
Abstract
Introduction
in the elderly patient population, where fracture comminution, osteoporotic fractures, and associated arthritis or rotator cuff pathologies dominate, metadiaphyseal proximal humeral fracture is a challenging subset of fractures to treat. This study reports on cementless long-stem reverse total shoulder arthroplasty (RTSA) as primary treatment of metadiaphyseal proximal humeral fractures in elderly patients.
Materials & Methods
Between January 2018 and October 2021, 22 consecutive patients sustained proximal humerus fractures with metadiaphyseal extension and underwent surgery with cementless long-stem RTSA. Patients older than 60 years with minimum 1 year of clinical and radiographic follow-up were included. Patient demographics, range of motion, and patient reported outcomes [Visual Analog Scale (VAS) pain scale, Simple Shoulder Test (SST), Subjective Shoulder Value (SSV), and American Shoulder Elbow Surgeon (ASES) scores] were retrospectively collected. Postoperative X-rays were evaluated for fracture and tuberosity union.
Results
There were 14 eligible patients with a median age of 71 years (range 61-91 years) and a median 13 months follow-up. At final follow-up, the median active elevation was 120° (range 80°-150°), external rotation was 40° (range 0°-50°), and internal rotation was 40° (range 0°-80°). Median VAS was 2 (range 0-8), SST was 71% (range 33%-92%), SSV was 78% (range 20-90%), and ASES was 73 (range 17-90). All patients exhibited radiographic union. There were five minor complications in three patients: postoperative neuropathy, tuberosity nonunion, scapula notching, and proximal humeral stress shielding.
Conclusion
Cementless long-stem RTSA is a viable alternative to primary fracture fixation in the elderly patient population with metadiaphyseal proximal humerus fractures.
Keywords
Introduction
Proximal humerus fractures are a common cause of morbidity in the elderly population, accounting for 4% of all fractures. 1 Due to the low bone mineral density, 70% of these fractures occur in patients older than 60 years of age. 1 With our aging population, the incidence of proximal humerus fractures is increasing, 2 with an estimated tripling of fall-related proximal humerus fractures since 1970. 3 As orthopedic surgeons, our natural inclination is to restore the native anatomy via fracture osteosynthesis. However, in the elderly patient population, fracture comminution, osteoporosis fractures, and associated arthritis or rotator cuff pathologies dominate, which can preclude acceptable fracture alignment, stable surgical fixation, or restoration of pre-injury function.4–7
Recent literature suggests that patients over 65 years of age with proximal humeral fractures may benefit from arthroplasty procedures over open reduction internal fixation (ORIF).8–11 Reverse total shoulder arthroplasty (RTSA) has the mechanical advantage of an intramedullary load-sharing device for stabilizing fracture stability while maximizing deltoid function and compensating for rotator cuff dysfunction, a common pathology in geriatric patients. 12 As the elderly population grows with increases in life expectancy and arthroplasty techniques and implants continue to improve, RTSA will continue to become increasingly common.
A challenging subset of proximal humeral fractures has a prolonged fracture segment extending to the metadiaphyseal region. There is a paucity of literature evaluating the options of ORIF versus arthroplasty in the management of these patients. Robinson et al presented their series of 102 patients who were treated with long lateral locking plates with satisfactory outcomes. 13 Other authors utilized a unique spiral plate which lies proximal lateral and distal anterior for surgical stabilization. Although this is theorized to have the benefit of avoiding the deltoid insertion and neurovascular structures, the minimally invasive surgical technique can be technically challenging.14,15 On the other hand, RTSA for surgical treatment of these fractures has its unique set of challenges due to compromised bony fixation in the metaphyseal region, requiring longer prosthesis or cementation for increased stability. 16 Garofalo et al previously reported satisfactory results using cemented long-stem RTSA with cerclage wire for the treatment of these complex fractures with metaphyseal extension. 17
The purpose of this case series is to present the early clinical and radiologic outcomes of primary cementless long-stem RTSA for metadiaphyseal fractures in the elderly utilizing a contemporary, press-fit technique. The hypothesis is that cementless long-stem RTSA is a safe and effective method for the treatment of these complex fractures with high radiographic healing rates.
Material and Methods
From January 2018 to October 2021, 22 consecutive patients with metadiaphyseal proximal humeral fracture underwent treatment with cementless long-stem RTSA by three fellowship-trained shoulder surgeons. Inclusion criteria included elderly patients greater than 60 years old with proximal humeral fracture extending to the metadiaphyseal region with a minimum 1-year follow-up. Exclusion criteria included previous surgeries or complex fracture patterns with associated glenoid or scapula spine fractures. Fractures were termed “acute” if treated within 4 weeks of injury and “chronic” if treated more than 4 weeks from injury.
