102 geriatric patients that underwent inpatient surgical management of proximal humerus fractures were identified. Among geriatric patients undergoing ORIF, the cumulative incidence of conversion to arthroplasty within 10 years was 8.2%. The 10-year cumulative incidence of all-cause reoperation was 12.1% for ORIF patients and less than 4% for both HA and SA patients. Female sex was associated with increased risk of ORIF conversion and younger age was associated with higher all-cause reoperation. ORIF was associated with higher 30-day readmission and short-term complication rates. Over the study period, the proportion of patients treated with ORIF or SA increased while the proportion of patients treated with HA decreased. Short-term complication rates were similar between arthroplasty and ORIF patients in the later cohort (2015-2017).
Conclusion
The 10-year cumulative incidence of conversion to arthroplasty for geriatric patients undergoing proximal humerus ORIF as an inpatient was found to be 8.2%. All-cause reoperations, short-term complications, and 30-day readmissions were all significantly lower among patients undergoing arthroplasty, but the difference in complication rate between arthroplasty and ORIF was attenuated in more recent years. Younger age was a risk factor for reoperation and female sex was associated with increased risk of requiring conversion to arthroplasty after ORIF.
Keywords
Highlights
The 10-year cumulative incidence of conversion to arthroplasty for inpatient geriatric patients undergoing proximal humerus open reduction and internal fixation (ORIF) was around 8%.
Geriatric proximal humerus fractures treated with hemiarthroplasty or shoulder arthroplasty had lower all-cause reoperation rates than those treated with ORIF.
Younger age was a risk factor for reoperation and female sex was associated with increased risk of requiring conversion to arthroplasty after ORIF.
Introduction
Proximal humerus fractures (PHFs) represent the third most common fracture in patients older than 65. 1 Roughly 80% of these injuries are managed nonoperatively, 2 but surgical management with either open reduction internal fixation (ORIF), hemiarthroplasty (HA), or reverse total shoulder arthroplasty (RTSA) is indicated for displaced and complex fracture patterns. 3 As the geriatric population continues to expand in the United States, 4 the societal burden associated with treating these injuries is expected to grow.
Operative management of these injuries in geriatric patients is challenging due to poor bone quality and a high rate of concurrent medical comorbidities. 5 ORIF, the gold standard in young active adults, confers the benefit of preserving bone stock but has been associated with high rates of screw cut-out.6,7 RTSA has surpassed hemiarthroplasty as the treatment of choice for 3 to 4 part fractures, head-split fractures, or fractures with significantly greater tuberosity comminution.8,9 Its use was initially limited to elderly and low-demand patients, but recent short-term studies have described promising functional outcomes as well.6,10 In addition, primary arthroplasty may offer the secondary advantage of eliminating the risk of needing a second surgery to convert an ORIF to arthroplasty. However, while single-center studies have reported on reoperation rates for elderly patients undergoing ORIF,5,11 it remains uncertain what proportion of these reoperations are salvage procedures to convert to shoulder arthroplasty versus revision fixation or hardware removal.
This study aims to use a longitudinal state-wide inpatient database to analyze the long-term risk of conversion to shoulder arthroplasty after ORIF of geriatric proximal humerus fractures and to compare the long-term reoperation free survival rates of ORIF, hemiarthroplasty, and shoulder arthroplasty in this population. We also aimed to define patient-specific risk factors associated with 30-day readmission, short-term complications, and reoperation.
Patients and Methods
Study Cohort
The California Office of Statewide Health Planning and Development (OSHPD) Patient Discharge Database (PDD) is a mandatory discharge database that includes all inpatient admissions in the state of California, and was used to identify patients for this study. This database includes hospital characteristics, patient demographic data, diagnosis and procedure codes, patient comorbidities, and length of stay. Furthermore, each patient in the PDD is assigned a unique identification number that remains constant for all subsequent encounters, allowing for longitudinal tracking for any postoperative readmissions that take place within the state of California. Institutional Review Board approval was obtained for this study.
