
Abstract
Purpose:
Epileptic seizures can cause shoulder dislocation, recurrent instability and eventually arthritis. The purpose of this study was to report the results, complications and rate of revision surgery following anatomical shoulder arthroplasty in epileptic patients with instability arthropathy.
Methods:
A consecutive series of eight patients with epilepsy underwent anatomical shoulder arthroplasty for recurrent shoulder instability and were retrospectively reviewed after a mean of 4.7 years (range, 2–7.5 years). These included three total shoulder replacements and five humeral resurfacing hemiarthroplasty procedures.
Results:
Mean age of the cohort was 33 years (range, 17–44). All patients experienced post-operative grand mal seizures. Two patients with hemiarthroplasty required further surgery due to painful glenoid erosion. No residual cases of instability were noted. Mean active forward elevation and external rotation improved following surgery. The Oxford Shoulder Score improved from 15 pre-operatively (range, 7–22) to 26 post-operatively (range, 12–45) (p = 0.031). This was accompanied by an increase in the mean Subjective Shoulder Value, which improved from 29 (range, 10–80) pre-operatively to 53 (range, 15–90) post-operatively (p=0.042).
Introduction
Epileptic seizures can cause dislocation of the shoulder joint and recurrent instability through powerful uncoordinated muscle contractions or external trauma secondary to a fall during a fit. 1,2 The incidence of dislocation during a seizure is difficult to estimate since many go undetected, but recurrent instability is common and occurs soon after the first dislocation. 2,3 Posterior dislocation has long been considered a complication of seizure-related disorders and is regarded as the most common form of shoulder instability seen in epileptics, but in the largest observational study of this cohort of patients, anterior instability occurred in 73% of cases and posterior instability occurred in 18%. 4 Locked posterior dislocation has additionally been described in patients with epilepsy with treatments including soft tissue reconstruction, glenoid/humeral osteotomy, posterior bone block augmentation, segmental humeral reconstruction and arthroplasty. 5 –7
Significant bone loss is responsible for high recurrence rate of shoulder instability in epileptics and so the majority of surgical strategies focus on bony augmentation of the glenoid, humeral head or both: This is not always successful, and may lead to persistent instability-related symptoms and arthritis. 1,8 –10 Conservative non-arthroplasty reconstruction is challenging due to the poor residual bone stock, large joint surface defects, and rotator cuff musculotendinous and capsular insufficiency. Patients are often young, in education or seeking work, and find the prospect of living with a painful unstable shoulder untenable. In this context, arthrodesis has been reported to be a successful treatment strategy but the limitation in range of movement that inevitably results means that it is not suitable for all patients. 11 Anatomical arthroplasty may therefore represent an alternative treatment option.
Shoulder arthroplasty is a well-established treatment for primary osteoarthritis of the glenohumeral joint. 12 Patients are often in their seventh decade at the time of surgery and osteoarthritis and fracture sequelae are the most common indications. 13 Revision rates are variable and have been noted to be higher in the younger population. 14 Patients with epilepsy present a unique challenge to conventional approaches to arthroplasty because of their young age, persistent grand mal seizures and severe glenoid bone loss. 4 Nevertheless, clinically significant instability arthropathy is a common long-term finding in this cohort, but the role of prosthetic replacement in its treatment has been infrequently discussed in the literature. 15
We report our experience with anatomical shoulder arthroplasty in young patients with epilepsy-related recurrent shoulder instability arthropathy to assess the results, complications and rate of revision surgery.
Materials and methods
All epileptic patients in whom shoulder arthroplasty had been performed for instability arthropathy were included in this study. Cases were identified using a computerized database and all clinic notes and operative reports were reviewed. Between November 1996 and July 2013, 179 patients with epilepsy underwent shoulder surgery. Of these, eight shoulders in eight consecutive patients underwent anatomical arthroplasty for instability arthropathy. These included three total shoulder replacements (TSR) and five humeral head resurfacing hemiarthroplasty (HHRH) procedures. Arthrodesis was not considered due to the limitation in range of movement and function it has been demonstrated to result in: This was deemed unacceptable to all patients in this study. 11 The decision to replace the glenoid was a joint one between the surgeon and the patient, which took into consideration the patient’s request for a higher degree of certainty over pain relief, any degenerative changes affecting the glenoid surface, the morphology of the glenoid and the known risks of glenoid prosthetic replacement in young patients.
