
Abstract
Background
Reverse total shoulder arthroplasty (RTSA) has become an established treatment for cuff arthropathy, severe osteoarthritis and in certain fracture cases. Due to the increasingly aging population, patients who have already exceeded their life-expectancy pose a significant challenge to the shoulder surgeon.
Methods
Patients older than 83 years who received a RTSA were included. Elective cases were compared to fracture cases. Patient demographics, hospital stay length, complication rate, functional outcome, patient reported outcome scores and mortality were assessed retrospectively.
Results
We included 110 cases, 48 in the elective group and 62 in the fracture group. The average age at time of surgery was 86.6 ± 3.5 years. Mean follow-up was 30 months. Elective cases had a significant shorter hospital stay length (P = .014). Functional outcome scores showed better results for the elective group with ASES 79 ± 12 vs 69 ± 19 (P = .07), QuickDASH 29 ± 16 vs 37 ± 21 (P = .22), subjective shoulder value 86 ± 14 vs 75 ± 19 (P = .04*) and VAS .7 ± 1.5 vs 2.1 ± 2.5 (P = .02*). There was no significant difference in ROM and mean quality-adjusted-life-years (QALY) with 3.2 ± 1.8 vs 3.5 ± 2.5 years (P = .69). The complication rate requiring surgical intervention was 2.4% in the elective and 6.5% in the fracture group. The 1-year mortality was 3 (6%) respectively 9 (15%).
Conclusion
RTSA in elderly patients can be successful with good functional outcomes. Age should not be a contraindication. Instead, the patient’s activity level and quality of life should be taken into account. Elective RTSA show better functional outcome scores and lower complication rates compared to RTSA in proximal humeral fractures.
Keywords
Introduction
Worldwide life expectancy is growing as well as the part of the elderly population. This population is often leading a healthy and active life style. Nevertheless, degenerative shoulder pathologies and trauma related shoulder problems limit function and quality of life in the elderly.
Current data reported that individuals of more than 85 years of age represent the fastest-growing demographic in the United States, 1 and they are projected to account for 2.3% of the U.S. population in 2030 and 4.3% in 2050. 2 In Switzerland, the reported average life-expectancy was 82 for men and 86 for women in 2018, 3 and in 2025 more than 20% of the whole Swiss population would be older than 65 years. 4 Although patients older than 80 years could benefit from a total shoulder arthroplasty (TSA),5,6 they might have a higher risk of peri- and postoperative complications because of their limited physiological reserves and higher comorbidities compared to younger patients.7,8
In very old patients, shoulder function may not only limit their quality of life but their autonomous life may also depend on shoulder function for daily activities. Losing one’s independent life style can be frustrating and expensive.
Shoulder surgery can help to overcome these problems. Total shoulder arthroplasties can offer good function, reduce pain and alleviate trauma related consequences. In the last decades, total shoulder arthroplasty (TSA) has become a well-established method for treatment of degenerative shoulder arthropathies as well for multi-part fractures which are surgically demanding.9-11
There is an ethical dilemma, whether to operate on patients who have already exceeded their life expectancy. A reasonable use of resources and sensible balance between benefit and risk for patients older than 80 and undergoing TSA is essential. 7
Previous authors have shown, that anatomical TSA is helpful in improving function and quality of life in patients older than 80 years.5,6,12 Concerning complication rate, comparative studies have shown a lower surgical related complication rate for TSA in the general population than for the well accepted total hip (THA) and knee arthroplasties (TKA) ranging from 2.8% to 7.55% for TSA compared to 7.6% to 15.5% for THA and 6.8% to 14.7% for TKA.13,14 Regarding TSA in patients older than 80 years, Ricchetti et al and Griffin et al reported a higher rate of postoperative anaemia and hospital stay length compared to younger patients. In terms of other perioperative complications, there was a higher trend in the older patient groups with up to 23% vs 17% minor complications and 7% vs 2% major complications, but with no statistical significance.7,15
Recently, there is new literature for RTSA in patients older than 80 years showing good results with comparable complication rates.12,16,17
To our knowledge, so far there is no study comparing primary RTSA in elective cases with RTSA in fracture cases for elderly patients who exceeded their life expectancy. Therefore, the aim of this study is to report and compare functional outcome, pain, quality of life and complications of RTSA for elective and fracture cases in patients older than 83 years (general life expectancy in Switzerland) and to report the 30 days, 1 year and mid-term mortality.
