
Abstract
Purpose
To identify prior studies of arthroscopic glenoid component removal after total shoulder arthroplasty (TSA) and understand indications, techniques and patient outcomes.
Methods
A search of the English language literature on arthroscopic removal of the glenoid component (ARGC) after TSA published between 2005 and 2021 was performed from MEDLINE and EMBASE databases. Articles with ARGC after TSA were identified and we recorded article characteristics as well as patient demographics and outcomes contained within the studies.
Results
A total of six publications (two case reports and four retrospective case series) detailing the outcome of ARGC performed on twenty-five shoulders were identified. The average time from index procedure to glenoid removal was 117 months and mean age at time of ARGC was 75 years. Although patient reported outcomes measures (PROMs) varied in type and reporting style, all articles reported improvements in PROMs. Twenty patients in this systematic review were evaluated for post-operative complications and the complication rate was found to be 15% (n = 3). There were 2 cases (18%) of superior migration of the humeral head relative to the glenoid and no reported cases of anterior or posterior humeral head subluxation. Two of 25 patients (8%) underwent subsequent open revision procedures.
Conclusions
The limited number of publications in this systematic review demonstrates that ARGC after TSA can result in improvements in both pain and PROMs. This less-invasive arthroscopic technique may be an alternative to open revision for lower demand patients; however, future prospective, comparative studies are necessary to better define indications.
Keywords
Introduction
Loosening of the glenoid component is the most common reason for revision after total shoulder arthroplasty (TSA) and may be responsible for 30% of revision procedures.1–3 While TSA continues to be a frequently performed and effective treatment option for pain relief and improvement of function for degenerative shoulder conditions there remains concerns regarding implant longevity.4–7 A recent population-based cohort study has estimated the lifetime revision rate for a failed primary TSA to be as high as 25%. 8 International joint replacement registries also have shown a rapidly growing number of shoulder arthroplasty procedures and future revision rates for TSA will likely be affected by this increase in primary volume.9,10
Several treatment options have been proposed for glenoid loosening, including glenoid bone grafting, open conversion to a hemiarthroplasty, revision glenoid implantation and conversion to reverse total shoulder arthroplasty (RTSA). 11 However there is currently no consensus on the optimal surgical technique, as all of these proposed methods have been shown to have varying complication and reoperation rates.1,12–15 Arthroscopic removal of the glenoid component (ARGC) after TSA has been proposed as an option for presumed aseptic polyethylene loosening (Figures 1 and 2). 16 Proposed advantages of this technique include a less-invasive arthroscopic approach, which may be beneficial in older patients with multiple medical comorbidities due to the potential to avoid some complications associated with open revision.17–19 Although open revision TSA techniques have been well studied, there remains a paucity of literature related to indications, outcomes and complications related to ARGC after TSA.

Preoperative (figure 1) and postoperative (figure 2) axillary radiographs for a case of ARGC after TSA.

Preoperative (figure 1) and postoperative (figure 2) axillary radiographs for a case of ARGC after TSA.
The purpose of this systematic review was to identify prior clinical series related to ARGC after TSA to better define indications, complications, and outcomes related to the procedure. We aimed to describe the clinical and PROMs that were previously published on this technique. We hypothesized that ARGC can be a useful operative technique for the revision of a failed primary TSA due to aseptic osteolysis of the polyethylene glenoid component.
Materials and Methods
Institutional Review Board exemption was obtained for this study. The paper follows the transparent reporting guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist.
Literature Search
On 07 September 2021, a search of the English language literature on ARGC after TSA published between 2005 and 2021 was performed from MEDLINE and EMBASE databases. A systematic review librarian from our institution's Health Science Library assisted with search strategy development. Search strategies are detailed in Table 1. We used 2005 as the start date as the first paper to describe this surgical technique was published that year. 16 All article formats, including case reports, expert opinions, retrospective reviews, and others, were included in the index search. Non-human research, cadaveric studies, articles not available in English, and surgical techniques not related to arthroscopic glenoid component removal were excluded. To ensure all instances of this technique were captured, there was no article exclusion based on sample size, follow-up length, reported complications, or study design.
Demonstrates the search strategies (mesh terms) used in our systematic review.

Study Selection and Data Extraction
Titles and citations were screened for duplicates in Mendeley (Elsevier, London, UK) and Microsoft Excel (Microsoft Corp, Redmond, WA). Remaining titles and abstracts were screened for eligibility independently by two authors, with any discrepancy being resolved through discussion and consultation with a third author. Eligible full-text articles were assessed against the inclusion and exclusion criteria and data extracted.
Data extracted from studies includes patient demographic information, index surgery and revision treatment technique, implant type, time to revision, revision surgical technique, functional outcomes, radiographic parameters, and complications. All data was extracted in duplicate and differences resolved through discussion and consolation with a third author. A risk of bias assessment and data synthesis was not performed due to the small volume or articles available on this topic.
Results
There was a total of 768 articles identified for review. Figure 3 illustrates article inclusion and exclusion for this investigation (Figure 3). After review of abstract and title, 50 articles were included for full text review. After applying exclusion criteria, a total of 6 articles were included in the final review (Figure 3). Of the 6 included articles, 2 were case reports, 3 were retrospective case series and 1 was a retrospective cohort study. A total of 25 cases of ARGC after TSA were identified across the included articles, the largest of which included 12 cases. An overview of information available within the clinical articles in presented in Table 2 (Table 2).

