
Abstract
The location and course of the suprascapular nerve (SSN) to the glenohumeral joint places this nerve at risk when operating around the shoulder. Iatrogenic injury to the suprascapular nerve has been described in several different procedures including, rotator cuff repairs, posterior capsulorraphy, Bankart repairs, SLAP lesion repairs, Latarjet procedures, and shoulder arthroplasty. We present a case of iatrogenic suprascapular nerve injury due to superior glenoid baseplate screw placement following primary reverse shoulder arthroplasty (RSA), a novel approach to diagnosis of nerve injury, and treatment.
Keywords
Case Report
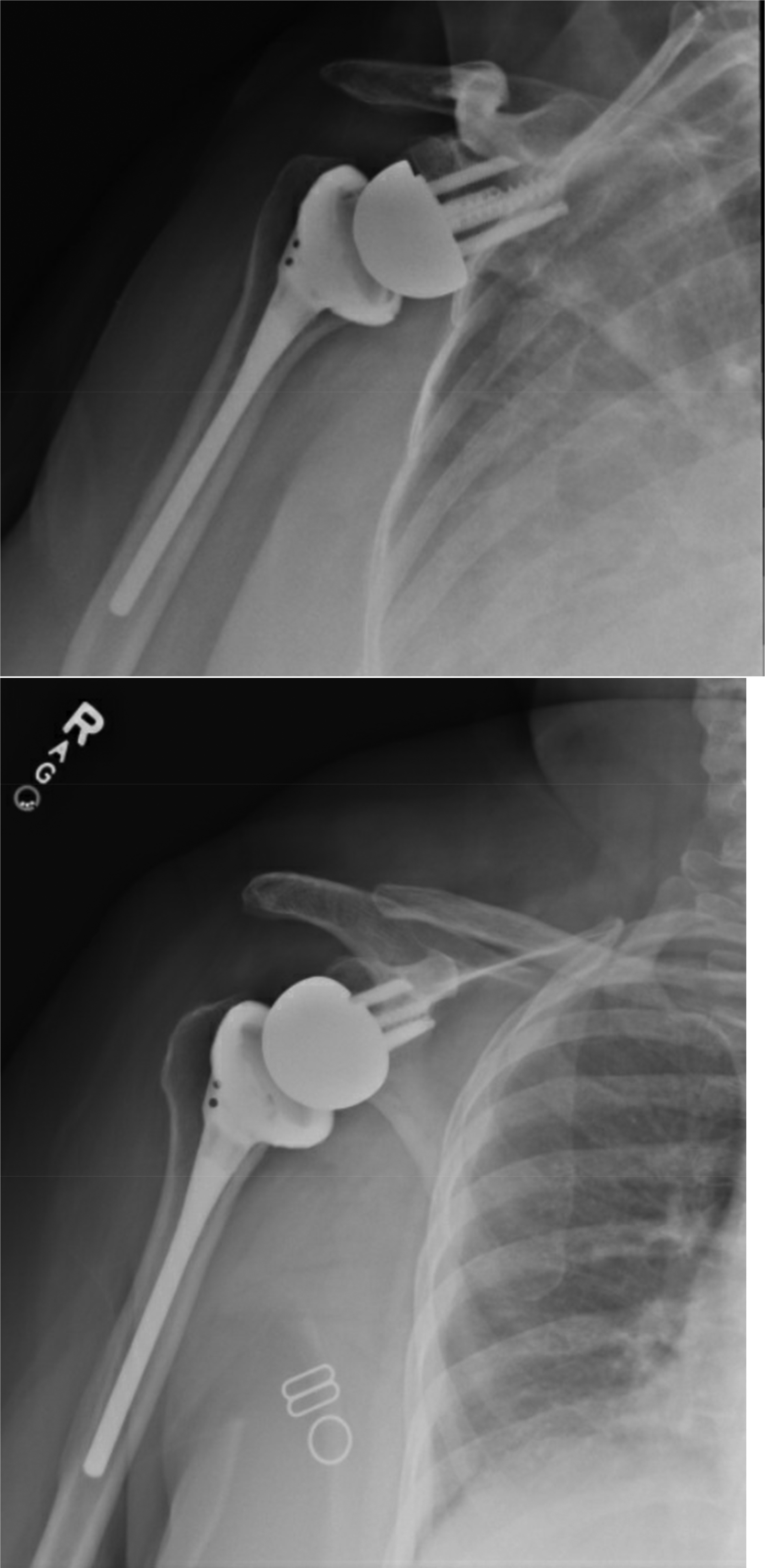
A 64 year old female underwent a right RSA procedure for rotator cuff arthropathy. Surgery was performed in the beach chair position utilizing ta standard deltopectoral approach. Bone allograft was used to augment the posterior glenoid. DJO (Encore Orthopaedics) Implants were utilized included a 30 mm screw-in base plate, 4 locking peripheral screws measuring 5 × 26 mm, 5 × 18 mm, 5 × 34 mm, 5 × 34 mm, a 36-4 mm glenosphere (placed with a 10 degree inferior tilt), and a size 6 humeral uncemented stem. Surgery was uncomplicated, and post-operative radiographs are shown in Figure 1.