The mean duration of epilepsy in the cohort was 12 years (range, 4–19) and all patients suffered from grand mal seizures. Primary dislocation occurred a mean of 13 years (range, 4–22) before surgery. All cases were performed by the senior authors (Simon M Lambert and Mark Falworth). The mean age at the time of surgery was 33 years (range, 17–44). The cohort consisted of seven males and one female. Six patients had anterior instability and two had posterior instability. One patient had bilateral symptoms. The dominant shoulder was affected in one case. Arthroplasty was performed after an average of two previous stabilization procedures (range, 0–3) in all but two patients in whom the procedure was used as primary treatment due to extensive degenerative changes (cases 3 and 8).
All patients developed instability following, or during, a seizure. In all cases, subsequent dislocations occurred during normal daily activities or further seizures. The indication for surgery was severe pain and dysfunction of the shoulder due to recurrent instability associated with bone loss (on glenoid, humeral or both sides) and degenerative joint disease. All patients were evaluated using diagnostic arthroscopy, plain radiographs and computed tomography (CT). Neurological advice was sought pre-operatively in all cases to optimize the treatment of the epilepsy. Detailed patient data are presented in Table 1.
Patient details.
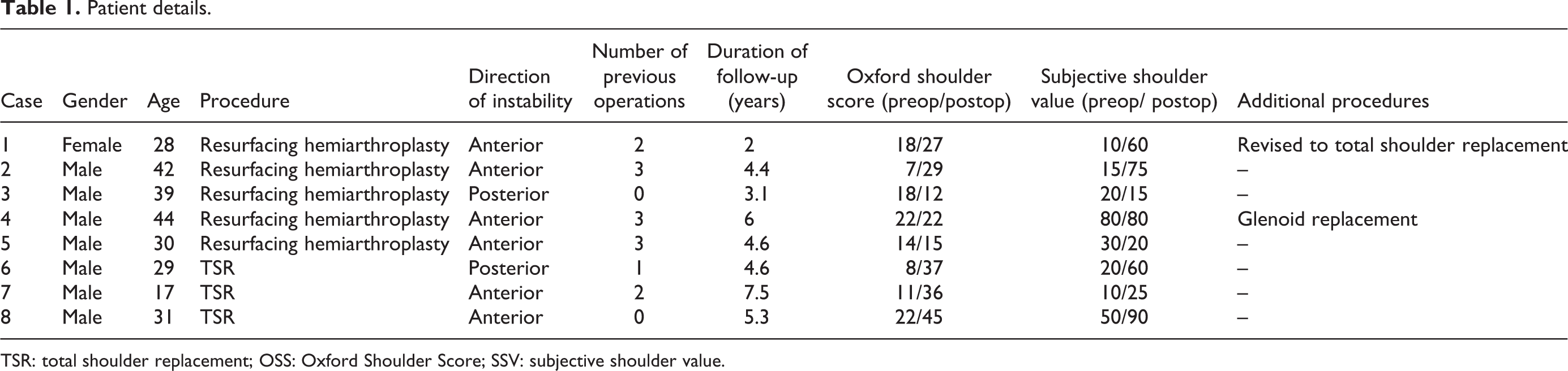
TSR: total shoulder replacement; OSS: Oxford Shoulder Score; SSV: subjective shoulder value.
