
Abstract
Background:
High rates of radiographic loosening have been reported with various glenoid designs. Many available designs sacrifice most of the bone at the central portion of the glenoid vault, creating large areas of deficiency when revision becomes necessary. The purpose of this study was to report the 2- to 5-year outcome of shoulder arthroplasty using a bone-preserving all-polyethylene glenoid components with self-pressurizing pegs.
Methods:
Between August 2011 and December 2014, 202 consecutive anatomic total shoulder arthroplasties (TSAs) were performed by a single surgeon with implantation of a self-pressurizing cemented pegged glenoid component in 190 patients (12 patients had both shoulders replaced). Patients were followed up prospectively and evaluated for pain, motion, strength, American Shoulder and Elbow Surgeons (ASES) scores, and radiographic changes. The mean follow-up time was 2.7 (2–5) years.
Results:
TSA improved pain and function reliably. At the most recent follow-up, 94% of the shoulders had no or mild pain. Motion included 154 ± 25° of elevation, 68 ± 18° of external rotation, and median internal rotation to T10 (range, iliac crest to T4). The most recent average ASES score was 82 ± 15 points. Early postoperative radiographs showed no radiolucent lines. No humeral or glenoid component was considered radiographically loose at the most recent follow-up. Complications requiring reoperation included subscapularis insufficiency (4), posterior instability (2), deep infection (1), stiffness (1), and a painful loose body (1). No components were revised for loosening.
Conclusions:
Anatomic TSA using a cemented bone-preserving all-polyethylene pegged self-pressurizing glenoid component provided satisfactory clinical outcomes and survival at 2 to 5 years.
Keywords
Introduction
Anatomic total shoulder arthroplasty (TSA) has been reported to provide good pain relief and improved function for various shoulder conditions.1–3 On the glenoid side, an all-polyethylene component is used most commonly. Although revision for loosening of all-polyethylene glenoid components has been reported to be relatively low with various designs, some authors have reported concerning high rates of radiographic failure.4–7 This seems to be especially true in young patients. 8
Controversy remains regarding the comparative performance of keeled versus pegged components. Some studies have shown the superiority of pegged components, 9–11 whereas other studies have shown no difference.12,13 It is important to note that several studies have reported on the performance of pegged components with three pegs in line, which biomechanically may behave similar to a keel. In a recent study by McLendon et al. on 330 anatomic shoulder arthroplasties with an in-line three peg component, the 10-year survival free of glenoid revision was 83%, but the 10-year survival free of radiographic loosening dropped to 43%.
Several factors have been associated with higher glenoid component failure rates, including younger age, component malposition, severe preoperative glenoid bone loss, excessive reaming, poor cementing technique (radiolucent lines present in the first postoperative radiograph), lack of mismatch between the radii of curvature of the glenoid and humeral head, and use of poor quality polyethylene.3–5, 8, 14–17 Several components have been designed with a large central peg made of polyethylene or metal to provide the opportunity for ingrowth.2,18 However, these components do use most of the bone in the central portion of the glenoid vault, leading to very large defects when they fail, which may severely complicate revision surgery. 19
Over the last 6 years, the senior author has used in his practice a bone-preserving highly cross-linked all-polyethylene component with self-pressurizing pegs. The purpose of this study was to report the 2- to 5-year outcome of anatomic TSA using this particular component in order to identify complications and reoperations.
Methods
Patients
Between August 2011 and December 2014, 202 consecutive anatomic TSAs were performed by a single surgeon with implantation of a self-pressurizing cemented pegged glenoid component (ReUnion, Stryker, Mahwah, NJ) in 190 patients (12 patients had both shoulders replaced). There were 90 females (5 bilateral) and 100 males (7 bilateral) with a mean age of 67 years (range, 24–93 years) at the time of surgery and a mean body mass index of 30.8 kg/m2 (range, 17.7–60.3 kg/m2). The underlying diagnosis was glenohumeral osteoarthritis in 176 shoulders, avascular necrosis of the humeral head in 14 shoulders, inflammatory arthritis in 6 shoulders, chondrolysis in 4 shoulders, and spondyloephiphyseal dysplasia in 2 shoulders.
Six shoulders were revised within the first 2 years after surgery. Three patients died within the first 2 years after surgery of reasons unrelated to their index shoulder arthoplasty (one of the deceased patients with bilateral shoulder arthroplasties had undergone revision surgery prior to death). Three additional patients were lost to follow-up (one of the patients lost to follow-up had both shoulders replaced). The remaining 189 shoulders were followed up for 2.7 years (range, 2–5 years). Complications and reoperations are reported for all 202 shoulders. Clinical results are reported for all shoulders with surviving implants and a minimum follow-up of 2 years.
