
Abstract
Although lipomas are the most common mesenchymal tumors, the intramuscular type is rare. We report the case of a patient with rotator cuff arthropathy with a lipoma in the teres minor. Wide surgical excision and total shoulder arthroplasty with reverse prosthesis was performed and 18 months of follow up showed excellent results with any recurrence. The teres minor is extremely important for the proper function of a reverse prosthesis, and lipoma growth in the muscular belly can compromise the functionality of the prosthesis. To the best of our knowledge, this is the first case report of a rotator cuff arthropathy with a lipoma in the teres minor.
Introduction
Lipomas are the most common benign mesenchymal tumors. 1 They are composed of mature adipose tissues. Depending on their location, they can be superficial or deep. Intramuscular lipomas are the deep kinds that grow inside a muscle and account for <1% of all lipomas.2,3 Intramuscular lipomas are of three types: infiltrative, well defined/non-infiltrative, and mixed. 2 The most common type is the infiltrative type, which is the most likely to reproduce. Involution and atrophy of muscle fibers around the lipoma with a neuropathic or myopathic pattern have been demonstrated by Mori et al 4 in up to 70% of cases, mainly in the infiltrative type. The main differential diagnosis is liposarcoma, which appears very similar to the infiltrating intramuscular lipoma in both imaging and histopathology. Liposarcomas are 10% to 35% of soft tissue sarcomas. 5 Rotator cuff arthropathy is associated with massive rotator cuff rupture and glenohumeral osteoarthritis. Surgical treatment with a reverse prosthesis is the treatment of choice. In the absence of other external rotators, the teres minor is critical for the proper functioning of a reverse prosthesis. 5 When there is no teres minor or it is dysfunctional, it is necessary to replace it by muscle transfer, usually using the wide dorsal or teres major. 6 Considering that the lipoma compromises the muscle mass of the teres minor, it can cause necrosis by compression, affecting its innervation, or in extreme cases, replacing all muscle mass compromising the functionality of the reverse prosthesis. Here we report a case of rotator cuff arthropathy with a lipoma in the teres minor with the review of literature.
Presentation of the Case
A 62-year-old female was presented with chronic right shoulder pain and progressive functional limitation which affected her daily activities and quality of life; with the historical background of humeral dislocation which one was solved by a closed reduction, without requiring any other further treatment. Her physical examination showed 100 degrees of forward elevation, 10 degrees of external rotation, internal rotation up to L4 and preservation of the external rotation function. On a plain shoulder x-ray, we found ascent of the humeral head, narrowing of the acromiohumeral interval, glenohumeral osteoarthritis and inferior osteophyte, compatible with grade 2 of Hamada rotator cuff arthropathy (Figure 1).