Operative data
Implants used for total shoulder arthroplasty (TSA) included: one customized prosthesis (Stanmore Implants, Elstree, UK) and two Epoca humeral components (DePuySynthes, Leeds, UK) with metal-backed glenoids. The HHRH implants comprised: two Eclipse humeral resurfacing components (Arthrex, UK), one customized humeral resurfacing replacement (Stanmore Implants, Elstree, UK), one Epoca humeral resurfacing component (Synthes, Leeds, UK) and one TESS humeral resurfacing component (Biomet, UK). All prostheses were implanted using a deltopectoral approach and subscapularis tenotomy. No special reconstruction techniques were required for the rotator cuff. The tendon of the long head of the biceps was retained in all cases. All patients were managed in a simple sling after the procedure and none required subsequent supportive splintage. Post-operative rehabilitation was initiated on the first post-operative day, in a standard programme for prosthetic shoulder arthroplasty. Active-assisted external rotation to neutral and sagittal plane elevation to shoulder level with short lever-arm was commenced as pain permitted. This was followed 6 weeks post-operatively, when the subscapularis tenotomy had healed (judged by provocative clinical examination), by active movements through the available range (including internal rotation), and then deltoid strengthening exercises were introduced 6 weeks later, when humeral component centring was clinically evident during resisted abduction. No variation on this programme or exclusion of patients was required due to epilepsy.
Radiographic analysis
All patients were evaluated using plain radiographs (anteroposterior and axillary views) and CT to quantify bone loss. Pre-operatively, all radiographs were assessed for the presence of degenerative changes using the Samilson and Prieto classification. 16 In this, arthrosis is predominantly graded according to the size of the inferior humeral and/or glenoid osteophyte on the anteroposterior radiograph. This measures less than 3 mm in mild cases, between 3 mm and 7 mm in moderate cases, and greater than 7 mm in severe cases. Moderate cases are further defined by slight joint irregularity and severe cases are characterized by glenohumeral joint narrowing and sclerosis. Post-operatively, all radiographs were reviewed for the presence of periprosthetic lucency and alteration in the position of the components. Radiographs for patients who underwent hemiarthroplasty were additionally examined for glenoid erosion. 12,17
Periprosthetic lucency was graded as 0 if there was no radiolucent line, 1 if the line was at least 1 mm wide and incomplete, 2 if the line was 1 mm wide and complete, 3 if the line was 1.5 mm wide and incomplete, 4 if the line was 1.5 mm wide and complete and 5 if the line was 2 mm wide and complete. Glenoid erosion was graded as none, mild if there was erosion into subchondral bone, moderate if there was medialization of the glenoid subchondral bone with associated hemispheric deformation of the glenoid or severe, if there was complete hemispheric deformation of the glenoid with bone loss to the base of the coracoid. Component migration was defined as present or absent. 12,17
Assessment of clinical outcome
Pre-operative and post-operative clinical outcome measures included active forward elevation and active external rotation. The Oxford Shoulder Score (OSS) was used to assess function. 18 In addition, all patients were evaluated using the Subjective Shoulder Value (SSV), which uses a scale from 0 (worst score) to 100 (best score) to describe the affected shoulder. 19 This can be used as a supplementary tool to traditional, more complex outcome measures and may be used in conjunction with other scores to assess the patients’ outcome.
Statistical analysis
The paired two-tailed Student’s t-test was used to compare the OSS and SSV before and after surgery. A p value of <0.05 was considered significant. The SPSS software package, version 23 (SPSS Inc, an IBM Company, Chicago, Illinois) was used to analyse data.
Results
Mean follow-up was 4.7 years (range, 2–7.5 years). Pre-operatively, all patients were on medical treatment for epilepsy and had been reviewed by a neurologist. All patients had bone loss characterized by a glenoid defect measuring at least 20% of its anteroposterior diameter and a Hill-Sachs lesion involving at least 20% of the articular surface. The Hill-Sachs lesion was engaging in one case (case 1). Glenoid bone loss was anterior in six cases (with anterior instability) and posterior in two (with posterior instability). Following surgery, all patients continued to have grand mal seizures but none had any further episodes of instability/dislocation. No patient reported apprehension during normal use of the affected arm. No further stabilization procedures were performed in the cohort. Degenerative changes were severe in three cases, moderate in one and mild in four.