Material and Methods
We conducted a retrospective study, which was approved by the local ethical committee (ID 2018-02336). The study was conducted entirely at the authors’ institution.
Patient Selection
We reviewed our institutions’ database and included all patients, who received a primary reverse shoulder arthroplasty from January 2008 to February 2019 and who were older than 83 years (the average life-expectancy in Switzerland) at time of surgery. We differentiated between elective cases for debilitating cuff arthropathy and dislocated proximal humeral fractures, which received a reverse shoulder arthroplasty. Patients treated with revision arthroplasty or conversion from prior osteosynthesis were excluded.
Data Collection
We retrospectively reviewed the medical records for time of surgery, duration of hospitalization, ASA (American Society of Anesthesiologists) classification at time of surgery, BMI (Body Mass Index), clinical follow-ups with range of motion (ROM). Patient-rated functional outcome scores such as the ASES (American Shoulder and Elbow Surgeons), VAS (visual analogue scale from 1-10), SSV (subjective shoulder value) and QuickDASH (Disabilities of the Arm, Shoulder and Hand) were evaluated. Patients unfit or unwilling to come in for a final follow-up were contacted via phone interviews or through their family physician and the above-mentioned scores were assessed.
The quality-adjusted-life-year (QALY) is a well-established indicator of the life quality for the remaining years 18 and was calculated as the years of life following the operation, multiplied by the utility value, for the current study, defined as the postoperative American Shoulder and Elbow Surgeons Shoulder Score (ASES) score (0-1 points) at last follow-up. A QALY of 1 indicated 1 year with excellent shoulder function.
All major surgical related peri- and postoperative complications were evaluated and revision surgeries were recorded. Time of death, if applicable, was noted for the overall mortality.
Surgical Technique
All procedures were performed in a beach chair position under general anaesthesia. Every patient received antibiotic prophylaxis 30 minutes before skin incision and for 24 h postoperatively. Surgeries were performed or supervised by 1 single senior shoulder surgeon using a standardized deltopectoral approach. In all cases, an anatomical reverse shoulder system were used (Zimmer® Anatomical Shoulder™, Warsaw, Indiana 46 580 USA). All stems were cemented in a standardized way.
Postoperative Care and Evaluation
All patients received a postoperative x-ray a.p. And Morrison before discharge. Standard clinical and radiological follow-ups with evaluation of range of motion (ROM) were performed at 6 weeks, 12 weeks and 1 year postoperatively, followed by yearly controls.
Statistical Analysis
Descriptive statistics used frequencies and percentages to present the data. Paired t-test and chi-square test were applied to compare data from both groups. A P-value of less than .05 was considered significant. A Kaplan-Meier curve was generated to analyse patient survivorship following surgery. All the statistical analyses were performed using SPSS version 23 software (SPSS Inc, Chicago, Illionois).
Results
Comparision of demographics, duration of hospital stay and follow-up time. BMI, body mass index; ASA, American Society of Anesthesiologists.

Mean follow-up was 36 months (3 to 148 months), excluding 8 patients, who have deceased within 3 months postoperatively due to medical conditions (pneumonia, sepsis, renal failure, malignancy) and 14 patients who were lost to follow-up (Table 1). Patients were considered lost to follow-up if they had no follow-ups longer than 3 months postoperatively.