Electronic medical records were retrospectively reviewed to collect patient demographics including age, gender, body mass index (BMI), operated side, chronicity of fracture, fracture type, range of motion (ROM)—active elevation (AE), external rotation (ER), and internal rotation (IR); and patient reported outcomes—Visual Analog Scale (VAS) pain score, Simple Shoulder Test (SST), 18 SANE, and American Shoulder Elbow Surgeon (ASES). All patients had routine trauma series of shoulder radiographs, bilateral humeri AP views, and preoperative 3D CT scans. Patients underwent the same surgical approach, the same glenoid component, and one of two types of cementless, adjustable humeral stem (Adjustable or Revive Stem, Stryker, Kalamazoo, MI). From 2018 to June 2019, all patients were reconstructed with the Adjustable stem, which was available for commercial use since 2013 as a 155° inlay stem. The stem was designed with a hydroxyapatite-coated 90 mm distal press-fit stem component along with five variable spacer component lengths (15, 20, 25, 50, and 100 mm). The modularity is secured with morse taper and interlocking teeth between the components and a 5 mm internal set screw that has same length as the spacer component. From June 2019 onward, all patients were reconstructed with the newly released version of modular stem from the same company. This second stem was the Revive stem, designed as a 145° onlay platform stem with a modular tray, a hydroxyapatite-coated distal press-fit stem component with variable 90 mm, 130 mm, 170 mm, or 210 mm lengths, and a set of 20–30 mm spacers components that stack up to a maximum of 50 mm. The modularity is secured with interlocking teeth between the components and a 6 mm internal set screw that is the same length as the spacer component, which is maximally 50 mm. Both stems were available in 2 mm increments (9 mm, 11 mm, 13 mm, etc)
All patients were routinely followed up at 6 weeks, then at 3, 6, and 12 months, until fracture healing and satisfactory functional outcomes were achieved. Minimum 1 year of clinical and radiographic follow-up was selected, as such time period was deemed necessary to assess adequate bony healing.
Institutional Review Board approval was obtained. Retrospective chart review of all patients and radiographic analysis was performed. Implant subsidence, radiolucency, instability, fracture healing, and/or heterotopic ossifications were recorded.
Operative Technique
All surgeries were performed using a previously reported technique 17 with few modifications. Surgery is performed in a modified beach chair position via an extended deltopectoral approach. After exposing the humerus fracture, if the tuberosities are fractured, the tuberosities are tagged and later repaired similar to RTSA for proximal humeral fracture. 19 If the fracture does not involve the humeral epiphysis and tuberosities, the humeral head is osteotomized and the standard glenoid implantation technique is utilized.
The metadiaphyseal humeral shaft fracture is exposed and fracture reduction and cerclage fixation can be attempted at this time. In the majority of cases, there is significant comminution with multiple fragments complicating direct reduction (Figure 1); thus, the humeral prosthesis is utilized to aid in the reduction. The distal humeral segment is prepared, and a trial sounder is inserted to determine the appropriate implant size. The arm is then extended and the approximate length of the implant is selected. Comparative preoperative humeral radiographs can be measured to determine the ideal prosthetic length. At this step, the formal humeral stem is implanted to minimize repeated humeral trialing, which can further dilate the medullary canal and compromise ultimate implant stability. The formal prosthesis is now placed with the distal end of the prosthesis positioned about two canal diameters past the fracture site. With the formal implant impacted into position, fracture fragments are reduced around the implant via bone stitching (direct suturing through drill holes to reduce two fracture fragments) and circumferential cerclaging (circumferentially wrapping the fragments) (Figure 2). If the fracture segment is short, only suture cerclaging may be necessary. If the segment is long and extensile, metallic wires and/or strut allograft may be considered for augmentation (Figure 3). The joint is gently reduced to confirm the glenohumeral stability. Transosseous fixation of the subscapularis utilizing non-absorbable #2 suture or tuberosity osteosynthesis is performed if there is a separate tuberosity fracture. 20

Seventy-seven-year-old woman presenting with metadiaphyseal fracture involving tuberosity s/p fall. XR (A) and 3d CT (B) are shown.