Complications and revisions
One patient (case 1) with a humeral resurfacing replacement required revision to an Epoca (DePuySynthes, Leeds, UK) TSR with a metal-backed glenoid at 1.2 years due to persistent pain from ongoing glenoid arthritis (Figure 1). Painful glenoid arthritis developed in two further patients with an HHRH. This was treated with an Epoca (DePuySynthes, Leeds, UK) metal-backed glenoid replacement at 1.8 years in one patient (case 4). No revisions were performed in those patients with a TSA.
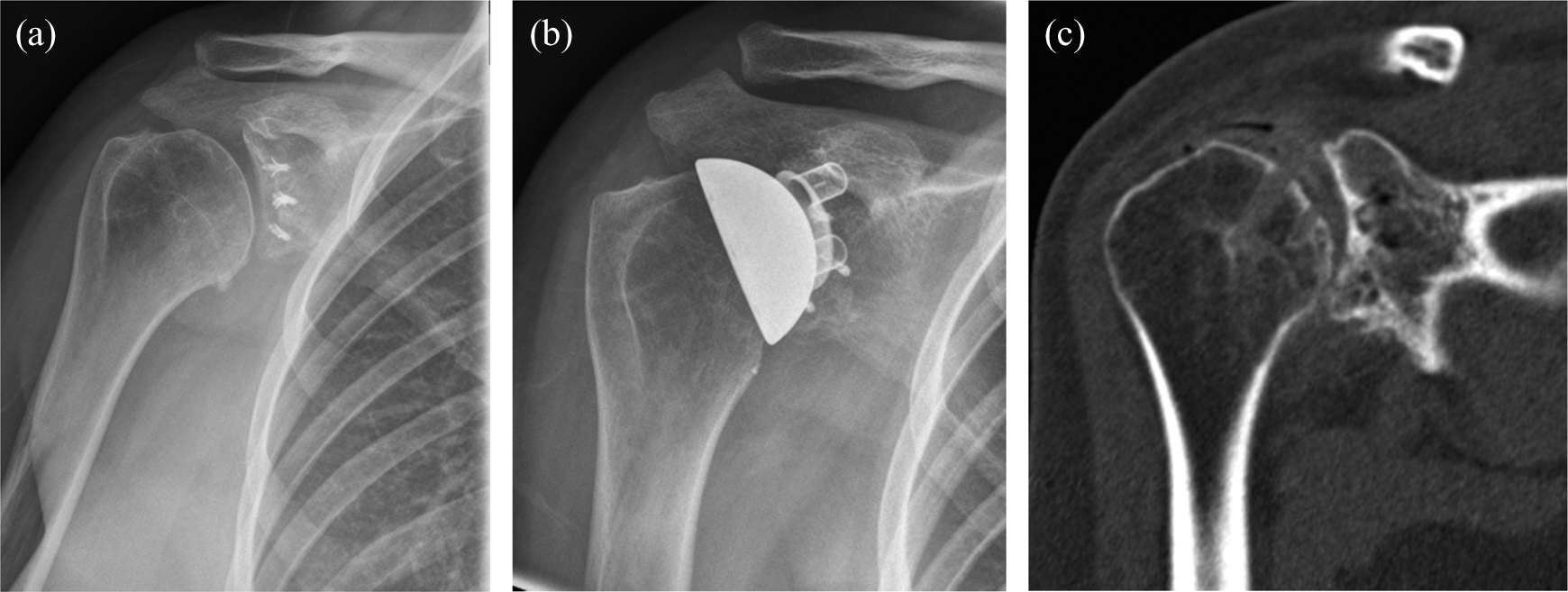
(a) AP radiograph of a 28-year-old right hand-dominant female with two previous stabilizations, 8 months after right humeral resurfacing. (b) AP radiograph of a 28-year-old right hand-dominant female with two previous stabilizations, 4 months after right revision resurfacing TSA. (c) CT scan (coronal section) showing glenohumeral arthritis 10 months following right humeral resurfacing, in a 28-year-old right hand-dominant female with two previous stabilizations. AP: anteroposterior; CT: computed tomography; TSA: total shoulder arthroplasty.