All patients 65 years of age or older with a diagnosis of a proximal humerus fracture that underwent either ORIF, HA, total shoulder arthroplasty (TSA), or RTSA between January 1, 2000, and December 31, 2017, were included. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis and procedure codes were used to identify cases prior to December 2014 and the ICD-10-CM was used to identify all cases after December 2014. As the ICD-9-CM procedure codes do not distinguish between RTSA and TSA, patients undergoing either procedure were analyzed together as patients undergoing shoulder arthroplasty (SA). All pathologic fractures were excluded from the analysis.
The primary long-term outcomes of interest were the conversion of ORIF to arthroplasty and all-cause reoperation. To meet the criteria for conversion, ORIF patients were required to present for a subsequent inpatient encounter with (1) a diagnosis code for ORIF failure, (2) a procedure code for internal fixation removal, and (3) a procedure code for shoulder arthroplasty. All-cause reoperation included implant removal, revision ORIF, conversion of ORIF to arthroplasty, revision of prior arthroplasty, conversion of hemiarthroplasty, ORIF of periprosthetic fracture, or implant removal. To meet the criteria for all-cause reoperation, patients must have presented for a subsequent encounter with a diagnosis code for ORIF, HA, or SA failure AND a procedure code for revision ORIF, implant removal, or SA revision.
Secondary outcomes included length of stay, 30-day all-cause readmission, and major short-term complications, which were adapted from the 2021 Centers for Medicare and Medicaid Services (CMS) Complication Measure Updates and Specifications for total joint replacement. 12 Short-term complications included readmission for hardware complication, infection, arthritis, loosening, osteolysis, or periprosthetic fracture or dislocation. See Supplemental Appendix 1 for a list of specific ICD-9-CM and ICD-10-CM codes used to define inclusion criteria, treatment failure, conversion, and revision.
Statistical Analysis
Patient demographics (age, sex, race/ethnicity, insurance status, obesity, diabetes, and other comorbidities) and short-term outcomes were summarized and compared between treatment cohorts. The overall study period was divided into 4 time periods and the proportion of cases treated with each procedure during each time period was reported. Subgroup analysis comparing demographics and outcomes between the early (2000-2004) and late (2015-2017) cohorts was performed for patients that underwent ORIF or SA. Multivariate analysis with logistic regression was performed to identify risk factors for 30-day readmission and major short-term complications. Regression results were reported as odds ratios (ORs) with 95% confidence intervals (CIs) and P-values.
Kaplan–Meier survivorship curves were generated to estimate 10-year conversion-free survival in all geriatric PHF ORIF patients. Multivariate Cox proportional hazards models including hospital and patient characteristics were performed to identify risk factors for ORIF conversion to arthroplasty.
Next, Kaplan–Meier survivorship curves were generated to estimate 10-year all-cause reoperation-free survival in geriatric patients who underwent ORIF, HA, or SA for proximal humerus fractures. Multivariate Cox proportional hazards models including hospital and patient characteristics were performed to identify risk factors for all-cause reoperation. In all analyses, age was included as a continuous variable.
Chi-squared tests were used to analyze categorical variables. Using the Shapiro-Wilks test, all continuous variables were found to be nonparametric, hence the Wilcoxon rank-sum test was used for comparisons between continuous variables. Statistical significance was defined as P < .05. All statistical analyses were performed with Stata 12.0 software (StataCorp LLC, College Station, TX).