Surgical Procedure
All procedures were performed by the same surgeon under general anesthesia with the use of an indwelling interscalenic catheter inserted prior to surgery and maintained for 24 h. All arthroplasties were performed in the beach chair position through a deltopectoral approach. Deep exposure was performed through a subscapularis tenotomy, repaired at the end of the procedure with multiple interrupted absorbable sutures. An effort was made to select the glenoid size based on the humeral head diameter to achieve a mismatch of 6 mm between the diameters of the articular surfaces of the humerus and glenoid. All humeral components were uncemented. All glenoid components were cemented using half a batch of polymethylmetacrylate. Vancomycin (1 g) and methylene blue (1 mL) were added to the polymethylmetacrylate at the time of cement mixing. Cement was applied in all peg holes. No drains were used at the end of the procedure. The mean operative time was 70 min (range, 41–120 min).
Implants
All arthroplasties were performed with the implantation of anatomic ReUnion components (Stryker). All humeral components were uncemented and proximally coated with hydroxyapatite. The stem geometry has a narrow anteroposterior cross-section to preserve proximal humerus bone. Primary stability is achieved by a combination of distal fit and an extended medial flare design that engages in the calcar region (Figure 1). The humeral canal was reamed distally line to line and underbroached proximally by 2 mm. Table 1 summarizes the diameter of the humeral stems implanted.
(a) Humeral component. (b) Implanted humeral component. Component Sizes for the 202 Shoulder Arthroplasties Included in the Study.

The glenoid component incorporates a number of design features (Table 2). The central peg is shorter than the peripheral pegs to preserve bone in the glenoid vault, whereas the peripheral pegs pressurize polymethylmetacrylate as they are impacted in their respective holes (Figure 2). Five sizes provide an automatic 6 mm diametrical mismatch when paired with humeral heads of the same numbering. Table 1 summarizes the glenoid sizes implanted in this study. As mentioned earlier, all glenoid components were fixed with vancomycin-impregnated polymethylethacrilate.
(a) Self-pressurizing pegged glenoid component. (b) Mechanism for cement self-pressurization. (c) Immediate postoperative radiographs shows complete absence of radiolucent lines at the implant–cement–bone interface. Glenoid Component Features.

Postoperarative Care
After surgery, all patients were recommended to use a shoulder immobilizer for the first 6 weeks postoperatively. Passive range of motion exercises in elevation and external rotation were initiated in postoperative day 1. Active-assisted range of motion exercises was initiated at week 7. Isometrics were added at week 10 and strengthening with elastic bands was added at week 12.
Clinical and Radiographic Evaluation
At our Institution, all patients undergoing arthroplasty are followed up prospectively using our Total Joint Registry database. 20 Data are collected preoperatively and at regular intervals including 2 years and 5 years postoperatively. At these respective follow-up times, patients are invited to return for a physical examination and radiographs. For those patients unable to return in person, data are collected using a mailed or telephone questionnaire and patients are requested to mail recent radiographs.
Pain is graded as none, mild, occasionally moderate, moderate, or severe. Motion is recorded in degrees for elevation and external rotation and as the highest vertebral level reached by the thumb for internal rotation. Strength is assessed manually using a 5-level scale (5 = normal, 4 = decreased but able to resist the examiner, 3 = decreased but able to resist gravity, 2 = visible contraction but unable to resist gravity, and 1 = paralysis). Complications and reoperations are recorded as well. Most recent results were also assessed using the ASES shoulder score.
The following radiographic projections are obtained: anteroposterior with the shoulder in external rotation, anteroposterior with the shoulder in internal rotation, axillary, and Y. Postoperative radiographs are evaluated for component position and the presence, thickness, and location of radiolucent lines. The humeral component was considered radiographically loose in the presence of implant subsidence, implant tilt, or a complete radiolucent line measuring more than 1 mm in zones 1 and 7 (Figure 3). The glenoid component was considered radiographically loose in the presence of implant migration, implant tilt, or a complete radiolucent line measuring at least 1 mm. Other radiographic complications were recorded as well.