PRISMA flow chart for systemic review of arthroscopically removed glenoid components.
Characteristics overview of articles with any arthroscopically removed glenoid component.

NR = Not Reported
Case Characteristics
Demographic information was inconsistently reported, with 5/6 articles included either patient sex, age, or laterality. The mean age was 75 years (range 50−86). The indications for index TSA were commonly osteoarthritis, rheumatoid arthritis, and humeral head osteonecrosis. Average time from index TSA to ARGC was 117 months (range 12−240) (Table 2).
Outcomes
The patient reported outcome measures (PROMs) varied across articles, including American Shoulder and Elbow Surgeons Score (ASES), visual analog pain scale (VAS), Simple Shoulder Test (SST), UCLA Shoulder Score, and the Constant-Murley score (CMS) as noted in Table 3 (Table 3). Improvement from preoperative baseline was reported across all functional outcome measures, when available.
Pre and post-surgical patient reported outcome data for arthroscopic glenoid removal.

NR = Not Reported; * = Reported as Mean.
Range of Motion
Reported change in range of motion was also variable. Forward elevation was reported in 16 patients preoperatively and 17 patients postoperatively with means of 117.5° and 117.4° respectively. External rotation was also reported in 16 patients with a mean of 32.5° pre-operatively and 34.7° post-operatively (Figures 4 and 5)

Clinical photograph demonstrating postop ROM after bilateral ARGC.