Results
A total of 27 102 patients 65 years of age or older with proximal humerus fractures were identified between 2000 and 2017. Of these, 12 000 (44%) underwent ORIF, 6567 (24%) underwent hemiarthroplasty, and 8535 (31%) underwent shoulder arthroplasty. The proportion of patients undergoing hemiarthroplasty decreased from 31% to 12% over the study period while the proportion of patients undergoing SA increased from 32% to 40% and the proportion of patients undergoing ORIF increased from 38% to 48% (Figure 1). Overall, 81% of all patients were female, with the ORIF cohort having a slightly lower proportion of females than the HA and SA cohorts (78.1% vs 81.2% vs 82.3%, P < .001). A higher proportion of ORIF patients carried a diagnosis of cancer, chronic obstructive pulmonary disease, coronary atherosclerosis, or congestive heart failure, but there was no significant difference between treatment cohorts with respect to the total number of comorbidities. There were otherwise no clinically significant variations between treatment cohorts with respect to age, race, ethnicity, insurance status, obesity, or diabetic status (Table 1).

The proportion of proximal humerus fractures treated with hemiarthroplasty, shoulder arthroplasty, or open reduction and internal fixation (ORIF) over time.
Patient Demographics and Comorbidities.

Kaplan–Meier survival curves with the end point of ORIF conversion were generated (Figure 2). Among ORIF patients, the 10-year conversion-free survival rate was found to be 91.8%, corresponding to a cumulative incidence of 8.2%. Multivariate Cox proportional-hazards models revealed that male sex was associated with a lower risk of conversion to arthroplasty (HR 0.72, P = .038).
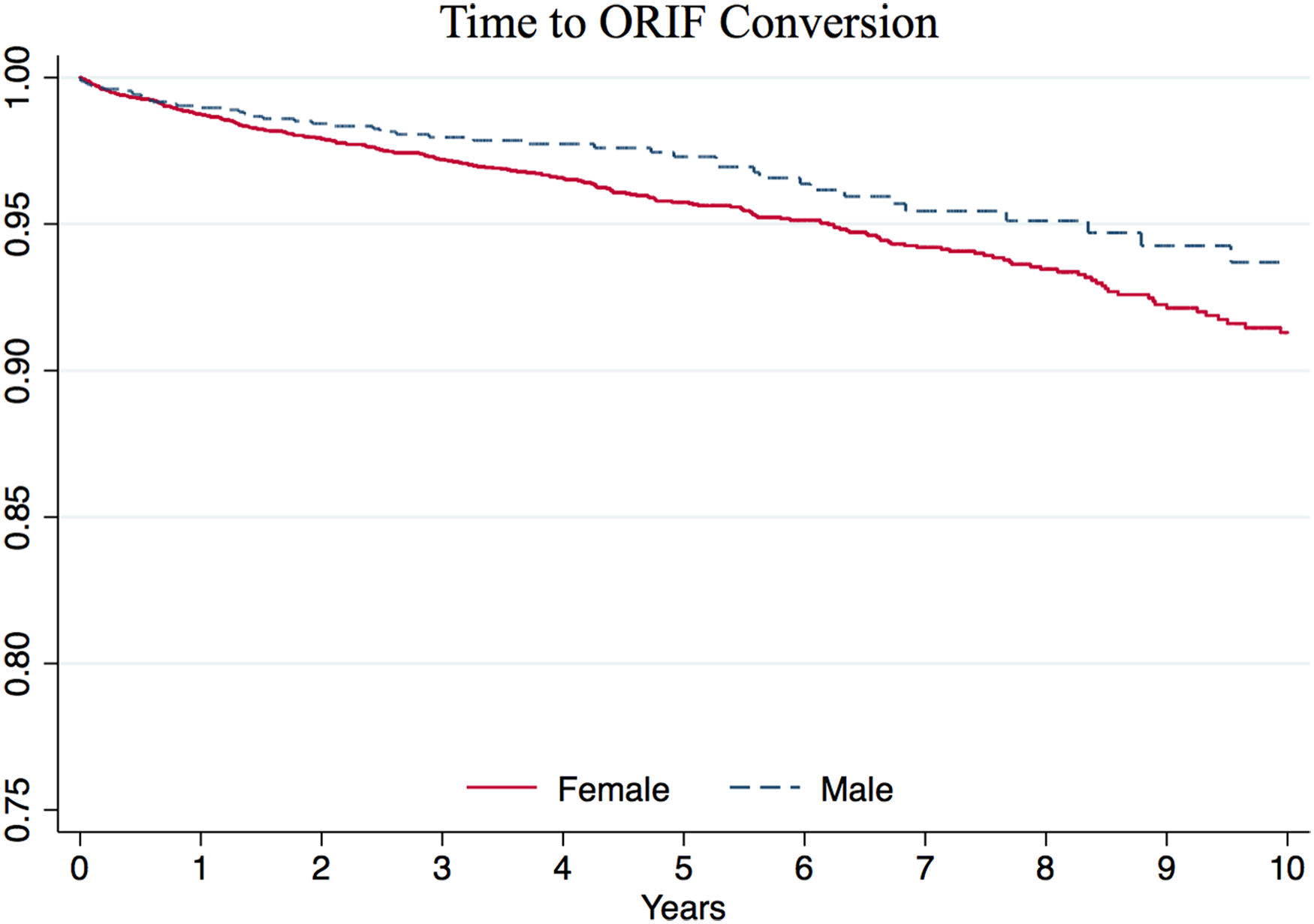
Kaplan–Meier survival curves with the end point of open reduction and internal fixation (ORIF) conversion to arthroplasty, stratified by sex.
Next, Kaplan–Meier survival curves with the end point of all-cause reoperation after ORIF, HA, or SA were generated, and stratified by procedure (Figure 3). Ten-year reoperation-free survival was found to be 87.9% for ORIF patients compared to 96.8% for HA patients and 96.2% for SA patients, corresponding to a cumulative incidence of 12.1%, 3.2%, and 3.8%, respectively. The multivariate Cox proportional-hazards model found that HA (HR 0.26, P < .001) and SA (HR 0.33, P < .001) were both associated with a lower risk of reoperation than ORIF. There was no significant difference in risk for reoperation between patients treated with SA versus HA (HR 1.24, P = .137). Other variables independently associated with a higher risk of reoperation included younger age (HR 0.98, P < .001), diabetes with vascular complications (HR 2.86, P = .005), and a higher number of comorbidities (HR 1.24, P < .001).
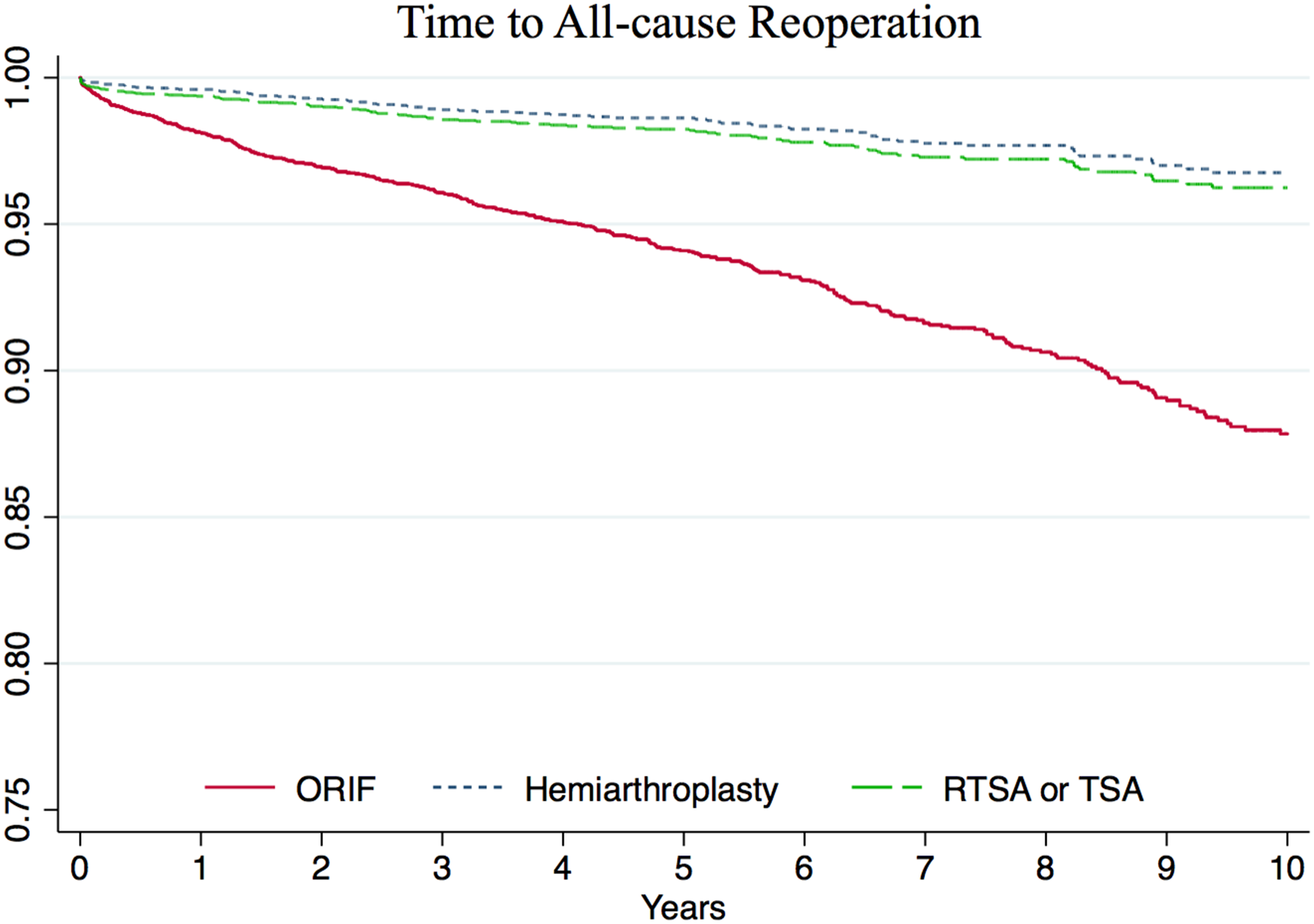