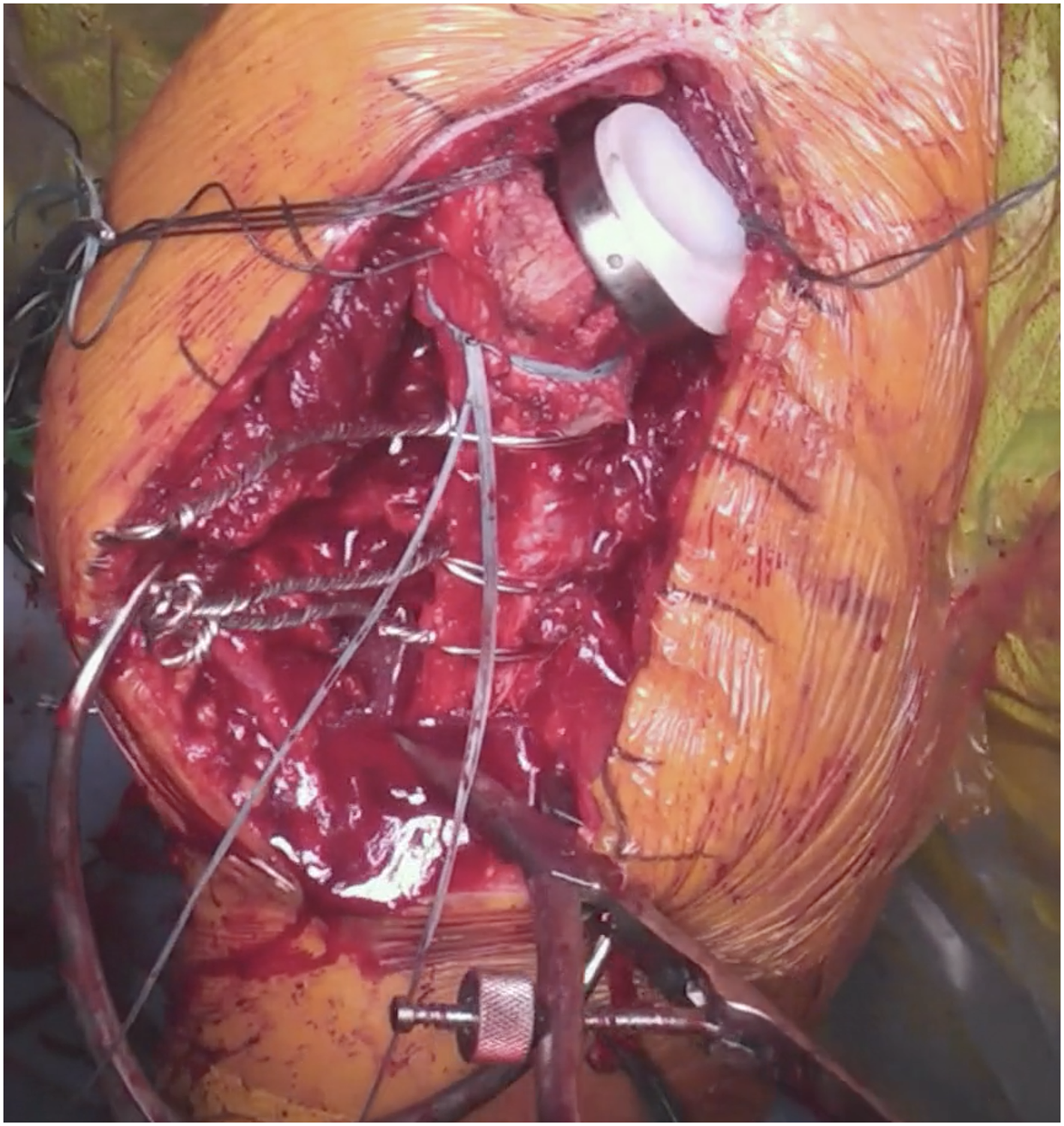
Intraoperative photo demonstrating bone stitching and cerclage suture to obtain interfragmentary compression.

Postoperative XR demonstrating surgical fixation with cementless press-fit long-stem RTSA with metaphyseal fragments cerclaged and augmented with tibial allograft strut.