(a) Humeral zones. (b) Glenoid zones. Clinical and radiographic outcome of one of the patients included in the study. (a) Preoperative radiograph. (b) Postoperative anteroposterior radiograph. (c) Postoperative axillary radiograph. (d) Elevation. (e) External rotation. (f) Internal rotation.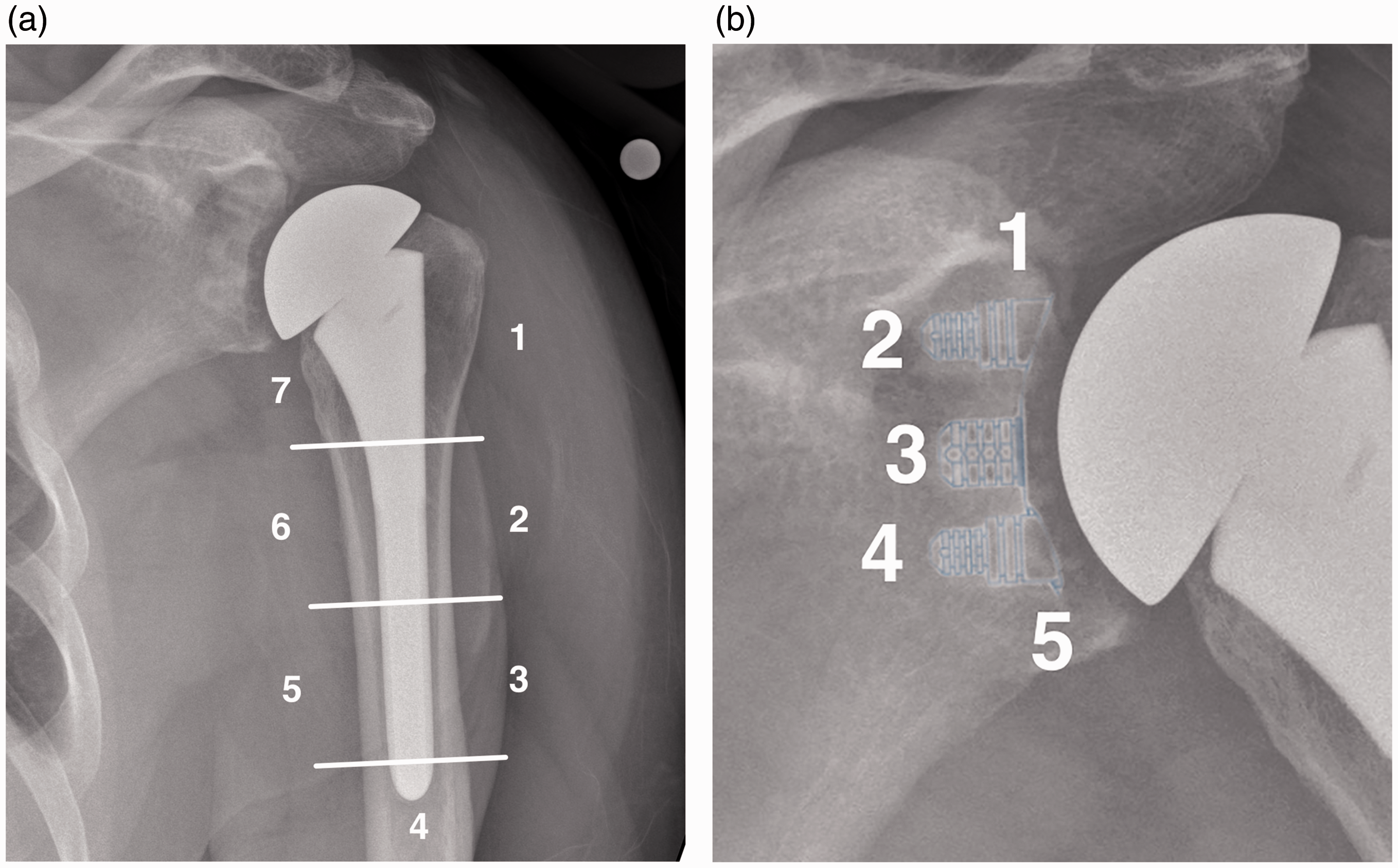

Results
Clinical Results
Anatomic TSA resulted in substantial improvements in pain, motion, and function. Before surgery, all shoulders were considered to be moderately or severely painful. For surviving shoulders with more than 2 years of clinical follow-up, pain was rated as none, mild, or occasionally moderate in 178 and moderate in 11 shoulders. At the most recent follow-up, average motion included 154 ± 25° (range, 50–170°) of elevation and 68 ± 18° (range, 0–90) of external rotation. The median internal rotation was to T10 (range, iliac crest to T4). Most recent strength measurements were 4.7 ± 0.6 for abduction, 4.9 ± 0.4 for external rotation, and 4.9 ± 0.4 for internal rotation. The most recent shoulder ASES score was 82 ± 15 points (range, 45–100).
Radiographic Results
No radiolucent lines could be identified in any of the 202 shoulders in the radiographs obtained 6 weeks postoperatively. At the most recent follow-up, 189 of the 193 surviving shoulders with a minimum 2-year clinical follow-up had recent radiographs. The mean radiographic follow-up time was 1.5 years (range, 3 months to 5 years). None of the humeral components were considered radiographically loose. No glenoid radiolucent lines could be identified on radiographs obtained at the time of most recent follow-up. No glenoid component was considered to have migrated or shifted. As such, no glenoid component was considered to be radiographically loose or at risk for loosening.
Complications and Reoperations
Complications Encountered.