Kaplan–Meier survival curves with the end point of all-cause reoperation, stratified by the procedure.
SA patients had a marginally shorter length of stay than HA or ORIF patients (median 3 days for all procedures, mean 4.4 vs 4.7 vs 4.5 days, P < .001). Thirty-day readmission rates were significantly higher in ORIF patients compared to SA or HA patients (10.4% vs 8.1% or 8.4%, P < .001). The overall rate of major short-term complications was also significantly higher in ORIF patients compared to SA or HA patients (8.2% vs 6.7% or 6.5%, P < .001), with ORIF patients specifically having a higher rate of postoperative sepsis and mechanical complications (Table 2).
Outcomes and Complications.

Abbreviations: MI, myocardial infarction; PE, pulmonary embolism.
Multivariate logistic regression showed that SA was associated with a lower risk of 30-day readmission (OR 0.77, 95% confidence interval [CI] 0.70-0.85, P < .001) and lower risk of major short-term complications (OR 0.80, 95% CI 0.71-0.89, P < .001) when compared to ORIF. Compared to HA, SA was not significantly associated with an increased risk of either 30-day readmission (OR 0.95, P = .420) or major complications (OR 0.95, P = .456). Other significant risk factors for both 30-day readmission and major complications included older age, male sex, diabetes with vascular complications, and a higher number of preoperative comorbidities. See Supplemental Appendices 2 and 3 for full multivariate results.