Plain radiography shows ascent of the humeral head, narrowing of the acromiohumeral interval, glenohumeral osteoarthritis and inferior osteophyte, grade 2 of hamada rotator cuff arthropathy.
MRI showed massive tear of rotator cuff with complete tear of the supraspinatus with tendon retraction to the glenoid edge and complete tear of the infraspinatus, atrophy and fat infiltration Goutallier grade 4. As an incidental finding, a compatible image of the intramuscular mass compatible with fatty tissue in the belly of the teres minor (Figure 2).
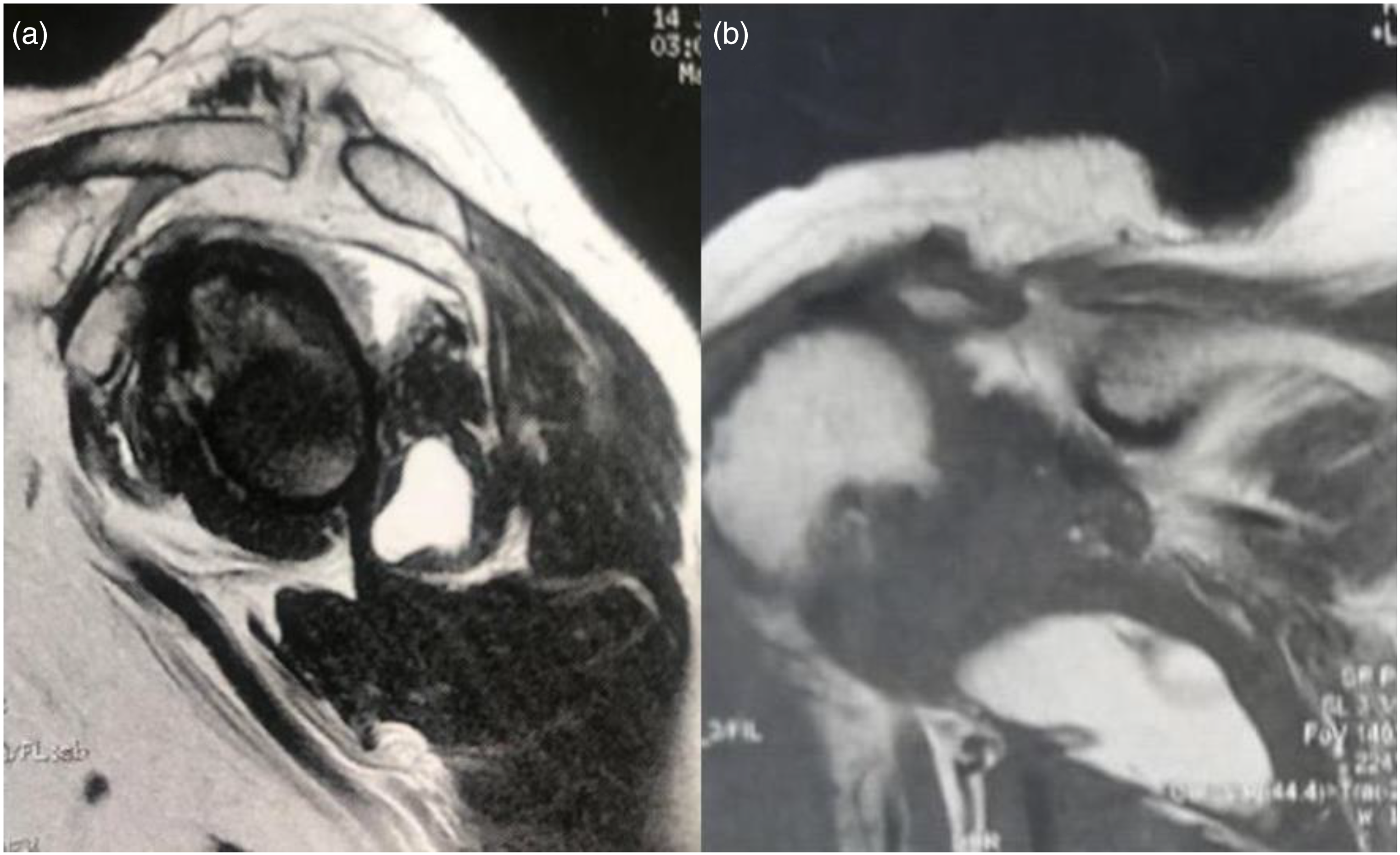
(a) T1 sagittal image with presence of a well-delimited lesion in the teres minor. Atrophy of the supraspinatus and infraspinatus. (b) T2 image of the lipoma in the teres minor, humeral head ascent.
Under general anesthesia, the patient underwent two procedures, the first one consisted in the excision of the tumor on the teres minor by a posterior approach of the shoulder parallel to the muscle fiber orientation, after the release of subcutaneous tissue, the teres minor muscle belly was identified and then the excision of the fat tissue tumor was done, after that an appropriate wound closure was performed through anatomical planes (Figure 3). At the same surgical time, a reverse shoulder replacement by a deltopectoral approach was performed, the deltopectoral interval was opened, with the exposure of the anterior aspect of the glenohumeral joint, the biceps tendon was tenotomized, then the subscapular tendon was released, the reverse shoulder replacement was then performed with Tornier® reverse prosthesis following the usual technique with cemented stem. The stability of the components was then assessed, after that an appropriate wound closure was performed through anatomical planes, the procedure had no complications.