Clinical photograph demonstrating postop ROM after bilateral ARGC.
Imaging
Post-operatively imaging was not routinely reported in series of ARGC (Table 4). Of the 11 patients with detailed postoperative imaging, 0 (0%) had any indication of subluxation and 2 (18%) had some evidence of superior migration of the humeral head relative to the glenoid. The average lateral offset of these 10 patients was −1.7 mm compared to 6.4 mm pre-operatively.
Details of the imaging modalities used in the publications in our review.
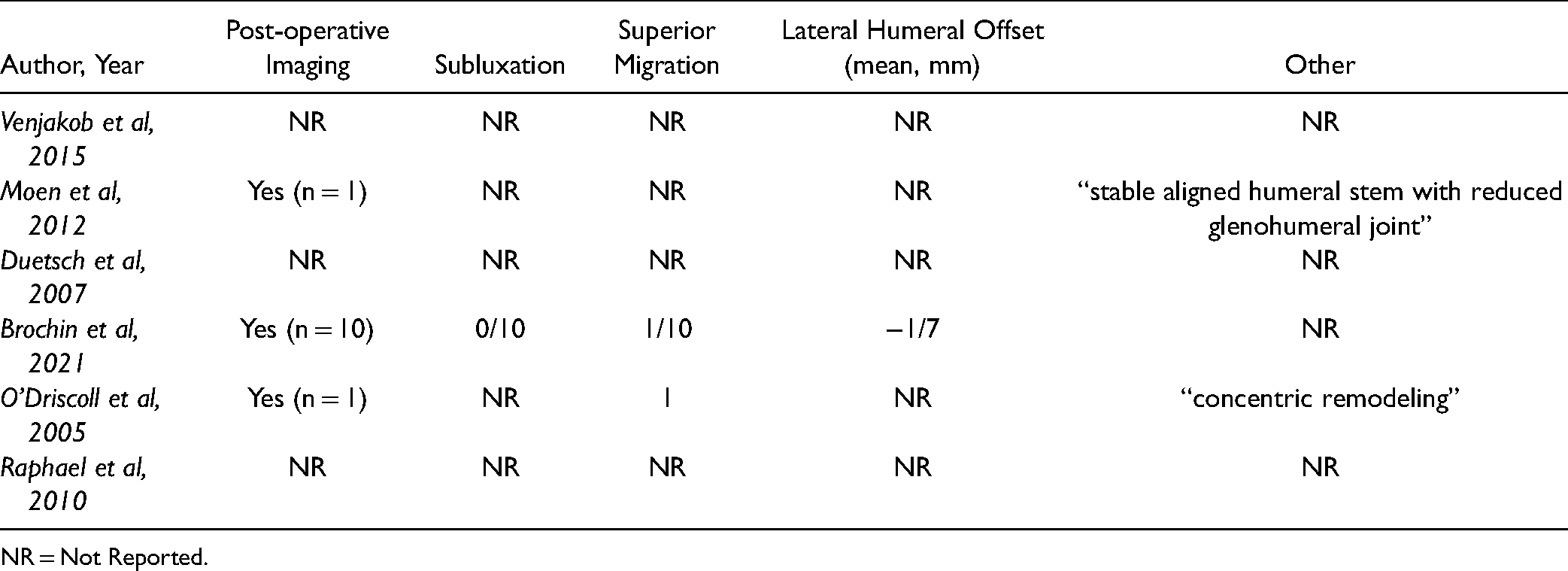
NR = Not Reported.
Complications
Complications were reported in 4/6 articles (Table 5). The overall complication rate was 15% (3/20 cases). The most common complication that was reported was reoperation, which involved open revision. This was reported in 2/25 (8%) patients identified in our review due to continued pain.
Pre and post-surgical range of motion and complications for arthroscopic glenoid removal.
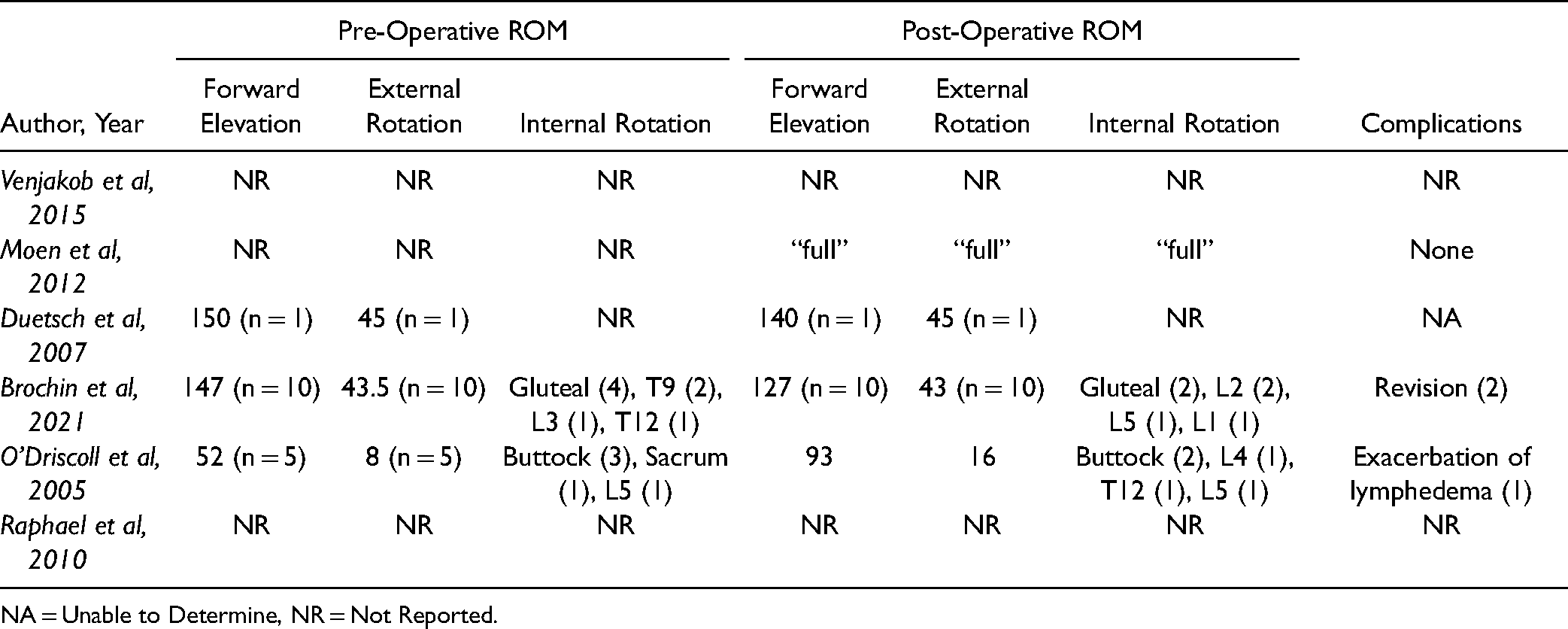
NA = Unable to Determine, NR = Not Reported.
Discussion
Our systematic review identified six clinical articles (25 cases) reporting on outcomes after ARGC after TSA (Figures 6 to 8). At the time of final follow-up (56 months) Brochin et al reported a decrease in VAS pain scale and an increase in ASES score. 17 Raphael et al retrospectively compared outcomes of glenoid open and arthroscopic glenoid removal to revision reimplantation procedures. 20 They reported improved Constant and UCLA scores for 5 of their patients that underwent ARGC and there were no statically significant differences between resection and reimplantation. 20 Additionally, O’Driscoll et al reported that all five patients in their series had improved pain after ARGC and stated that all the patients in their study would choose the same procedure again. 16 The outcomes of different revision techniques to address glenoid component loosening have also been reported on in previous studies. In their study comparing the outcomes of open conversion glenoid resection to reimplantation, Aibinder et al reported no significant differences in the outcomes between the two groups. 21 Cheung et al reached a similar conclusion in their comparative study but additionally reported a slight improvement in active elevation for the reimplantation group. 22 A previous systematic review has also identified improved PROMs, mainly in pain scale, ASES and Constant scores, for both revision TSA and conversion to RTSA after a failed index TSA. 1 Findings from this current systemic review indicate similar improvement in pain relief and PROMs after ARGC.