Results
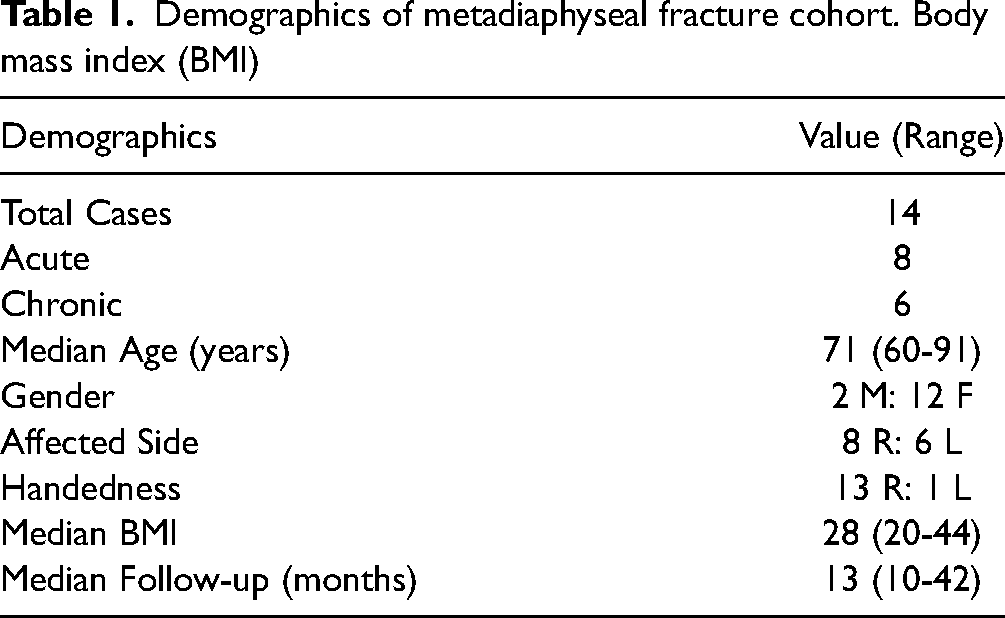
Detailed patient demographics are illustrated in Table 1. There were 14 patients eligible for follow-up during this study period; however, 7 patients were lost to follow-up and 1 was under 60 years of age. The remaining cohort had a median age of 71 years old (range 61-91 years). There were eight acute metadiaphyseal fractures and six chronic non-united fractures. Median duration of follow-up was 13 months (range 10-18 months).
Demographics of metadiaphyseal fracture cohort. Body mass index (BMI)
Median AE improved from 0° (range 0°-30°) to 120° (range 80°-150°), ER from 0° (range 0-10°) to 40° (range 0°-50°), and IR from 0° (range 0°) to 40° (range 0°-80°). Median VAS score improved from 9 (range 1-10) to 2 (range 0-8), SST score from 0% (range 0%-8%) to 71% (range 33%-92%), ASES score from 8 (range 0-45) to 73 (range 17-90), and SANE score from 15% (range 0%-40%) to 78% (range 20%-90%) (Table 2). On radiographic evaluation, all patients exhibited humeral shaft union (Figure 4). In seven patients who required additional tuberosity mobilization and osteosynthesis, five (71%) achieved tuberosity union.

Radiographs at 6-month follow-up demonstrating osteosynthesis and stable implant.
Patient functional outcomes before and after reverse total shoulder arthroplasty for metadiaphyseal fracture. Simple Shoulder Test (SST), Subjective Shoulder Value (SSV), American Shoulder Elbow Surgeon (ASES), active elevation (AE), external rotation (ER), internal rotation (IR).

Note: SST scores were calculated as a percentage of yes responses on the 12-item questionnaire.
No intraoperative or postoperative infections, postoperative instability, hardware loosening, or heterotopic ossification complications were encountered. There was one patient (7%) who had a recurrent fall postoperatively, leading to periprosthetic fracture distal to his fixation and required revision surgery. There were five other minor complications in three patients, all of which did not require revision surgery. These included postoperative neuropathy (2), tuberosity nonunion (1), scapula notching (1), and stress shielding (1). There were two patients who were deemed poor outcomes with functional scores less than 40. One of whom had greater tuberosity nonunion and axillary neuropathy and the other had recurrent trauma after surgery with neuropathic pain from cervical radiculopathy.