Range of Motion (ROM)
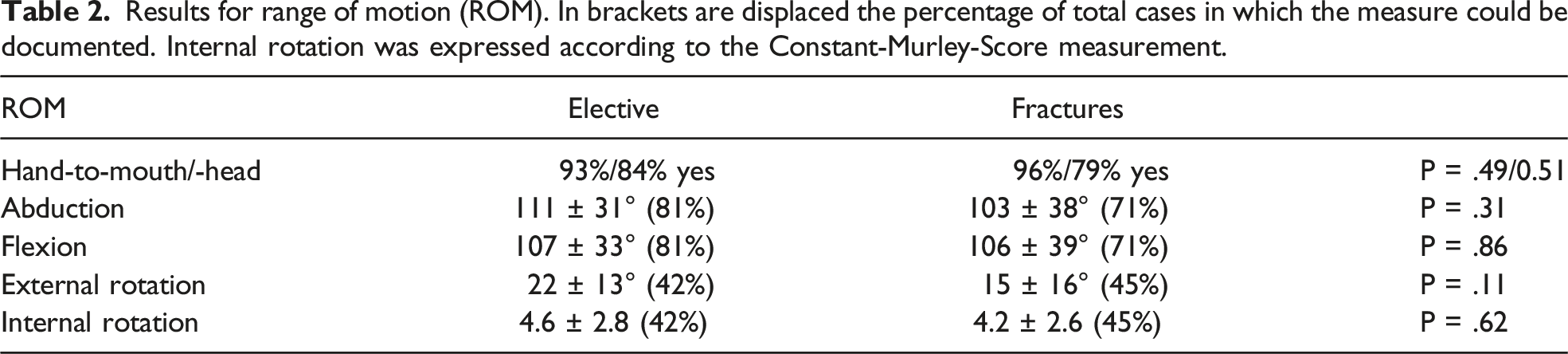
Results for range of motion (ROM). In brackets are displaced the percentage of total cases in which the measure could be documented. Internal rotation was expressed according to the Constant-Murley-Score measurement.
Functional Outcome Scores
Patient reported functional outcome scores and quality-adjusted-life-years (QALY). The values are given as average and standard deviation. In brackets are displayed the percentage of total cases in which the measure could be documented.

QALY Score
The mean QALY was 3.2 ± 1.8 years for the elective and 3.5 ± 2.5 years for the fracture group with no statistic significant difference (P = .69).
Complications
Surgical related complications and perioperative deaths.

Mortality
Mortality rate and mean survival.

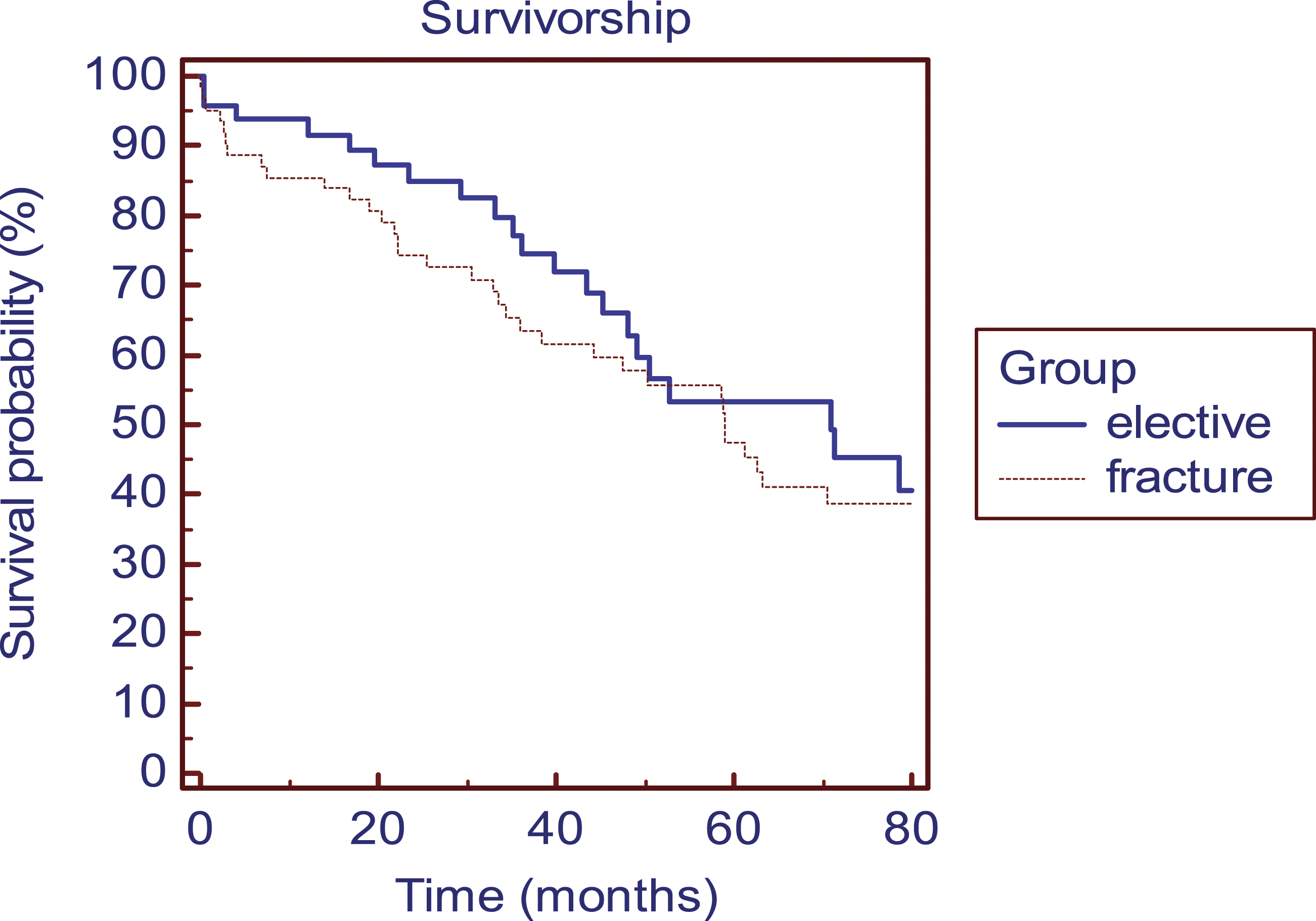
Kaplan-Meier curve showing the survival rate after implantation of a RSTA in the elective and fracture group.
Discussion
In the present study, good clinical results with acceptable low complication rate suggest that RTSA can be a save treatment option for patients, who have already exceeded their life expectancy, and provide improvement in quality of life.
In the ever-older growing population, pensioners today often lead a very healthy and active life style. Shoulder problems may hinder the elderly in their daily activities and might even take away their independency. In the last decades, shoulder arthroplasties have become well established for both arthropathies and trauma related problems with lower perioperative complication rates compared to total hip or knee arthroplasties.13,14 For shoulder arthroplasties, complication rates have been shown to be similar for patients older than 80 years compared to younger patients.7,12,15 For patients older than 90 years, Churchill 5 could show excellent pain relief, significant improvement in functional outcome and even enhanced general health status in a small cohort of 8 TSA cases.
For RTSA, recent publications have examined outcome, complication rate, mortality and morbidity in this specific patient population older than 80 years, and have also shown good results. Clark et al has investigated 242 RTSA for elective and fracture cases, of which 179 had a minimum of 2-year follow-up. They could show good results for range of motion and a surgical related complication rate of 12% with a low reoperation rate of 1.7%. 16 They did not report outcome scores. Kriechling et al reported 171 RTSA in 159 patients, also with good ROM, but a higher complication rate of 18% for local complications and a reoperation rate of 8%. Both studies have not compared outcomes for elective and fracture cases.