Clinical outcomes
Mean active forward elevation improved from 111° pre-operatively (range, 70°–150°) to 116° post-operatively (range, 70°–170°; p = 0.244). A similar gain was also noted in mean active external rotation, which improved from 31° pre-operatively (range, 10°–60°) to 39° (20°–70°) post-operatively (p = 0.376).
The mean OSS improved from 15 pre-operatively (range, 7–22) to 26 post-operatively (range, 12–45; p = 0.031). An increase was also noted in the mean SSV, which improved from 29 (range, 10–80) pre-operatively to 53 (range, 15–90) post-operatively (p = 0.042).
Radiological outcomes
All HHRH patients had evidence of glenoid erosion, which was moderate in four cases and mild in one. There were no cases of periprosthetic lucency or component migration in the cohort.
Discussion
The management of epilepsy-related instability arthropathy is challenging and involves a multidisciplinary team approach. Pre-operatively it is essential to involve a neurologist so that medical treatment can be optimized. In one study, over 50% of epileptic patients developed degenerative changes a mean of 12 years after their index dislocation. 4 A number of important factors unique to this patient group are likely to have contributed to this: repetitive articular surface damage resulting from high-energy dislocations, multiple pre-operative dislocations and the high recurrence rate. 4 Further conservative reconstruction becomes an unenviable prospect due to poor bone stock, large joint surface defects and rotator cuff musculotendinous and capsular insufficiency. The patients are often young, in education or seeking work, and find the prospect of living with an arthritic unstable shoulder untenable. In this context, arthrodesis has been reported to be a successful treatment strategy but the limitation in range of movement that inevitably results means that it is not suitable for all patients. 11 Anatomical arthroplasty may therefore represent an alternative treatment option; however, it has been infrequently alluded to in the literature. 4,10,15 The outcome has been noted to be favourable with no cases of residual instability or implant-related complications reported. 10,15
Younger patients undergoing shoulder arthroplasty are recognized to be at greater risk of complications and the need for revision surgery, due to their activity levels and higher life expectancy. 20 This is particularly true in the case of epileptic patients with recurrent shoulder instability who typically comprises active males who undergo their first stabilization procedure at 44 years. 10 Due to ongoing seizures recurrence is common and up to 72% of patients undergoing surgery for instability develop arthritis in later life. 10,16
Green and Norris 9 reviewed 19 patients in whom advanced glenohumeral arthritis developed after anterior instability repair. Arthroplasty was used to treat 17 patients at a mean age of 45 years with two humeral head replacements and 15 TSRs. Posterior glenoid erosion was characteristic of the condition. After a mean follow-up of 62 months, a reduction in the level of pain was noted in 16 cases and there was an improvement in functional use of the arm in all but one patient. Three revisions were performed. One humeral head replacement was revised to TSA 6 months following the index procedure due to ongoing pain. Glenoid loosening was noted to occur in one case of TSA, which was later converted to a humeral head replacement. One patient suffered from recurrent posterior subluxation, which necessitated in total shoulder revision 18 months after the initial arthroplasty procedure. Neer et al. 21 reported the results of 273 TSAs that were followed-up for a minimum of 24 months. This included 25 patients with arthritis of dislocation with a mean age of 45 years (range, 19–74). Glenoid involvement was more marked than in the typical shoulder with osteoarthritis and posterior erosion was frequently encountered. The outcome of 13 cases was rated as excellent. One patient had recurrent posterior subluxation following a dislocation 3 weeks after surgery but was treated conservatively. No revisions were performed and no cases of clinical loosening were identified.