Compared to patients in the early cohort (2000-2004), patients in the late cohort (2015-2017) that received either ORIF or SA demonstrated decreased complication rates (ORIF—6.3% vs 9.2%, P = .001; SA—5.1% vs 6.9%, P = .033) and decreased length of stay despite having higher rates of morbid obesity, congestive heart failure, or renal failure (Table 3). SA patients in the late cohort also had higher rates of osteoporosis and diabetes with vascular complications. On subgroup analysis limited to the late time period, treatment with SA instead of ORIF was associated with a lower length of stay and lower rates of 30-day readmission. There was no significant difference in the 30-day major complication rate.
Characteristics and Outcomes Between the Early and Late Time Periods.

Abbreviations: MI, myocardial infarction; PE, pulmonary embolism; ORIF, open reduction and internal fixation; COPD, chronic obstructive pulmonary disease; SA, shoulder arthroplasty.
*ORIF versus SA, 2015 to 2017 only.
Discussion
In this study, the 10-year cumulative incidence of conversion to arthroplasty for geriatric patients undergoing proximal humerus ORIF as an inpatient was found to be 8.2%. Overall 10-year all-cause reoperation rates were found to be 12.1% for ORIF patients and less than 4% for both HA and SA patients. Both hemiarthroplasty and shoulder arthroplasty patients had lower rates of 30-day readmission or short-term major complications than ORIF patients, although the difference in complication rate between arthroplasty and ORIF was attenuated in more recent years. Finally, during the 17-year study period, the proportion of patients treated with hemiarthroplasty decreased while the proportion treated with arthroplasty increased.
Our findings regarding long-term reoperation rates after proximal humerus fracture ORIF support evidence from existing smaller cohort studies. Out of 131 geriatric proximal humerus fractures treated with ORIF, Barlow et al reported an 11% reoperation rate at a mean 6-year follow-up. 5 In an age-matched comparison of geriatric PHF patients, Greiwe et al 10 found that 6 out of 25 patients in the ORIF group underwent reoperation (4 conversions, 1 revision, and 1 hardware removal) at mean 4-year follow-up compared to 0 patients in the RTSA group, despite a lower proportion of 3 to 4 part fractures in the ORIF cohort. Klug et al13,14 has published twice on their experience with RTSA versus locking-plate ORIF for complex proximal humerus fractures, reporting a 12% to 20% reoperation rate for ORIF patients compared to 3% to 5% in RTSA patients. Yahuaca et al 15 also reported far higher rates of reoperation in ORIF patients compared to RTSA, although their results were likely affected by including patients younger than 65 that were more likely to undergo fixation. Finally, Suroto combined the results of 6 studies in a systematic review and meta-analysis, reporting that RTSA had overall lower reoperation rates than ORIF when treating 3 or 4 part fractures. 16 Taken together, our study and the existing evidence suggest that in the appropriately selected patient, specifically elderly females, management with RTSA instead of ORIF may be preferential to minimize the risk of reoperation or conversion to arthroplasty. Older age was associated with a lower risk of reoperation across all treatment cohorts and females who underwent ORIF were found to have a higher risk of conversion to arthroplasty than males.