The here presented results showed similar good values for range of motion, both for elective and fracture groups with no statistic significant difference in between both groups. In addition, we documented the ability to reach mouth and head with the hand of the affected side, because we believe, that these are important functions for the elderly to maintain or improve their quality of life and independency. 93% of the elective and 96% of the fracture cases were able to reach their mouth and 84% resp. 79% could reach their head, which we consider to be excellent results.
We found better functional results and significant better subjective shoulder values and pain reduction in patients treated with RTSA for degenerative indications in comparison with patients treated with RTSA for proximal humeral fractures. Range of motion was comparable between the 2 groups. In elective RTSA cases we found a non significant better ASES of 79 (
For estimation of quality of life, we adjusted the well-established quality-adjusted-life-year (QALY) and used the ASES as the utility value. Therefore, a QALY of 1 indicated 1 year of excellent shoulder and elbow function contributing to a good general quality of life. In our study, elective cases showed a QALY of 3.2 ± 1.8 years compared to 3.5 ± 2.5 years for fracture cases, so good shoulder function could be expected for at least 3 years following surgery. We consider this to be an additional factor in the decision making process for surgical intervention in the elderly. In the time of scarce resources, cost-effectiveness should also be taken into consideration. In the United States, a cost threshold of under $50.000 per life-year gained is considered to be a reasonably cost-effective treatment. 20 In our clinic, $22.000 is a rough estimate of treatment costs for a RTSA with a hospitalization duration of 7 days. Allthough we cannot refer to life-years gained, but rather to life-years with good shoulder function, we consider the treatment to be highly cost-effective in respect to a QALY of 3.2 to 3.5 years, which would add up to approximately $7.000 per year gained.