Post-operative radiograph of right shoulder.
Post-operative course was uneventful until 4 months after the procedure when the patient noted 4/10 right shoulder pain. Pain was located superiorly without any precipitating event or injury. She described the pain as sharp and a “knot” localized to her distal acromion. On exam, tenderness to palpation was noted over her right distal acromion but was otherwise unremarkable. Shoulder radiographs (Figure 2), were negative for any complication. However, given the location and severity of her pain, she was presumed to have a stress fracture of the acromion. An abduction sling was provided, and she was instructed to continue with her passive range of motion as pain allows with FF limited to 90 degrees and return in 1 month for repeat radiographs.

Coronal CT image of right shoulder.
Patient returned to clinic routinely in the subsequent months, but interval history, exam, and imaging were unchanged. She continued to endorse pain in the superior aspect of her shoulder, starting near a “knot” about her acromion and extending laterally and anteriorly, which was made worse by any range of motion and activity. Patient had failed conservative management, which to this point included a sling, activity modification, bone stimulator, and calcium supplementation. At 10 months post operatively decision was made to obtain a CT scan of her right shoulder shown in Figure 2.
Radiologist report of the CT scan was unremarkable and revealed no hardware complication and incorporating bone graft. Given this information and the duration of the patient's symptoms, there was concern for possible infection. She therefore, underwent an infectious work up including C-Reactive Protein (CRP), Erythrocyte Sedimentation Rate (ESR), Complete Blood Count (CBC), and radiology guided joint aspiration to obtain synovial cell count, culture, gram stain, and crystals. However, infectious work up was unremarkable, and upon extensive review patient's many prior radiographs and recent CT, there was concern that the superior screw may have violated the spinoglenoid notch irritating the suprascapular nerve.
As a result, ultrasound exam and guided injection were ordered to assess whether the superior screw was the source of this patient's pain. Exam revealed a linear echogenic foci in the spinoglenoid notch corresponding to the screw from reverse arthroplasty glenoid component with CT correlate. A 3.5” 22-gauge spinal needle was inserted into the spinoglenoid notch and 4 cc of 0.5% ropivacaine was injected.
At follow up appointment a few days later, she noted complete pain resolution for 24 h after this injection. Given the recalcitrant nature of her pain, surgical options were discussed, including superior screw removal utilizing the patient's prior deltopectoral incision, complete glenoid revision, and burring of the screw through an approach along the scapular spine via a trapezius split and supraspinatus reflection.
Risks and benefits of these approaches were weighed with the patient. The risk of instability, and/or functional decline with a formal revision surgery to remove the superior were of concern. Furthermore, given the lack of posterior glenoid bone stock that required bone grafting, revision of the baseplate may also prove challenging, likely requiring additional augmentation via bone graft. Finally, if the superior screw were to be removed entirely, there was concern that this may compromise the glenoid baseplate. Therefore, the decision was made (now approximately 2 years from her index procedure) to undergo burring of the superior screw through an approach along the scapular spine via a trapezius split and supraspinatus reflection.