Intraoperative (6, 7) photographs depicting ARGC after TSA. Figure 8 depicts the resected polyethylene glenoid component and cement.

Intraoperative (6, 7) photographs depicting ARGC after TSA. Figure 8 depicts the resected polyethylene glenoid component and cement.

Intraoperative (6, 7) photographs depicting ARGC after TSA. Figure 8 depicts the resected polyethylene glenoid component and cement.
A proposed benefit of ARGC after TSA is that it may be less invasive (and potentially less morbid than open revision). This systematic review found that in primary clinical articles related to ARGC after TSA, complications were infrequently reported. Twenty patients were evaluated for postoperative complications. One patient (5%) had exacerbation of their pre-existing lymphedema.16,17 Two patients 2 patients (10%) had persistent pain postoperatively and underwent conversion to RTSA.16,17 None of the publications in our review reported any intraoperative complications for these reoperations. In addition to ARGC after TSA, several revision options such as conversion to RTSA, open conversion to hemiarthroplasty, and component re-implantation for aseptic glenoid component loosening exist. Previous publications on these revision options have shown variable rates of complications and reoperations. Additionally, a larger retrospective series with 127 shoulders focusing on conversions to RTSA reported a 29% rate of intraoperative complication and 20% reoperation rate. 13 A complication rate of 35% and a 29% reoperation rate was reported by another retrospective study that outlined outcomes of open revision hemiarthroplasty for aseptic glenoid component loosening. 14 A higher reoperation rate of 67% for glenoid component revision has also been reported. 15 Additionally, a systematic review of 3843 failed index TSAs undergoing either revision TSA or conversion to RTSA reported a 20% postoperative complication and a 13% re-operation rate. 1 It is worth noting that the leading cause for re-operation in these studies was recurrent loosening of prosthetic components and instability.1,12–15 Our review shows lower reported complications and revision rates for ARGC when compared to other operative modalities for treating aseptic glenoid component loosening.
The findings in this systematic review indicate that ARGC has historically been performed for older patients (mean age of 75). A plethora of factors such as infection, instability, loosening and the status of the rotator cuff can impact the management of a failed primary TSA. 23 Even though re-implantation of the glenoid component may have potential advantages, open revision procedures can introduce substantial risk particularly for elderly patients with multiple medical co-morbidities. 24 Prior studies have indicated that patients undergoing re-implantation and conversion to RTSA may have less-advanced arthritic disease and higher baseline levels of function than those undergoing ARGC. 20 Several examples from our findings support this trend. O’Driscoll performed this procedure in patients with morbidity obesity, difficult index procedure exposure, large rotator cuff tears, and other those with severe medical co-morbidities. 16 In their series, Raphael et al indicated that the resection group had more prior surgeries and lower functional demands. 20 Additionally, they stated that ARGC was performed in patients with insufficient glenoid bone stock. 20 In this context, ARGC might be better reserved for patients who have a lower baseline functional demands or may be at higher risk for surgical morbidity with open revision procedures in patients with co-morbidities. In addition, considering that ROM does not appear to substantially change postoperatively, ideal candidates for this procedure would have pain as a main complaint and should be satisfied with their preoperative ROM.
This study has a number of limitations which should be considered. Overall, there were a limited number of articles (6) and included patients (25). Patient baseline demographics and PROMs were inconsistently reported, making comparisons across clinical series difficult. Furthermore, the included articles overall contained lower levels of evidence, and in the absence of large comparative series, making comparisons between different revision techniques can be difficult.
Conclusions
Our systematic review identified 6 articles that reported on the outcomes of ARGC for aseptic loosening after TSA. The included clinical series indicate that ARGC can improve pain and functional outcomes in appropriately selected patients. At present, patients undergoing ARGC appear to be older, have lower functional demands and may be at risk for medical complications with open revision. ARGC after TSA has a low rate of subsequent reoperation (8%) and has the potential to avoid some of the complications associated with open revision arthroplasty procedures. As a less-invasive arthroscopic technique, ARGC after TSA may be an alternative to open revision for lower demand patients; however, future prospective, comparative studies are necessary to better define indications and outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article