Four shoulders underwent reoperation for symptomatic subscapularis insufficiency at 6 weeks (1), 6 months (2), and 1 year (1) postoperatively; subscapularis repair was attempted in one shoulder and failed. All four shoulders were revised to a reverse arthroplasty, maintaining the humeral stem. Two additional shoulders developed posterior instability and were revised to a reverse prosthesis. One shoulder developed a deep periprosthetic infection and was treated with a two-stage reimplantation. For these 7 shoulders, the humeral and glenoid components were considered well fixed at the time of revision or resection.
One shoulder with an underlying diagnosis of chondrolysis developed severe stiffness and was treated with arthroscopic contracture release 1.7 years after the index arthroplasty. Finally, one shoulder developed posterior pain after trauma; ultrasound evaluation and image-guided injections demonstrated the presence of a fractured posterior osteophyte, which was removed arthroscopically with complete resolution of symptoms.
Discussion
Anatomic TSA is considered a successful surgical procedure for various conditions affecting the glenohumeral joint.1–3,17,18 Improvements in pain and function are reliable. However, complications do happen to some individuals. In the early postoperative period, subscapularis insufficiency, shoulder instability, and deep infection are the main failure mechanisms. Later on, failure of the glenoid component seems to become the predominant failure modality. 16 Some studies have reported radiographic glenoid loosening rates ranging between 30% and 50% at 5 and 10 years, respectively.4–6
The results of our study seem to indicate that anatomic TSA performed using a cementless hydroxyapatite-coated humeral component and a bone-preserving self-pressurizing cemented all-polyethylene glenoid component is associated with excellent performance and survivorship at 2 to 5 years (Figure 4).
Several factors related to the glenoid component design have been associated with higher failure rates. Incomplete seating of the component, the presence of radiolucent lines in the early postoperative period, and a matched radius of curvature between the articular surfaces of the humeral head and glenoid are some of the factors commonly mentioned in the literature.3–5,8,14–17
Early radiolucent lines are considered to represent areas of poor component–cement–bone bonding as the result of interposed blood, fluid, or fibrous tissue. Areas of poor bonding are suspected to facilitate further debonding leading to component loosening.14,21,22 Different techniques have been developed to decrease the rate of early radiolucent lines, including suction applied to the glenoid vault and cement pressurization with instruments. The glenoid component analyzed in this study eliminates early radiolucent lines through a self-pressurizing peg design. The results of this study confirm the absence of radiolucent lines in the early postoperative period when this component is used.
Certain mismatch between the radii of curvature of the articulating surfaces of the glenoid component and the prosthetic humeral head has also been associated with improved radiographic performance.15,23 Six millimeters of diametrical mismatch were achieved by design in all shoulders included in the present study by matching the size of the glenoid component to the anticipated size of the humeral head. None of the glenoid components implanted in this series developed progressive radiolucent lines or were considered radiographically loose at the most recent follow-up. The importance of other design factors in the radiographic performance of this component—such as a curved back—and the manufacturing of the component with highly cross-linked polyethylene remain unclear.
Promising results have also been shown with the use of alternative modern all-polyethylene components with a large uncemented central peg.1,2,18 However, bone ingrowth on a polyethylene surface has been difficult to prove in other joints. In addition, a wide and long central peg requires sacrificing most of the central bone in the glenoid vault. This can be particularly relevant at the time of revision surgery. The results of our study seem to indicate that similar results may be obtained using a glenoid component that allows more bone preservation.
Nonimplant-related complications continue to occur after anatomic shoulder arthroplasty. As noted in other studies, subscapularis failure, prosthetic instability, and deep infection are among the most common modes of failure. They commonly require revision to a reverse arthroplasty, which may be facilitated by use of a so-called platform system and minimal bone loss on the glenoid side at the time of revision surgery. All seven shoulders revised in this study to a reverse arthroplasty could be performed maintaining the previously implanted stem and without the need for glenoid bone grafting.
Our study has a number of limitations. All procedures were performed by a single high-volume shoulder arthroplasty surgeon and the results may not be extrapolated to general community. Computed tomography was not used to assess radiolucent lines at the most recent follow-up. Radiographs at the most recent follow-up were available for most but not all of the patients included in the study. The strengths of the study include the use of the same surgical technique for all shoulders, the prospective collection of data, and the high quality of the radiographic follow-up.
Conclusion
Anatomic TSA using a cementless hydroxyapatite-coated humeral component and a cemented bone-preserving all-polyethylene pegged self-pressurizing glenoid component provided satisfactory clinical outcomes, with a low rate of mechanical complications, and excellent component survival at 2 to 5 years of follow-up.
Footnotes
Declaration of conflicting interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Sanchez-Sotelo royalties/Stryker; rest of the authors have no disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.