Surgery was performed in the lateral position. An incision was carried down along the spine of the scapula (Figure 3). The trapezius muscle was split and the fat was cauterized to the level of the spine. The scapular spine periosteum was then incised with electrocautery and elevated with a key elevator. The supraspinatus belly was then elevated. A Hohman retractor was passed on bone down to the supraspinatus fossa and over the anterior, superior edge of the scapula. The retractor was used to lift and elevate the supraspinatus muscle belly (Figure 4). At this point, visualization of the prominent screw was obtained (Figure 5). The transverse suprascapular ligament was released with cautery. The suprascapular artery and nerve were visualized traversing directly over the screw threads. The nerve and artery were then carefully retracted laterally and anteriorly and the screw was burred down with a metal cutting burr. At this point in time, a neurolysis of the suprascapular nerve was performed. Once the screw was burred down and flush with the bone, palpation confirmed a decompression of the nerve (Figure 6). Post-operative radiographs can be seen in Figure 7 which noted decreased prominence of the superior screw.

Operative picture - The incision for exposure of supraspinatus fossa is approximately 7 cm in length and centered just superior to the scapular spine. This longitudinal incision allows for easy elevation of the supraspinatus muscle belly and visualization of suprascapular notch, suprascapular ligament, suprascapular nerve, and prominent hardware.
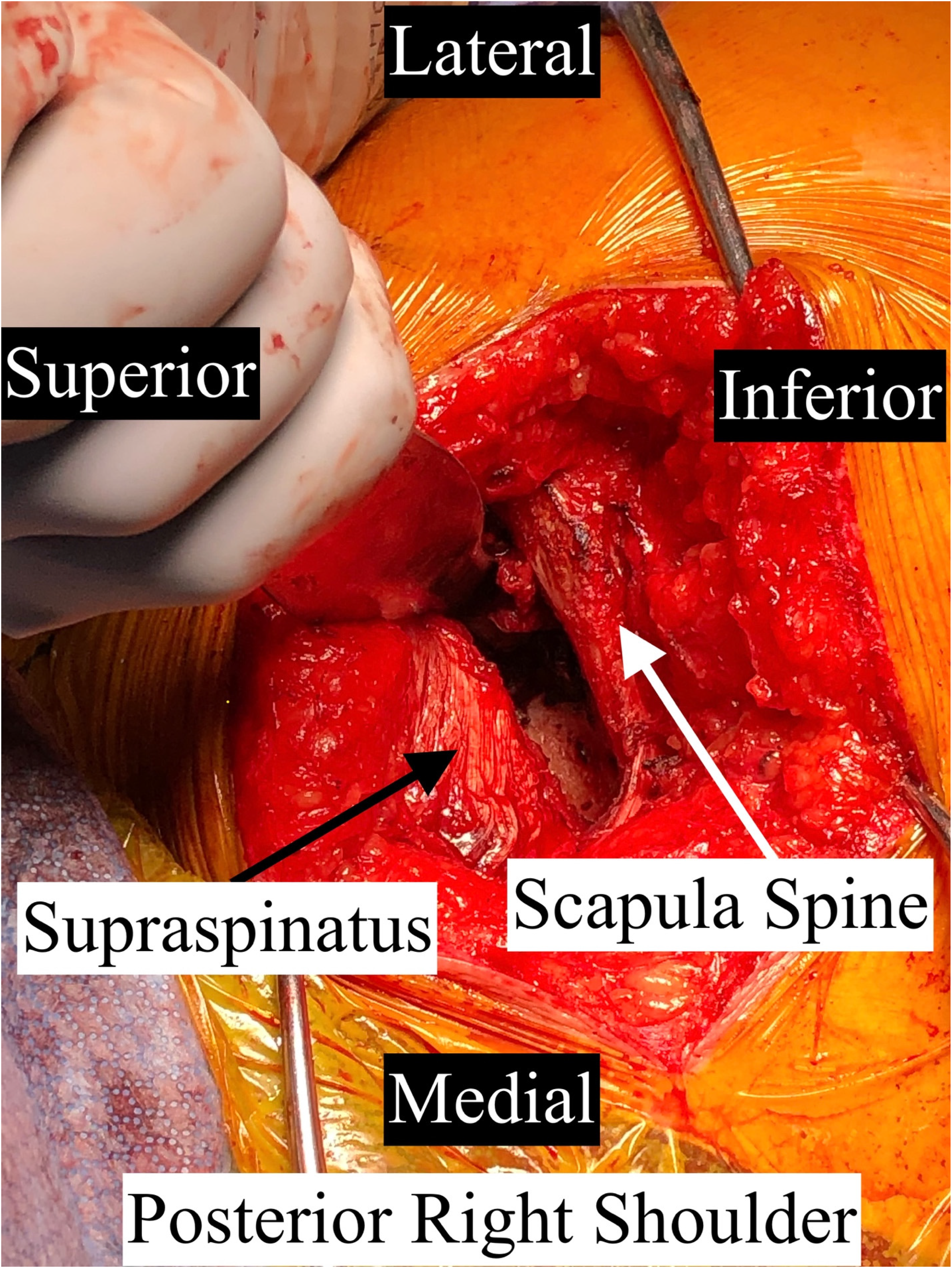
Operative picture - deep exposure of the supraspinatus fossa. The scapular spine is used as the main landmark to begin elevating the supraspinatus muscle belly, starting at the most distal, superior aspect of the scapular spine and elevating deep and towards midline. Care should be taken not to lacerate the suprascapular artery as you approach the suprascapular notch.

Operative picture - deep exposure of the supraspinatus fossa with visualization of prominent hardware, blue arrow. The suprascapular ligament, pink arrow, has been released for decompression of the suprascapular nerve, white arrow. The scapular spine is marked with a green arrow.

Operative picture - following hardware removal with a diamond tipped burr, the hardware is now below the cortical margin of the scapula, white arrow. The nerve was able to course around the lateral aspect of the scapular spine, black arrow, without continued bowstringing over the screw.
Post-operative radiographs of right shoulder.
At the initial, two week post-operative visit, the patient reported significant improvement in her pain. She denies experiencing the sharp pain and a “knot” localized to her distal acromion that she had previously described. The patient had begun attending physical therapy and had discontinued use of the sling. Overall, she was pleased with her results. Active forward flexion at that time was noted to be 130 degrees. Repeat shoulder radiographs confirmed screw decompression and stable hardware. At six months she reported complete resolution of her pain and return to her range of motion prior to her second surgery.
Discussion