Comparing the complication rate, our results show a similar local complication rate with 10.4% for elective and 12.9% for fracture cases and a comparable revision rate with 2.4% and 6.5% respectively. This is in the same range as reported by the Nordic Arthroplasty Register with a revision rate of 5%, mostly caused by infections, loosening and instability in a patient cohort of 1904 RTSA with a mean age of 74 years. 8 We could observe more postoperative anaemia in the fracture group, which could be explained due to the obvious blood loss in fractures.
Peri- and post-operative anaemia were also reported to be higher in the very old population. 7 Further data analysis of 58.790 TSA in patients from younger than 40 to older than 80 years showed a longer hospital stay (4 days in over 80-year-old patients vs 3 days in patients younger than 50 years), an increased need for blood transfusions but no difference in cardiac, embolism or infection for patients older than 80 years when compared to a younger patient population. 6 In our study we found a significant longer stay of hospitalization for patients treated for fractures (9.4 ± 5.3 days) compared to elective RTSA (7.1 ± 3.3 days) in patients with a mean age of 87.0 and 86.0 years respectively.
Mean survival in the patients reported by Foruria et al 6 for TSA patients older than 80 years was 7.5 years. We found a mean survival rate of 5.1 years and 5.0 years in elective and trauma group respectively, but the here presented patients were older with mean ages of 86.0 (83-98) and 87.0 (83-98) years.
There are obvious limitations to this study. First, it was a retrospective case series in a regional hospital, in which standardized data collection often poses an administrative challenge and involves a risk of selection bias. Functional outcome scores were not part of routine preoperative and postoperative assessments and thus, we could not present pre- and postoperative comparisons.
Second, data collection is very challenging in this specific very old patient cohort. We often miss functional outcome scores in patients who already have deceased at the time of this study. Many of our patients moved to or live in nursing homes. Therefore, we could not contact all patients directly. Some patients could only be evaluated by telephone, some were unwilling to come in because of their limited mobility and some were contacted and examined by their family physician who were kind enough to collect outcome data. Others are suffering from dementia and could not be questioned sufficiently for this study. And naturally, some patients were simply lost for follow-up. These limitations explain the diversity in follow up time and also reflect the reality of clinical assessment in very old patients.
The idea of treating very old patients with a RTSA is not to make them function and score like younger patients, but to offer pain relief, reliable and acceptable function. Therefore, we believe that shoulder function scores and range of motion are not that important in this special patient cohort. We believe that even with a limited standardized data set, functional outcome, pain and complication rates in very old patients who underwent RTSA can be presented.
Conclusion
In conclusion, patients who have already exceeded their statistical life expectancy, could profit from a reverse shoulder arthroplasty for degenerative shoulder problems and fractures. This continuously growing population raises the question, whether a surgical intervention is worth the perioperative risk. They might need a longer hospital stay, but in general will not show a statistically higher complication rate compared to a younger population. Restored shoulder function and less pain might offer this special patient group a better quality of life and longer independence. 94% of patients treated for degenerative shoulder problems and 85% treated for proximal humerus fractures were still alive 1 year postoperatively with a functional implant in situ.
Footnotes
Authors’ contribution
Mai Lan Dao Trong: Conceptualization, M, Validation, Data Curation, Formal analysis, Investigation, Visualization, Project administration, Writing and Review.
D Dimitriou: Software, Formal analysis, Review.
S Guenkel: Validation, Writing original draft.
N Helmy: Conceptualization, Review and Editing.
U Riede: Validation, Resources, Review and Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ulf Riede received consultant payments but not royalties from Zimmer Biomet, which was not related to the subject of this work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This research did not receive any specific funding.
Ethical Committee Approval
Ethikkommission Nordwest-und Zentralschweiz (EKNZ) ID 2018-02336