Glenoid bone deficiency is a challenging problem for anatomical shoulder replacement and can result in ongoing instability. 22 A number of strategies have been proposed to treat this problem including asymmetric reaming, bone grafting and the use of specialized glenoid components. 22,23 These measures have traditionally been used to treat posterior glenoid wear as this is most commonly encountered in severe osteoarthritis. 24 This is in contrast to epileptic patients with recurrent shoulder instability who most commonly exhibit anterior glenoid bone loss secondary to anterior instability. 4 In the only study evaluating the outcome of shoulder arthroplasty in the setting of anterior glenoid bone deficiency, Lenart et al. 23 evaluated five patients who underwent TSA with an anteriorly augmented component. Mean age at the time of surgery was 67 years and at final follow-up (mean of 33.2 months), there were no cases of loosening, instability or revision. In our series, bone loss was present in all cases but no specific surgical strategies were deemed necessary to address this. Nonetheless, in the short term, we have not encountered any problems with the components such as dislocation, loosening or periprosthetic fracture.
We have reported the first series in the literature of epileptic patients with recurrent shoulder instability, instability arthropathy and persistent grand mal seizures to be treated with prosthetic replacement. These patients had both degenerative and instability symptoms making arthroplasty an appealing treatment option, where maintenance of the range of glenohumeral joint motion was desired and the option of arthrodesis uncertain due to the degree of bone loss on one or both sides of the joint. Mean age of the cohort was younger than in other published reports but the results suggest that arthroplasty can still be successful in improving functional outcome and maintaining stability while preserving range of motion with improved rotator cuff function. The crucial finding in this study is that despite all patients continuing to have grand mal seizures following surgery, there were no further episodes of instability. This confounds traditional thinking where arthroplasty in this population is deemed to have an unacceptably high risk of complications due to the damage ongoing powerful seizures can cause. We speculate that pre-operative neurological review was essential to optimize anti-convulsive therapy and limit the number of seizures (without necessarily eradicating them), thereby reducing the risk of prosthetic disruption during the post-operative period.
Glenoid erosion occurred in all cases of HHRH and was treated by revision to TSA in one patient and isolated glenoid replacement in another. No revisions were undertaken in the TSR group and there were no cases of periprosthetic lucency or component migration in the entire cohort. These are similar findings to other reports of arthroplasty in young adults where glenoid erosion requiring further surgery occurs relatively frequently following hemiarthroplasty. This is in contrast to TSA, which is associated with fewer re-operations and a higher revision-free survival rate. 12,25
Limitations of this study include those associated with its heterogeneous cohort and the mean follow-up of 4.7 years, which is relatively short in terms of prosthesis and functional survivorship. Due to the rarity of epilepsy-related shoulder instability in which bone loss and surface degeneration mandate intervention only a small number of cases were included. We cannot make a comprehensive comparison between HHRH and TSA for this problem but these results suggest that, in common with the literature concerning prosthetic arthroplasty of the shoulder in young patients, those with a TSA will have a superior result to those with an HHRH. Nevertheless, this study provides some insight into a difficult and uncommon problem.
In conclusion, patients with epilepsy-related recurrent shoulder instability pose a significant challenge to management. Multiple stabilization procedures have often been performed, increasing the risk of arthritis. 9,21 Patients can present simultaneously with degenerative and instability-related symptoms. Our results show that hemiarthroplasty is still associated with a high rate of revision even with a short-term follow-up. Given that instability arthropathy is associated with posterior glenoid erosion, hemiarthroplasty may not be the most suitable procedure since it has been associated with poorer results when the glenoid is non-concentric. 21,26 TSA may therefore be the better alternative.
Conclusion
Despite ongoing post-operative seizures in this series, shoulder arthroplasty eliminated recurrent instability, improved functional outcome and maintained a range of movement, which was more functional by virtue of the reduction in instability. Before definitive conclusions can be made regarding the precise role of arthroplasty in the treatment of recurrent shoulder instability in epileptic patients, further larger, long-term studies are required.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.