We believe this case represents a novel approach to diagnosis and treatment of iatrogenic SSN from a baseplate screw following RSA and can help provided information and options for diagnosis and treatment for surgeons who encounter and work up patients with pain following RSA. Ultrasound guided injection should be considered for patients with clinical signs and symptoms of SSN injury. If patients demonstrate a response to the injection, surgeons can expect good clinical outcomes following removal of the prominent hardware.
The SSN arises from the upper trunk of the brachial plexus which is formed by C5 and C6. It provides both sensory and motor innervation to the shoulder, and it's course has been well described in the literature.1–4 The SSN branches off the upper trunk of the brachial plexus, passes across the posterior triangle of the neck parallel to the inferior belly of the omohyoid muscle and deep to the trapezius muscle. It then runs along the superior border of the scapula, passes through the suprascapular notch inferior to the superior transverse scapular ligament and enters the suprascapular fossa. Here the nerve provides motor branches to the supraspinatus muscle. As the SSN passes beneath the supraspinatus, it heads obliquely and laterally along the lateral border of the spine of the scapula, eventually reaching the spinogleniod notch at the base of the scapular spine. Here it passes underneath the inferior transverse scapular ligament and enters the infrascapular fossa. The nerve then curves medial providing motor branches to the infraspinatus muscle. Throughout its course, the SSN also provides sensory innervation to the subacromial bursa, acromioclavicular and coracoclavicular ligaments, as well as the posterior glenohumeral capsule. 5
The incidence of neurologic complications following reverse total shoulder arthroplasty has been reported to be anywhere from 0.6% - 3.6%.6,7 Knowing the course of the SSN allows the surgeon to know the areas at risk of iatrogenic injury. Common points of reference to know are the distance from the superior glenoid to the suprascapular notch and the distance of the posterior glenoid to the base of the scapular spine. These are known areas in which the SSN routinely travels and can be at risk during superior and posterior screw placement respectively. Anatomic studies have shown this distance from the superior glenoid to the suprascapular notch to be about 3 cm and the distance from the posterior glenoid to the base of the scapular spine to be about 2 cm.1,4 Based on this information, known danger zones have been described as areas where the SSN is at greatest risk. For a right shoulder this areas correspond to the two o’clock to eight o’clock positions, with the area of about eleven o’clock to two o’clock corresponding to screws directed at the suprascapular notch and the area from eleven o’clock to eight o’clock corresponding to screws directed at the base of the scapular spine. 4
In this case, the superior screw was found to violate spinoglenoid notch, injuring the SSN. Many factors could have contributed to this including the patient's anatomy and posterior glenoid wear. We believe that having an understanding the relationship between the glenoid and the SSN and knowledge of these danger zones could have helped the surgeon avoid iatrogenic injury to the SSN.