Discussion
Complex proximal metadiaphyseal fractures of the humerus are a rare and difficult injury to manage. Often occurring in the geriatric population with a multitude of comorbidities, they can result in significant short-term and long-term morbidity. 21 Traditionally, many proximal humerus fractures have been managed conservatively; however, as the complexity of the fracture increases, there is an increased risk for loss of quality of life and limited long-term return of function with non-operative management.22,23
Primary ORIF with locked plating has been successful in a younger patient population with proximal humeral fracture. The goals are anatomic restoration, preservation of vascular supply, stable osteosynthesis, and early mobility. 24 In the elderly population, there is an increased risk of fracture comminution, osteoporosis, and osteonecrosis due to displaced fracture pattern, which leads to a high rate of postoperative complications.5–7 In recent studies, despite using contemporary surgical techniques, including fibula strut and locking plate fixation, associated complications of screw cut-out remains to be elevated at 12%–44% in the literature.4,6,25 Moreover, ORIF does not address the common concomitant issues of glenohumeral arthritis and rotator cuff pathology, which can be found with geriatric proximal humerus fractures.26–28 Utilizing magnetic resonance imaging analysis of proximal humerus fractures, rates of rotator cuff tears from 42% to 70% has been demonstrated, which can be associated with limited functional outcomes.29,30 As a result, the current operative approach to complex proximal humerus fractures in this population has shifted largely towards RTSA utilization, with increasing literature support.31–33 With that said, a recent study compared treatment approaches among shoulder and trauma surgeons and found that while the preferred management varied among surgeons of different training and experience, especially when managing complex fractures in low functioning, elderly patients. 34 This is the first study that describes using RTSA to manage complex proximal humeral fractures of the metadiaphyseal region in the elderly. The authors theorize that elderly patients have a prevalence of poor medical comorbidities, poor vascularity, osteoporosis with low-fracture healing potential, and rotator cuff pathologies which would benefit from arthroplasty management. 35 Several anatomic studies demonstrated that the vascularity of the metadiaphyseal humerus originate with the circumflex humeral artery and secondarily by the nutrient artery more distally.35,36 Hence, the risk of the humeral vascular supply should be similar to what Hertel et al described. 37 Furthermore, the authors believe that the benefits of arthroplasty management have been shown in the current literature evidence for treating epiphyseal proximal humeral fractures.38,39
With regard to metadiaphyseal fractures, there is a paucity of literature concerning treatment and outcomes. Some authors have advocated for fixation with complete open or minimally invasive locked plating.26–28 ORIF of proximal humerus fractures in this patient population is associated with higher levels of technical difficulty, 26 outcomes that are operator dependent, 26 the possibility of subacromial impingement syndrome due to hardware prominence, 7 risk of axillary and radial nerve palsies, 28 and a two- to threefold increased risk of all complications when compared to younger patients. 40 Robinson et al presented the large series of patients treated with ORIF and found overall nonunion rate of 7%. 13 They reported no neurologic complications but noted that their surgical approach required protecting the neurovascular structures. 13 Touloupakis et al reported their technique of ORIF and required a special spiral plate to avoid the neurovascular structures; however, they still encountered a few cases of neurologic injuries. 15 While ORIF is an option, the technical difficulty, potential limited postoperative function, and a high rate of serious complications must be considered by both surgeons and patients.
In theory, a load-sharing implant such as intramedullary nail (IMN) would allow for an earlier weight-bearing and return to function. 41 Long-stem RTSA construct has an internal strut similar to an IMN to aid fracture reduction, act as a load-sharing device, and allow early mobilization. 17 Previous studies described using stemmed cemented implants to bypass the proximal fracture site. 17 However, use of cement can be associated with the theoretical risk of cement extrusion into the fracture sites limiting healing, thermal necrosis of the bone, as well as potential difficulty with any future revision surgery.42–44 Recent RTSA design allows press-fit surgical technique with reliable bony healing and comparable postoperative function. 19 By eliminating cementation, there is less difficulty for future revisions, if required, as well as potentially lower rates of loosening compared to cemented implants in RTSA utilized for the treatment of fractures. 19 In the current series, the outcomes of using long-stemmed press-fit RTSA implant for treatment of metadiaphyseal proximal humerus fractures were performed through the conventional deltopectoral approach and showed promising early radiographic results. All patients had consistent, early healing of the fracture. With the exception of one patient who had recurrent trauma, there were no cases of implant loosening or subsidence. ROM and postoperative function demonstrated acceptable and early satisfactory outcomes comparable to previously published series. 17
This paper is the first study evaluating treatment of metadiaphyseal fractures treated with cementless, press-fit long-stem RTSA. However, due to the rare nature of this fracture pattern, this remains a relatively small retrospective series of patients compared to other fracture studies. There was no control group to compare these outcomes, limiting the generalizability of the results to other patient populations. Further studies should include randomized control trials with comparison against the previous standard of care treatments in this patient population. Using a shoulder arthroplasty can lead to potential future problems such as stress shielding, joint infection, or implant loosening; these were not seen in this short-term study but need to be considered in real-life scenarios.
In conclusion, primary arthroplasty with cementless, press-fit long-stem RTSA implant may be a viable alternative to the locked plate or IMN fixation in the geriatric population for the treatment of metadiaphyseal proximal humerus fractures. Early outcomes at 1 year demonstrate high, consistent healing rates, improvement in pain, return of shoulder function, and a minimal complication rate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.