When evaluating short-term outcomes between treatment cohorts, HA and SA patients had similar rates of 30-day readmission and short-term major complications. Management with ORIF was associated with higher rates of both 30-day readmission and short-term major complications, with the most common complications being pneumonia (3.5%), mechanical complications (2.4%), and sepsis (1.6%). These findings are in line with Zhang et al, 17 whose State Inpatient Database (SID) study reported a similar overall 30-day readmission rate (8%) and a decreased readmission risk in hemiarthroplasty and shoulder arthroplasty patients compared to ORIF patients. They also found that mechanical complications were more common in ORIF patients. 17 In contrast, Cvetanovich et al 18 reported a higher rate of minor complications in hemiarthroplasty and shoulder arthroplasty patients compared to ORIF patients, largely driven by a higher rate of blood transfusion in arthroplasty patients, a metric that is not collected by OSHPD. Similar to existing literature,17–20 we found that older age, medical comorbidities, and severity of diabetes were independent risk factors for short-term major complications and readmission, irrespective of treatment type. Female sex, on the other hand, was found to be protective against short-term adverse outcomes. This finding echoes that of Ezuma et al, who used the National Surgical Quality Improvement Program database to compare complication rates after RTSA for PHF and found that males had a 2.4-fold risk of developing any 30-day complication and a 10-fold risk of 30-day reoperation. 21 Male sex has also been shown to be an independent risk factor for instability and dislocation, 22 re-admission, 23 and reoperation after RTSA. 24
Between 2000 and 2017, the proportion of patients treated with hemiarthroplasty dropped from 31% to 12%. Meanwhile, the proportion treated with primary arthroplasty increased from 32% to 40% and the proportion treated with ORIF increased from 38% to 48%. These numbers are consistent with previously reported trends both in the United States and abroad.8,25,26 The number of PHFs being treated with RTSA is rising, but ORIF remains the most common surgical option as of 2019, 25 likely reflecting the fact that RTSA has consistently demonstrated superior functional outcomes to HA. 27 Encouragingly, we found that short-term outcomes after both ORIF and SA improved over time, with patients in the later cohort (2015-2017) enjoying significantly lower complication rates and shorter length of stay. Complication rates were similar between ORIF and SA patients in the later cohort. While prior studies have demonstrated that the complication rate, operative time, transfusion rate, and length of stay after SA have improved in the last 2 decades, 28 our findings suggest that there have been similar improvements in the patient selection process, technique, or implants used for internal fixation.
As RTSA approaches ORIF as the most common surgical option for geriatric proximal humerus fractures, 9 it is important to keep certain limitations in mind. The long-term weight-bearing and activity restrictions after RTSA make it a less compelling option for active, high-demand individuals. 29 Young patients that undergo shoulder arthroplasty are also at a higher risk of revision. 30 While options for failed ORIF include revision ORIF or conversion to arthroplasty, which have demonstrated good to excellent clinical results,31,32 the sole option for a failed arthroplasty is a revision RTSA, which is more technically demanding and has been associated with comparatively worse outcomes.33,34 Infected shoulder arthroplasty is also a disastrous outcome that often requires a 2-stage revision and/or long-term antibiotics. 35 Hence, the lower rates of reoperation after shoulder arthroplasty may in part be due to surgeons’ reluctance to perform RTSA revision. Finally, RTSA continues to be associated with higher costs than ORIF.9,36
The strengths of this study include a sample size of 27 102 total patients and state-wide longitudinal follow-up, allowing for more accurate estimation of rare events such as conversion or reoperation. Single-center retrospective studies are limited by low numbers and loss to follow-up, and commonly used databases such as the National Inpatient Sample or National Surgical Quality Improvement Program fail to collect outcome data past initial hospitalization and 30 days, respectively. The OSHPD database, on the other hand, captures all readmissions and reoperations state-wide, even if they occurred at a different hospital than the index procedure.