A case has been described by Wang et al of suprascapular nerve injury following reverse shoulder arthroplasty. 2 In that case work up included electromyography and CT scan with 3-dimensional (3D) reconstruction to confirm SSN injury. In this case, we utilized ultrasound exam and ultrasound guided injection in addition to CT to confirm malpositioning of the screw and that the SSN was the etiology of this patient's pain. A similar open surgical technique to nerve decompression was employed via an incision along the scapular spine followed by a trapezius split, reflection of the supraspinatus muscle belly, burring of the screw to maintain glenoid base plate stability, and finally nerve decompression.
Ultrasound guided exams and injections are commonly utilized to diagnose and treat nerve lesions, however targeting of the SSN is less common. It has been described in a few different orthopaedic settings including pain relief for patients with adhesive capsulitis, rotator cuff tears, rotator cuff tendonitis, nerve blocks during arthroscopy, and diagnosing compressive lesions about the SSN.8–15
Ultrasound guided exam and injection of the SSN in this setting of screw irritation may represent a more specific test than CT or CT with 3D reconstruction to diagnose iatrogenic injury to the SSN. Utilizing this modality may prevent patient from undergoing a prolonged, painful post-operative course and extensive unnecessary workup. For these reason in patients with concerns for iatrogenic SSN injury on imaging, unexpected postoperative pain, and clinical signs of SSN injury, we recommend consideration of an ultrasound guided injection to aid in diagnosis.
In this clinical scenario consideration could be given to screw removal, screw exchange, or glenoid baseplate revision. This would avoid an additional incision, possible muscle damage, metal debris, or further nerve injury. However complication rates following revision RSA are around 33% and may be has high as 70% if one includes all short term complications. 16 These include infection, glenoid loosening, instability, and dislocation to name a few. 17 Additionally, revision of the glenoid component is often times the most challenging part of revision RSA. The patient presented here had previously grafted posterior glenoid. CT imaging demonstrated graft incorporation, however there is always concern that revising the glenoid screw or baseplate may compromise the graft or glenoid bone stock which is of great concern during revision RSA. Furthermore, there is no ability through a deltopectoral approach to evaluate the SSN or perform neurolysis as was done in this case. As a result, we believe this technique offered this patient the most targeted treatment option, preventing the complications associated with complete screw removal and revision of the glenoid component.
Conclusion
We believe that this is the first case reported to utilize ultrasound guided exam and injection to confirm suprascapular nerve injury due to a malpositioned superior screw following reverse shoulder arthroplasty. Treatment was through an open approach along the scapular spine via a trapezius split and reflection of the supraspinatus muscle, followed by burring of the prominent screw and nerve decompression. Ultimately avoiding the morbidity associated with complete screw removal and revision arthroplasty, in addition to providing this patient with satisfactory results and significant pain relief.
Footnotes
Sources of Financial Biases
Christopher S. Klifto, MD is a consultant for Integra Life Sciences.
Author Contributions
Jason Long wrote the manuscript. Jordan Liles provided and edited the images for the manuscript. All authors reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.