Well-delimited lipomatous mass in the muscular belly of the teres minor, extracted by a posterior approach of the right shoulder.
The anatomopathological study reported lipoma (Figure 4).

The cuts show mature adipose tissue consisting of adipocytes of regular size and shape without evidence of stromal atypia. No other tissue component is identified. Hematoxylin–eosin staining 40×.
The patient recovered well in the postoperative period. Imaging of functionality was performed at 18 months postoperatively. The patient did not report pain and had good function that allows her to perform all daily activities with an elevation of 140° and without deterioration of external rotation (Figure 5). No local clinical tumor recurrence was noted (Figure 6).

Clinical images of the patient 18 months after shoulder replacement and mass resection with (a) forward elevation of 140 degrees, clinical pictures of the (b) 45 degrees of external rotation (c) internal rotation at the level of T12 (d) posterior approach for the excision of the lipoma and (e) anterior deltopectoral approach for the reverse shoulder replacement were then obtained.

Control x-ray of the shoulder’s patient, 18 months after reverse shoulder replacement, (a) on the anteroposterior view, (b) anteroposterior with abduction and (c) Y scapular view.
Discussion
In 1853, Paget described an intramuscular lipoma on the trapezius and Regan introduced the term infiltrating lipoma in 1946. 7 Subsequently, Greenberg et al 8 differentiated the infiltrating lipomas into intramuscular or intermuscular. Intramuscular lipomas are relatively uncommon and the most frequent locations are the thigh and shoulders. Within the shoulder girdle, they are more frequent in the trapezius, pectoralis major, latissimus dorsi and deltoids. 3 They can occur at any age but are more frequent between ages 40 and 70 years without sex preference, although several studies suggest a higher incidence in women.9,10 Fletcher 2 found that 83% of intramuscular lipomas were infiltrating. The usual symptom is local mass or pain, and it is shown that the growth of lipomas can affect the biochemical homeostasis of the muscle causing its degeneration, affecting its innervation or replacing the muscle mass, rendering it dysfunctional. Diagnosis is confirmed by imaging. Plain radiography shows calcifications, if any, but generally does not provide information. Ultrasonography has a high sensitivity and specificity in superficial lipomas. This allows detection of well-delimited masses but does not have greater precision if the lipomas are intramuscular. It also does not allow differentiation of liposarcomas, the main differential diagnosis of infiltrating lipomas and the most common type of intramuscular lipomas.9,11 The gold standard is nuclear resonance imaging where in t1 and t2 images the usual characteristics of lipomas are found. They are uninodular and may have non-thick septa, infiltrate adjacent tissue and intertwined muscle fibers within the tumor mass. Liposarcomas are generally multilobed with thick septa within the tumor mass and have a size > 10 cm.12–14 Although the shoulders are the site where intramuscular lipomas are frequently found,1,3,15 their presence within the rotator cuff muscles is really exceptional, with a few cases reported in the supraspinatus 11 and subscapular16,17 and a single case in the infraspinatus, 18 with no such cases reported in the teres minor so far.
Rotator cuff arthropathy is a pathology that is associated with massive irreparable rupture of the rotator cuff with glenohumeral osteoarthritis. 19 The treatment of choice is reverse prosthesis,20–22 which was devised by Grammont in 1987.23,24 The functionality of the prosthesis depends on the deltoid and the teres minor, 25 to such an extent that, given the dysfunction of the teres minor, it may be necessary to transfer the wide dorsal to replace its function. 21 Therefore, a lipoma in the teres minor can belatedly compromise its function, affecting the functionality of the prosthesis necessary for rotator cuff arthropathy treatment. 26 Therefore, we decided to excised the mass and perform total shoulder replacement with reverse prosthesis. It was performed in a single procedure given the extremely low risk of recurrence, and there was no suggestive sign of malignancy, which was confirmed in a pathologic study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.