Despite this, database research comes with significant limitations. First, we relied on ICD-9 and ICD-10 codes for inclusion criteria, cohort selection, injury characterization, and determination of outcomes of interest. Not only may inaccurate coding affect our results, 37 but these codes fail to capture information such as fracture severity and classification, presence of comminution, or bone quality. This information may affect decisions regarding treatment and introduces potential for heterogeneity between treatment cohorts with respect to injury characteristics. Furthermore, as ICD-9 procedure codes fail to distinguish between anatomic and reverse shoulder arthroplasty, we were unable to report exclusively on RTSA. Fortunately, the impact of this should be minimal, as anatomic TSA accounts for fewer than 5% of all arthroplasties performed for proximal humerus fractures. 38 Second, as with most database studies in the orthopedic literature, we cannot comment on functional outcomes, mobility, or patient satisfaction. Adverse events that do not result in reoperation such as superficial infection, delayed union, or malunion are also unable to be captured. Third, while OSHPD includes all inpatient admissions in California, it fails to capture surgeries that take place in an outpatient setting at ambulatory surgery centers. Due to this, our study is limited to index surgeries and reoperations that take place in an inpatient setting, meaning that this sample likely includes a patient population that is more frail with more comorbidities than the average patient undergoing proximal humerus fracture surgery. As demonstrated by Bovonratwet et al 39 and Mehta et al, 40 however, the majority of both proximal humerus ORIF and primary arthroplasties are still performed in the inpatient setting, with older patients having an even higher rate of requiring admission. Given this, our findings remain applicable to the majority of geriatric patients undergoing proximal humerus fracture surgery. Fourth, we lack information regarding surgeon specialty, surgeon skill, and surgical volume of the treating hospital, all of which may significantly impact surgical outcomes. Fifth, patients that move out of state are lost to follow-up, hence our long-term reoperation rates may be an underestimated. Finally, we do not report the indications for revision or conversion surgery and are unable to estimate the rate of specific long-term complications such as posttraumatic arthritis.
Conclusion
The 10-year cumulative incidence of conversion to arthroplasty for geriatric patients undergoing proximal humerus ORIF as an inpatient was found to be 8.2%. All-cause reoperations, short-term complications, and 30-day readmissions were all significantly lower among patients undergoing arthroplasty, but the difference in complication rate between arthroplasty and ORIF was attenuated in more recent years. Younger age was a risk factor for reoperation and female sex was associated with increased risk of requiring conversion to arthroplasty after ORIF.
Supplemental Material
sj-docx-1-sea-10.1177_24715492231192068 - Supplemental material for Short-Term Outcomes and Long-Term Implant Survival After Inpatient Surgical Management of Geriatric Proximal Humerus Fractures
Supplemental material, sj-docx-1-sea-10.1177_24715492231192068 for Short-Term Outcomes and Long-Term Implant Survival After Inpatient Surgical Management of Geriatric Proximal Humerus Fractures by Brendan Y Shi, Alexander Upfill-Brown, Shannon Y Wu, Rishi Trikha, Seth Ahlquist and Thomas J Kremen, Christopher Lee, Nelson F SooHoo in Journal of Shoulder and Elbow Arthroplasty
Supplemental Material
sj-docx-2-sea-10.1177_24715492231192068 - Supplemental material for Short-Term Outcomes and Long-Term Implant Survival After Inpatient Surgical Management of Geriatric Proximal Humerus Fractures
Supplemental material, sj-docx-2-sea-10.1177_24715492231192068 for Short-Term Outcomes and Long-Term Implant Survival After Inpatient Surgical Management of Geriatric Proximal Humerus Fractures by Brendan Y Shi, Alexander Upfill-Brown, Shannon Y Wu, Rishi Trikha, Seth Ahlquist and Thomas J Kremen, Christopher Lee, Nelson F SooHoo in Journal of Shoulder and Elbow Arthroplasty
Supplemental Material
sj-docx-3-sea-10.1177_24715492231192068 - Supplemental material for Short-Term Outcomes and Long-Term Implant Survival After Inpatient Surgical Management of Geriatric Proximal Humerus Fractures
Supplemental material, sj-docx-3-sea-10.1177_24715492231192068 for Short-Term Outcomes and Long-Term Implant Survival After Inpatient Surgical Management of Geriatric Proximal Humerus Fractures by Brendan Y Shi, Alexander Upfill-Brown, Shannon Y Wu, Rishi Trikha, Seth Ahlquist and Thomas J Kremen, Christopher Lee, Nelson F SooHoo in Journal of Shoulder and Elbow Arthroplasty
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was provided by the Committee for the Protection of Human Subjects (CPHS) of the Health and Human Services Agency of the State of California under assurance #00000681. Project Number 12-08-0614.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported in part by the H. H. Lee Research Program, Department of Orthopaedic Surgery, UCLA.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.